
Abstract
Introduction:
The frequency of breast cancer in young women, corresponding to women under 40 years of age; varies from 5% to 7% in developed countries. The objective of this study was to contribute to the improvement of the management of breast cancer in young women in Togo, by establishing the molecular classification of these cancers.
Methodology:
This was a retrospective descriptive and analytical study from January 2010 to December 2020.
Results:
About 35 cases of breast cancer were identified in women under 40 years of age. The average age was 35.4 ± 3.5 years. The right breast was affected in 18 cases (51.43%). Histologically, 30 cases (85.72%) were invasive carcinoma of no special type (NST), 2 cases (5.71%) were invasive lobular carcinoma and micro-papillary carcinoma respectively, and 1 case (2.86%) was tubular carcinoma. There were 6 cases (17.1%) of grade I, 25 cases (71.4%) of grade II, and 4 cases (11.4%) of grade III. Molecularly, there were 20 cases (57.1%) of triple-negative subtype, 6 cases (17.1%) of Luminal B subtype, 05 cases (14.3%) of HER2-enriched subtype and 4 cases (11.4%) of Luminal A subtype.
Conclusion:
Breast cancers of young Togolese women express very weakly hormone receptors, with a predominance of a triple negative subtype.
Introduction
Globally, breast cancer is the most common cancer in women, and it is estimated that its incidence and mortality rate will increase significantly over the next 5 to 10 years. 1 In 2020, more than 2.3 million new cases of breast cancer were diagnosed worldwide, accounting for 11.7% of all cancers, surpassing lung cancer in terms of incidence in both sexes. 2 It is also the leading cause of cancer death in women. 2 In the literature, the definition of a young woman is not univocal. 3 A young woman is either a woman under 35 years of age, a woman under 40 years of age, or simply a pre-menopausal woman.3 -6 However, the World Health Organization defines a young woman as a female aged 35 years or less. 5 The frequency of breast cancer in young women varies from 5% to 7% in developed countries. 7 In the USA, breast cancer occurs in 4% to 5.6% of women under the age of 40.3,8 The frequency of breast cancer in France is 7% in women under 40 years of age.6,9 In less developed regions such as Africa and the Middle East, where screening is not systematic and populations are on average much younger, a higher proportion of patients are diagnosed before the age of 40, up to 20%. 10 Research is underway to determine whether there are underlying genetic or environmental factors that make women in Africa and the Middle East more likely to develop breast cancer at a young age. 11 In Africa, there is regional variability in the incidence of breast cancer in young women of 10% to 12%.12 -14 In Ivory Coast, nearly 27% of breast cancers are diagnosed before the age of 40. 15 Breast cancers in young women are considered to have a worse prognosis, which has long justified more aggressive therapeutic management in terms of adjuvant or neoadjuvant chemotherapy.6,16 However, many studies have shown that there is no statistically significant correlation between the age of onset of these cancers and their molecular profile.3,4,6,8,9 Nevertheless, Luminal B HER2-negative cancers tend to be the most frequent and HER2-enriched, triple-negative cancers appear to be increasingly common.6,7,9 A study conducted in 2016 on the epidemiology of cancer in Togo had shown that breast cancer occupied the first rank and represented 21.2% of female cancers. These cancers occurred in 38.3% of women under 40 years of age. 17
The objective of this study was to contribute to the improvement of breast cancer management in young women in Togo, by establishing their molecular profile.
Methodology
This was a retrospective, descriptive, and analytical study from January 1, 2010 to December 31, 2020, a period of 10 years. The data were collected from the registers of the anatomical pathology laboratory of the Teaching Hospital of Lomé. From these registers, patients under 40 years of age, diagnosed with primary invasive carcinoma of the breast were selected and their blocks were selected for immunohistochemical examination. The technical part of the immunohistochemical examination was performed in the pathology laboratory of the Teaching Hospital of Cocody in Abidjan. The data collected concerned sociodemographic data (frequency, age, laterality) and anatomopathological data (nature of the sample, histological type, Nottingham grade, expression of hormone receptors and HER2 oncoprotein). Our study did not include cases of local recurrence or blocks that were available but not immunohistochemically exploitable.
Immunohistochemical analysis was performed on the 3 µm thick tissue sections. These tissue sections were heated in the BINDER® drying oven (BINDER company, Tuttlingen, Germany) for at least 12 hours at a temperature of 60°C to unmask the antigenic sites. Then, the determination of ER and PR expression, Human Epidermal Growth Factor Receptor (HER) 2 oncoprotein overexpression analysis on these tissue sections were processed by Ventana BenchMark® GX apparatus in automatic mode (Ventana Medical Systems Inc, Tucson, AZ, USA). The antibody clones used were monoclonal, developed in rats, consisting of SP1 for ER, 1E2 for PR and 4B5 for HER 2.
