
Abstract
Metaplastic breast carcinoma (MBCs) is a rare heterogeneous group of malignancies. Herein, we report a case of metaplastic breast carcinoma, which had 2 components. One of them was typical invasive ductal carcinoma (IDC), the other one was presenting as osteosarcoma with lots of immature trabeculae. The results of immunohistochemistry showed different presentations between them. The majority of MBCs show triple-negativity for ER, PR, and HER-2 and are thus associated with poor prognosis. Our report shows that, it is necessary to describe the proportion of the components and the presentations of immunohistochemistry in the diagnosis, which will be important to develop specific and effective therapies.
Introduction
Metaplastic breast carcinomas (MBC) comprise less than 1% of all breast cancers. The majority of MBCs show triple-negativity for ER, PR, and HER-2, therefore, they are associated with poor prognosis. Histopathological subtyping of MBC is complex, and may be characterized by differentiation of the invasive epithelium, which may be along squamous, spindle, mesenchymal, and other lineages. Osseous differentiation included in mesenchymal, is quite rare in breast metaplastic carcinoma.1,2 Herein, we report a case of metaplastic breast carcinoma with osseous differentiation.
Case Report
The case is about a 42-year-old woman, who complained of a painful mass of her right breast. The mammography demonstrated a high-density mass lesion of size 2.7 × 2.2 × 1.7 cm, which was presented not well-circumscribed, irregular borders (Figure 1). The mass showed heterogeneous calcification. For making pathological diagnosis of the mass, core needle biopsy was taken. The histopathology of the tumor was intriguing, because there were 2 different components in the tumor. One of them was typical invasive ductal carcinoma (IDC) (Figure 2), the other one was presenting as osteosarcoma. Lots of immature trabeculae could be seen, and atypia osteocytes among them (Figure 3). The results of immunohistochemistry showed different presentations between them. The IDC parts of the tumor was positive for ER, PR, and CK8/18, but the osteosarcoma was negative for ER, PR, and Her-2. The component of osteosarcoma expressed SATB-2 (Figure 4). The patient underwent the radical operation of the lump. The gross appearance of the tumor revealed a solid mass with hemorrhagic (Figure 5). The mass was too firm to make the sections, so it was been decalcified. Routine microscopic examination revealed an invasive biphasic tumor comprising malignant epithelial and osseous tissue. It was the same as the histopathology of the core needle biopsy, as well as the results of immunohistochemistry. The final diagnosis was given, that was breast mixed metaplastic carcinoma, which was display a mixture of osteosarcoma (65%), with invasive ductal carcinoma (35%).

Mammogram of the mass, showed heterogeneous calcification, and irregular borders.
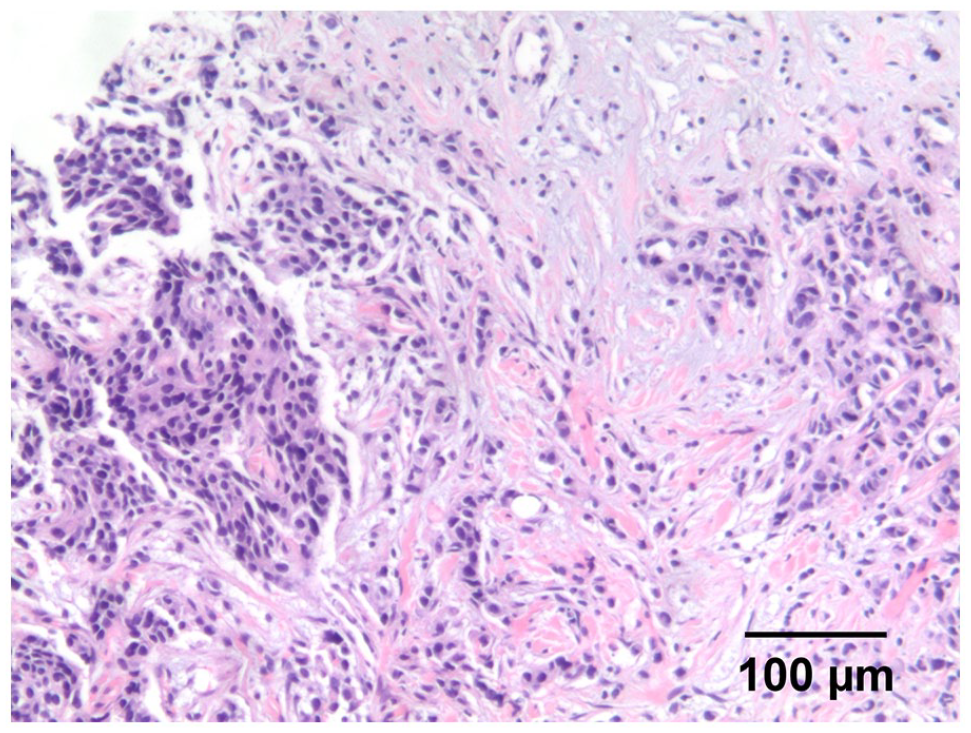
This picture showed the component of typical invasive ductal carcinoma.

