
Abstract
Accidental injuries in the pediatric population are common. The response to injury also differs owing to anatomical and physiological differences in children. While such injuries carry a risk of lifelong morbidity, some cases may follow a benign course despite their distressing appearance. We report two cases of accidentally incurred penetrating trauma in the pediatric population with unusual objects, including a pencil and a toy wheel. Despite their intracranial extension, neither of the patients exhibited any discernible neurological deficits. Penetrating brain injuries require early removal and meticulous perioperative care to minimize the risk of long-term adverse neurological events in children.
Background
Penetrating brain injuries (PBI) occur when an object penetrates both the skull and the protective membranes, known as meninges that surround the brain. 1 Although they carry a risk of neurological deficits, rare cases exist in which patients may show no neurological impairments. 2 This is dependent on several factors such as object’s trajectory, affected brain regions, and individual neural adaptations. There are some anatomical and physiological differences in the adult and pediatric brains that account for the differences in their responses to injury. While the children’s scalp and soft tissues exert a poorer cushioning effect, their nerve fibers are more pliable and at a lesser risk of rupture from trauma. 3
Treatment for PBI depends on the severity and location of the injury as well as the associated symptoms. Antiepileptic drugs and antibiotic prophylaxis may be administered to manage symptoms and prevent complications. Surgical procedures are often necessary to remove foreign bodies, evacuate hematomas, and reduce post-injury edema. PBI frequently results in cerebrospinal fluid (CSF) leaks due to dural tears, which can be challenging to adequately seal through normal tissue healing processes at the entry or exit sites. 4
In this report, we present two cases of accidental PBI in pediatric patients. Both these cases occurred with objects of daily use, which are extremely rare objects that can cause head injury.
Case presentations
Case 1
A 3-year-old boy presented to the emergency department with a wooden pencil protruding from the superomedial aspect of his left orbit (Figure 1). The parents reported that the child fell forward while running with the object in his hand, thus sustaining the injury. However, the child remained alert and exhibited no neurological or ocular deficits. Extraocular movements were also intact. Computed tomography (CT) scan showed that the pencil penetrated the skull through the ethmoid bone with its tip at the inferomedial aspect of the ipsilateral frontal lobe, extending up to 5 cm. There was no surrounding hemorrhage or edema (Figures 2 and 3).

Triangular-shaped wooden pencil protruding through the left orbit beside the superomedial aspect of the globe.

(a) and (b) Preoperative computed tomography (CT) scan with pencil penetrating the skull through the ethmoid bone with its tip (arrow) at the inferomedial aspect of the ipsilateral frontal lobe, extending up to 5 cm. (c) Postoperative CT scan.