The Chi-square test was used to analyze the correlations between the molecular subtypes of breast cancer and the classical clinico-pathological factors (age, laterality, histological type, and Nottingham grade). A probability value P < .05 was considered statistically significant. Light microscopic analysis assessed the percentage and intensity of labeling of tumor cells showing nuclear labeling for ER and PR (0%-100%). Breast tissue sections were considered positive for ER and PR if more than 1% of invasive tumor cell nuclei were labeled. The HER 2 score was based on the intensity and percentage of invasive tumor cells positive for membrane labeling on a scale of 0 to 3+. 18 Slides immunostained with ER, PR, and HER 2 antibodies were independently evaluated by 2 pathologists. Thus, these cancers were classified into 4 molecular subtypes as follows:
- Luminal A; ER (+)/PR (+)/Her2 (−)
- Luminal B; ER (+)/PR (+/−)/Her2 (+) or RO(+)/Her2(−)/PR (−)
- HER2 enriched; ER (−)/PR (−)/Her2 (+)
- Triple negative; ER (−)/PR (−)/Her2 (−).
Results
Epidemiological data
A total of 804 cases of breast cancer in women were collected, including 35 cases in women under 40 years of age, that is, a frequency of 4.35%. The mean age of the patients was 35.4 ± 3.5 years with extremes of 27 and 39 years. According to laterality, there were 17 cases (48.57%) in the left breast and 18 cases (51.43%) in the right breast.
Histopathological data
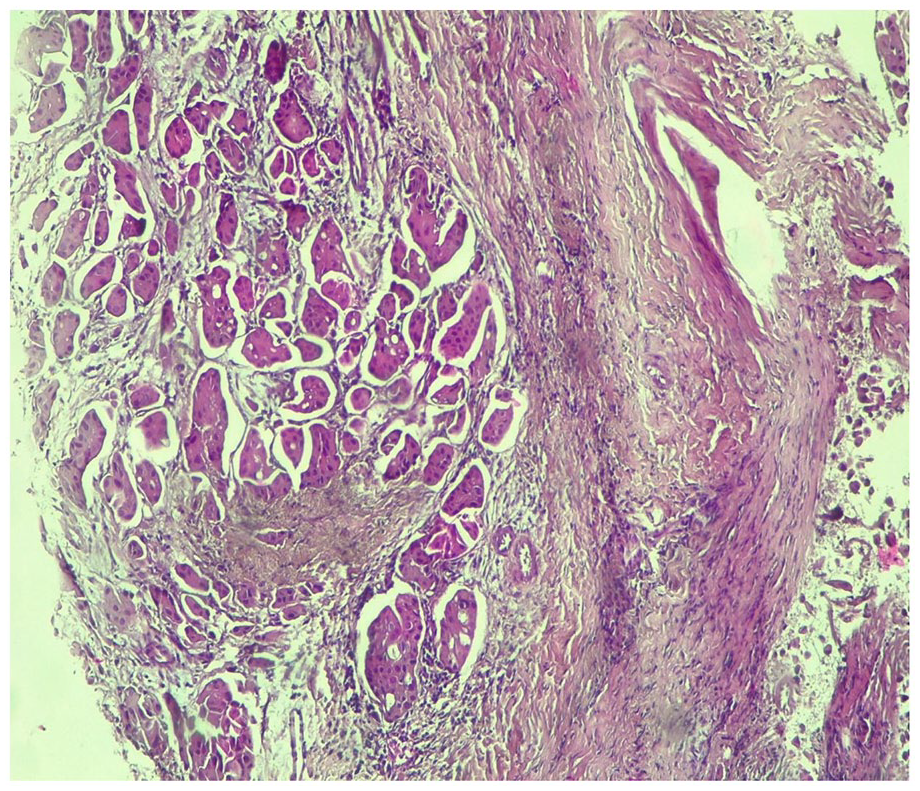
The diagnosis was made on biopsy in 11 cases (31.43%) and on surgical parts in 24 cases (68.57%). The surgical parts consisted of 11 cases of breast nodes, 7 cases of lumpectomy, and 6 cases of mastectomy. Invasive carcinoma of no special type (NST) was present in 30 cases (86%), followed by 2 cases (06%) of invasive lobular carcinoma and micropapillary carcinoma respectively, and 1 case of tubular carcinoma (Figures 1 and 2). These carcinomas were grade II in 25 cases (71.4%), grade I in 6 cases (17.2%), and grade III in 4 cases (11.4%).