This picture showed the component of osteosarcomatous differentiation.

This picture showed the result of immunohistochemistry, the osteosarcomatous part is positive for SATB-2 (monoclonal antibody, Zhongshan Bio), the nuclear staining brown.

The gross image of the tumor, showed the cut surface is solid-cystic, hemorrhagic, and firm.
Discussion
Metaplastic breast carcinoma is a heterogeneous group of malignancies that can exhibit multiple morphologies, which account for approximately 1% of breast tumors. These tumors have unique pathologic features, as their glandular component maybe partially or totally replaced by nonglandular component(s), which may differentiate along squamous, spindle cells, mesenchymal, and other lineages.
Carcinomas with mesenchymal differentiation are composed of an admixture of differentiated mesenchymal components, including chondroid, osseous, rhabdomyoid, and rarely neuroglial elements. Most commonly seen is an admixture of cartilaginous and osseous differentiation. The heterologous components can show a wide spectrum of atypia, ranging from bland to overtly malignant.2,3
There were many studies about metaplastic breast carcinoma, some of them were fours on which with mesenchymal morphology. One lecture from India, showed that 13 (2.5%) out of total 510 breast specimens presented mesenchymal differentiation, but none of them with osseous. 4 The other study from Australia showed 14 cases of metaplastic breast carcinoma, only 2 of them with mesenchymal differentiation, none of them with osseous, either. There is only 1 case report about MBC with osseous. 5
It is difficult to diagnose, because of the limitations of materials, especially by core biopsy. Fortunately, the case in our report whose pathological sections present 2 different components of the tumor, either by core biopsy or by biopsy specimens. One component is invasive ductal carcinoma, and the other one is osteosarcoma. 6 The 2 parts of the tumor appear simultaneously, that reminded us to make a diagnosis of MBC. Most of the other cases in earlier reports, which with osseous differentiation, osteoclast-type tumor giant cells often could be seen. In our case, a lot of immature trabeculae could be noted, that is quite rare.
Immunohistochemical confirmation of tumor epithelial component is necessary for the diagnosis of metaplastic carcinoma. Most of the MBCs demonstrate immunopositivity for p63 and CK, which distinguishes them from fibromatosis.2,6 Our case showed immunopositive for CK8/18 in the component of epithelial, and also exhibited estrogen and progesterone receptor positive in them. Conversely, in the element of osteosarcoma, they are negative, including HER-2, just like other studies of MBCs. So triple-negativity for ER, PR, and HER-2 may be a feature of mesenchymal components, not for the whole tumor. We described different presentations of immunohistochemistry in different component, to expect helping therapy.7,8 SATB2 is a marker of osteoblastic differentiation in bone tumors. 9 So the positive of SATB2 confirmed osseous differentiation of the tumor.
Conclusion
Histological examination of the tumor must be comprehensive, the glandular components and the mesenchymal components of the tumor are both hoped to be found to help making the diagnosis. If the glandular component were totally replaced by nonglandular component(s), it is difficult to named tumor. Most of the MBCs was known as triple-negativity for immunohistochemistry, but our case shows different presentations in 2 components. So it is necessary to describe the proportion of the components and the presentations of immunohistochemistry in the diagnosis, which will be important to develop specific and effective therapies.
The patient we fours on, after taken the operation, has completed the entire process of chemotherapy (8 cycles). During 20 months follow-up, the patient is still alive without relapse.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Tianjin Key Medical Discipline(Speciality) Construction Project.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Yang Xue: Performed the data analysis and wrote the manuscript. Chen Ling: Helped perform the analysis with constructive discussions. Shen Yan: Contributed to the conception of the study.