Preoperative computed tomography scan showing the relation between the tip of pencil and the cerebral vasculature.
The patient was transferred to the operating theater, where the pencil was removed under general anesthesia. A small linear skin incision was made adjacent to the entry point of the pencil, and part of the bone was cut away to free the penetrating object (Figure 4). The remaining pencil particles within the cavity were thoroughly washed out, and no CSF leakage was observed. The wound was closed, and a water-tight seal was ensured by applying fibrin glue.
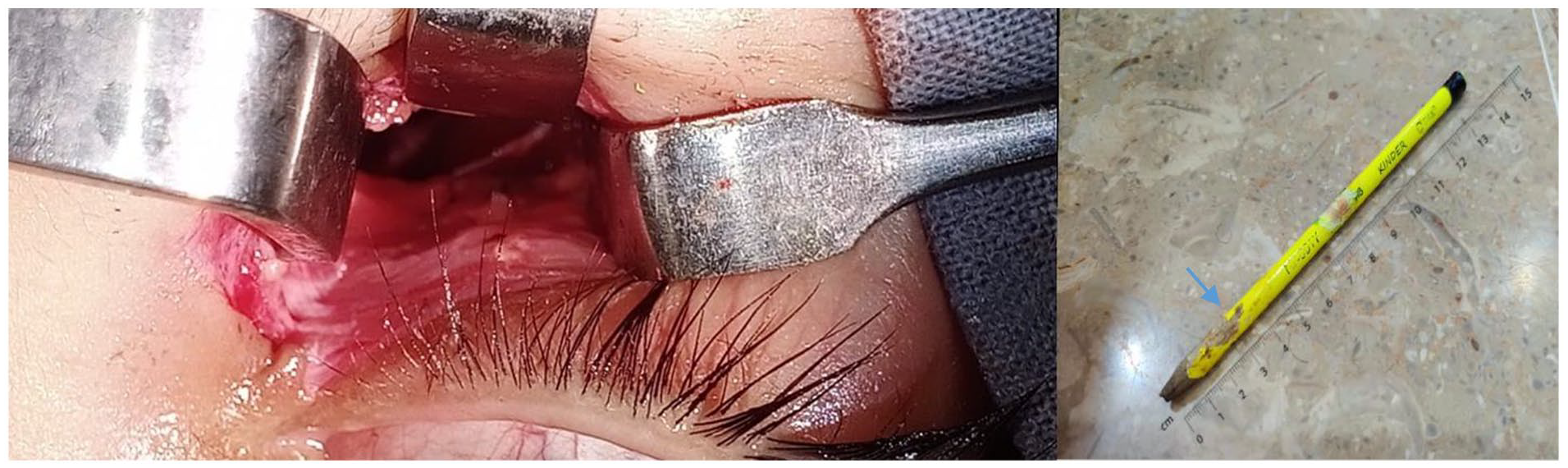
Perioperative imaging of the cavity after retrieving the pencil. A pencil was removed, inserted up to 3 cm (blue arrow).
Postoperatively, the child received intravenous antibiotics: ceftriaxone and metronidazole. In addition, intravenous antiepileptic prophylaxis with levetiracetam was administered. The patient showed a full recovery without any lasting neurological issues. On discharge on the seventh postoperative day, the child was prescribed oral cefixime to be taken every 12 h. A subsequent follow-up performed 2 weeks later was also unremarkable.
Case 2
A 19-month-old child was brought to the emergency room with a foreign body protruding from the back of his head, which was identified as a toy car wheel (Figure 5). The injury happened while the child was playing with his toys 2 h back. The child was well-oriented and calm with intact neurological function. There was no evidence of increased intracranial pressure.

(a) A toy wheel foreign body affected at the occipital area. (b) The metal artifact post Craniectomy.
His head CT revealed a linear hyperdense object with a metallic artifact in the left occipital area at a depth of approximately 1.5 cm without any evidence of infarction, acute intracranial hemorrhage, or mass effect (Figure 6). The child was taken to the operating theater and the toy car wheel was removed under general anesthesia in the right lateral position. A C-shaped skin flap was used for exposure, with 2 cm horizontal incisions made at each end. A burr hole was made near the bone defect; a 2 cm × 2 cm craniectomy was performed around the foreign body. Using Kerrison Rongeur forcep, the foreign body and the surrounding bone were removed intact slowly and carefully. Post-removal, bleeding from the posterior third of the superior sagittal sinus was managed by identifying and suturing bleeding points with Vicryl 5.0 running sutures, followed by the application of gel foam for hemostasis. The dura mater was then closed with interrupted sutures to ensure a watertight seal, and the overlying soft tissues were approximated. Given the size and location of the craniectomy defect, it was decided to leave it open rather than replacing the bone flap immediately.