Immunohistochemical data
The breast carcinomas presented by our patient expressed estrogen receptor in 10 cases (28.57%) and progesterone receptor in 8 cases (22.86%). Overexpression of HER2 oncoprotein was found in 8 cases (22.86%). No cases of breast carcinoma had an equivocal status (Figures 3 and 4).


Molecularly, there were 20 cases (57.1%) of triple-negative subtype, 6 cases (17.1%) of Luminal B subtype, 5 cases (14.3%) of HER2-enriched subtype, and 4 cases (11.4%) of Luminal A subtype.
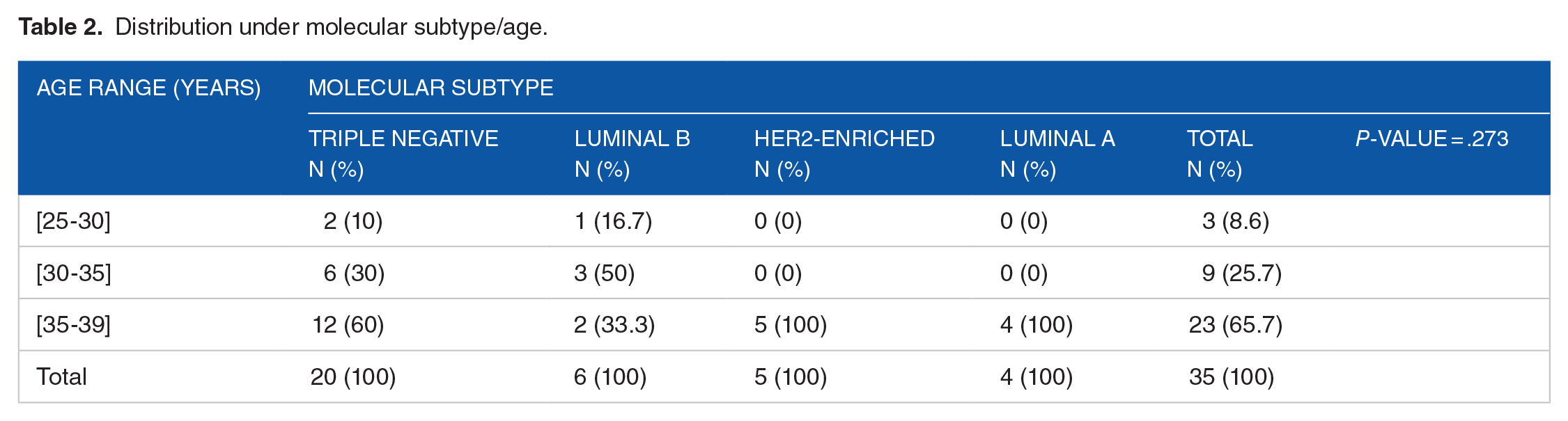
There was a statistically significant relationship between molecular subtype and histological type (P-value = 4.88 × 10−16) (Table 1). On the other hand, there was no statistically significant association between molecular subtype and age (P-value = .273) (Table 2), laterality (P-value = 1), nature of the specimen (P-value = .34) (Table 3), and histopronostic grade (P-value = .4235) (Table 4).
Distribution of molecular subtype/histological type.

Abbreviation: CINS, invasive carcinoma of no special type (NST).
Distribution under molecular subtype/age.
Distribution by molecular subtype/type of sample.

Molecular subtype/Nottingham grade distribution.

Discussion
Epidemiological data
We found a frequency of 4.35% of breast cancer in young Togolese women. This frequency is clearly lower than that of other African series and is comparable to that of developed countries. Indeed, the frequency of breast cancer in young women is 12% in Burkina Faso, 11% and 10%, respectively, in Tunisia and Morocco.12,14,19 It varies from 5% to 7% in developed countries. 7 This frequency of breast cancer in young women in Togo, probably underestimated, could be related to the under-medicalization of the health system, the geographical and financial inaccessibility of health care facilities, difficulties of diagnosis, and the shortage of pathologists and oncologists. The average age of our patients was 35.4 ± 3.5 years. Similar mean ages were found by Azim and Partridge (36 years) and Bennis et al (35 years).7,19 The impact of age on the prognosis of breast cancer is controversial. Some studies consider very young age as a significant negative predictive factor for survival, others suggest no effect of young age on prognosis.3,6,20,21 The majority of cancers were located in the right breast (51.43%). This predominance of cancer location in the right breast was found in the study of Erić et al. 22
Histopathological data
Invasive carcinoma of no special type (NST) was the most represented histological type (85.72%). Invasive carcinoma of no special type (NST) remains the most common histological type of breast cancer in young women in the literature.3,7,14,22 These cancers were predominantly grade II (71.43%). Walsh et al and Lamien-Sanou et al also found a predominance of grade II.4,14 Grade III was predominant in the study by Copson et al . 23 Regarding the Elston and Ellis grade of tumors presented by young patients, a significantly higher number of grade III tumors in young women was noted in the literature.6,24 -26
Immunohistochemical data
The breast carcinomas presented by our patient had low hormone receptor positivity rates; 28.57% and 22.86% for estrogen receptor (ER) and progesterone receptor (PR) respectively. These hormone receptor positivity rates are significantly lower than those of other African series. In Burkina Faso, Lamien-Sanou et al found positive estrogen and progesterone receptors in 55.26% and 39.47% of cases, respectively. 14 Jedidi et al found positive estrogen receptors in 47.7% of cases and positive progesterone receptors in 63.6% of cases. 27 The high rate of breast carcinomas not expressing hormone receptors in our study could be explained by an long fixation time in formalin (more than 72 hours), as well as a high melting temperature of the kerosene during the standard histological technique, leading to a destruction of the antigenic sites, responsible for false negative results. Overexpression of the HER2 oncoprotein was found in 8 cases (22.86%). This rate of HER2 oncoprotein overexpression is similar to that found by Lamien-Sanou et al (18.42%) and El Gnaoui et al (17%).14,28 In the literature, overexpression of HER2 oncoprotein is more important in young women. Anders et al reported a positivity rate of 29% in women under 40 years of age compared to 22% in patients under 45 years of age and only 14% in those over 65 years of age. 29
From a molecular point of view, the triple negative subtype was predominant (57.1%). Lamien-Sanou et al 14 also found a predominance of the triple-negative subtype in 29.41%. Darré et al 30 found a predominance of the Luminal B subtype (40.85%) in the general Togolese female population, with the triple-negative subtype representing only 14.08%. According to the literature, Luminal B tumors tend to be slightly more frequent and triple-negative HER2-enriched tumors appear more frequent.6,24,31 We did not find a statistically significant correlation between molecular profile and age (P-value = .273). On the other hand, there was a statistically significant relationship between the molecular profile and the histological type (P-value = 4.88 × 10−16). The high rate of breast carcinomas not expressing hormone receptors in our study could be explained by an often long fixation time in formalin (more than 72 hours), as well as a high melting temperature of the kerosene during the standard histological technique, leading to a destruction of antigenic sites, responsible for false negative results.
Women <40 years are more likely to develop breast cancer with worse clinicopathological features and more aggressive subtype. This has been frequently associated with inferior outcomes. Recently, the prognostic significance of age <40 has been shown to differ according to the breast cancer subtype, being associated with worst recurrence-free survival and overall survival for luminal breast cancer. 32 The indications for and the choice of systemic treatment for invasive breast cancer (both early and advanced disease) should not be based on age alone but driven by the biological characteristics of the individual tumor. 33
Limitations of the study
The main difficulties encountered in this study were common to all retrospective studies. Indeed, some of the information sought, such as age and nature of the sample, was not always found in the registers. We were also confronted with the problem of the duration of fixation of the samples in formalin, which was often too long, as well as with the difficulties of conservation of the blocks.
Conclusion
Breast cancer in young women, long underestimated, remains a daily problem in young Togolese women. Invasive carcinoma of no special type (NST) remains the most diagnosed histological type. Regarding the Elston and Ellis grade of the tumors presented by these young patients, we note a predominance of grade II. At the molecular level, these tumors express hormone receptors very weakly, with a clear predominance of the triple negative subtype. This is indicative of the very aggressive nature of breast cancer in this age group, which is emphasized in the literature. Studies on a more representative sample, with respect to preanalytical conditions, are desirable to establish the real molecular profile of breast cancer in Togolese women.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
TDj performed the laboratory analyses and their interpretation and drafted the manuscript. BK, PS, BMS, MB, and BD participated in the management of the specimens; reviewed the manuscript. TD is responsible for the overall scientific management, revised and finalized the manuscript. All authors have read and approved the final version of the manuscript to be submitted for publication.
Availability of Data and Materials
All data supporting the conclusions of this article are included in the manuscript and its supporting documents.
Ethical Approval and Consent to Participate
The study received approval from the head of the laboratory to be conducted. Due to the retrospective nature of the study, it was not possible to have the patients sign a consent form. However, the data were collected anonymously. The manuscript was not submitted to more than one journal for simultaneous review and has not been previously published. Single study, not divided into multiple parts and no data were generated.
Consent for Publication
The Department of Pathology of the University Hospital of Lomé has authorized the publication of this manuscript (Ref No. 18/2019/LAP/CHUSO).