(a) Preoperative computed tomography (CT) 3D reconstruction shows the visible object at the left occipital area. (b and c) Coronal cut CT (preoperative) exhibits a linear hyperdense object, 1.5 cm in depth, causing metallic streak artifacts at the affected left occipital area, indicative of infarct without evidence of acute intracranial hemorrhage or mass effect. (d) Postoperative 3D reconstruction following successful removal of the object. (e and f) Coronal cut CT (postoperative) illustrates the absence of the previously noted linear hyperdense object after the surgical procedure.
There were no postoperative complications. The child was kept on antibiotic ceftriaxone and metronidazole intravenously with antiepileptic prophylaxis with levetiracetam intravenously. He recovered without any residual neurological sequelae. The patient was discharged on seventh postoperative day with oral antibiotic cefixime 12 h. A subsequent follow-up after had intact neurological function, with no history of seizure.
Discussion
PBIs from objects of daily use are exceedingly rare. However, they carry the potential for severe neurological and ophthalmological complications. 5 This type of injury can give lead to a range of complications, including meningitis, cerebral abscess, intracerebral hemorrhage, and, particularly in children, long-term neurological dysfunction. 6 Fortunately, timely and appropriate management plays a crucial role in mitigating or preventing many of these complications.
Neurological damage associated with PBIs often presents as altered consciousness, seizures, or focal neurological deficits. Strikingly, some patients may display minimal or no symptoms. 2 In our cases, despite the distressing appearance of the injuries, the patients remarkably did not experience any neurological dysfunction.
The initial diagnostic tool in cases of PBIs is plain head CT scan, which serves as the primary imaging modality. 7 This scan is instrumental in assessing the extent of the injury and visualizing the trajectory of the penetrating object within the brain, which is crucial information for formulating the surgical plan. 8 In our first case, a transorbital approach was adopted because of the absence of hemorrhage on CT. Alternatively, more significant brain injuries may require a transcranial approach. Although CT angiography is recommended to rule out vascular damage, 1 it was not proceeded due to cost and time constraints. In addition, the absence of hemorrhage on the plain CT scan suggested that the tip of the toy car wheel was located away from major vascular structures, reducing the immediate risk of vascular injury or hemorrhage during removal.
The key aspect in managing PBIs lies in the removal of foreign bodies, as they not only induce direct tissue damage but also pose a risk of infection. Infections are the most lethal complications, with reported rates of 64%–70% and mortality rates ranging from 14% to 57%. 9 The British Society for Antimicrobial Therapy suggests the following treatment regimen for PBI: intravenous co-amoxiclav at a dose of 1.2 g every 8 h, or intravenous cefuroxime with an initial dose of 1.5 g followed by 750 mg every 8 h, along with intravenous metronidazole at a dose of 500 mg every 8 h. Alternatively, metronidazole can be administered rectally at a dose of 1 g every 12 h or orally at a dose of 400 mg every 8 h. 10 Antimicrobial prophylaxis was promptly initiated in both cases. This administration should start immediately after the injury and persist for 5 days postoperatively, maintaining prophylaxis for 7–14 days. 4 An illustrative case report by Al-Otaibi et al. 11 highlighted an occult transorbital penetrating injury caused by a pencil, resulting in an abscess and subdural empyema necessitating surgical drainage. The literature also documents rare instances of tattooing and the formation of pencil core granulomas as complications following pencil penetration. 12
Another notable concern in PBI cases revolves around the potential development of epilepsy, as scar tissue formation in the injured cortical tissue can precipitate seizures. Between 30% and 50% of patients with a PBI are at risk of developing seizures. 13 Approximately 10% may experience seizures within the first week following the trauma, with the majority (80%) occurring within the initial 2 years. 14 In addition, around 18% might not have their first seizure until 5 years or more post-injury. A case report by Lee and Lee 15 documented a 14-year-old girl with epilepsy attributed to a retained pencil. To mitigate the risk of posttraumatic epilepsy, the early initiation of antiepileptic drugs is recommended, with studies indicating that commencing anticonvulsant treatment within the first 7 days of the injury significantly diminishes the likelihood of epilepsy development. 16 For less severe injuries, it is considered acceptable to forego prophylactic anticonvulsant treatment entirely. In addition, the continued use of anticonvulsants beyond the first week post-injury is generally discouraged. 13
Time has emerged as a critical factor in the management and prognosis of PBIs. Timely surgical intervention is paramount for reducing the mortality rates associated with these injuries. As per current recommendations, surgical intervention should ideally occur within 12 h of the injury.17,18 Swift surgery has been linked to a mortality rate of approximately 33%. Conversely, delaying surgical intervention can substantially elevate the mortality rate to approximately 53%. 6 Therefore, minimizing the time gap between injury and surgical intervention is imperative for achieving better patient outcomes. Both of our cases underwent surgery within 12 h of arrival, immediately following the establishment of baseline labs and blood arrangement.
It is essential to recognize that the management of PBIs might exhibit slight variations across diverse regions and healthcare systems. Nevertheless, the core principles remain unwavering: swift imaging, thorough extraction of foreign bodies, administering suitable antibiotics, promptly initiating antiepileptic drugs, and ensuring that surgical intervention occurs without delay.
Conclusion
PBIs demand the utmost care and prompt management in trauma centers due to their potential for catastrophic outcomes. A comprehensive approach involving skilled specialists, advanced imaging, and timely surgical intervention is crucial for optimizing patient outcomes and minimizing the long-term sequelae associated with these injuries.
Footnotes
Author contributions
S.S., A.K.: Conception and design; S.S., S.A., A.B.A.: Acquisition of data; M.S.S., S.M.F.Z.: Drafting of the manuscript; F.A., A.A.K., I.A.S.: Critical revision for important intellectual content; M.S.S., S.M.F.Z., S.S., A.K., A.A.K., I.A.S., F.A., A.B.A., S.A.: Final approval of the study.
Availability of data and materials
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.