
Abstract
Background:
The Female Sexual Function Index (FSFI) is an internationally validated multidimensional self-report instrument for assessing female sexual function across six domains. Despite its widespread use, a psychometrically validated Hindi version has not been available for application among Hindi-speaking women in India, where sexual dysfunction remains underdiagnosed.
Aim:
This study aimed to perform a rigorous translation, cultural adaptation, and psychometric validation of the Hindi version of the FSFI (FSFI-H).
Methods:
The original FSFI was translated into Hindi using a standardized forward-backward translation protocol recommended by the World Health Organization (WHO), followed by expert panel review and cognitive debriefing in a pilot sample. A cross-sectional validation study was conducted among 200 sexually active, Hindi-speaking women aged 18–50 years attending a tertiary gynecology outpatient clinic. Internal consistency was evaluated using Cronbach’s alpha. Test-retest reliability over a two-week interval was assessed in a subsample (n = 40) using the intraclass correlation coefficient (ICC).
Results:
The FSFI-H demonstrated excellent internal consistency (Cronbach’s α = 0.89), with subscale alphas ranging from 0.78 to 0.92. Test-retest reliability was strong (ICC = 0.91; 95% CI: 0.87–0.94). Exploratory factor analysis (EFA) revealed a six-factor structure consistent with the original FSFI domains, accounting for 78.2% of the total variance. Known-groups validity was confirmed by significantly lower total FSFI-H scores among women with diagnosed sexual dysfunction compared to controls (mean ± SD: 19.3 ± 4.6 vs. 27.7 ± 3.8; P < .001; Cohen’s d = 2.01).
Conclusion:
The FSFI-H is a psychometrically sound instrument for assessing female sexual function in Hindi-speaking populations. The FSFI-H is a psychometrically sound and culturally appropriate instrument for assessing female sexual function in Hindi-speaking populations and can be reliably used for clinical screening, epidemiological research, and outcome assessment in Indian women.
Keywords
Introduction
Sexual health is a fundamental component of overall health and well-being and has been formally recognized by the World Health Organization (WHO) as an integral aspect of physical, emotional, mental, and social health. Female sexual health, in particular, is influenced by a complex interplay of biological, psychological, sociocultural, and relational factors. Female sexual dysfunction (FSD), encompassing disorders of sexual desire, arousal, orgasm, and pain, is a highly prevalent yet underdiagnosed condition, especially in low- and middle-income countries. Studies from both developed and developing nations estimate the prevalence of FSD to range from 30% to 60% across different populations, with significant implications for quality of life, self-esteem, interpersonal relationships, and psychological health.1,2 Despite its clinical importance, the recognition and evaluation of FSD remain limited, particularly in conservative societies such as India, where open discussion about female sexuality is often discouraged due to prevailing cultural norms and gender roles. A major barrier to the diagnosis and management of FSD is the lack of validated, language-appropriate, and culturally sensitive instruments to assess female sexual function in routine clinical and research settings. The development and validation of such instruments are crucial not only for individual patient care but also for large-scale epidemiological studies and public health interventions targeting sexual health and reproductive rights. The Female Sexual Function Index (FSFI), developed by Rosen et al. in 2000, is one of the most widely used and psychometrically validated tools to evaluate female sexual function across six core domains: Desire, arousal, lubrication, orgasm, satisfaction, and pain. 3 Comprising 19 questions, the FSFI has demonstrated excellent reliability, validity, and responsiveness across multiple settings and populations. It has since been translated and validated into over 30 languages, including Chinese, Arabic, Turkish, Portuguese, and Spanish, thereby enabling cross-cultural comparisons of sexual function and dysfunction among women globally.4,5 In the Indian context, community- and clinic-based studies have reported a prevalence of FSD ranging from 40% to 70%, with desire and arousal disorders being the most commonly affected domains. Factors such as sociocultural taboos, limited sexual health literacy, and restricted access to specialized care further contribute to underreporting and underdiagnosis of FSD among Indian women. 6 However, there is currently no formally validated Hindi version of the FSFI (FSFI-H) available for use in Indian clinical or research contexts. Hindi is spoken by more than 44% of India’s population and is one of the most widely spoken languages globally. Mere translation is insufficient; a validated adaptation must undergo a structured process of forward and backward translation, expert review, cognitive debriefing, and comprehensive psychometric testing to ensure conceptual equivalence and clinical utility across populations.6,7 Previous studies have underscored the importance of contextualizing sexual health instruments within cultural frameworks. For example, concepts such as sexual desire and satisfaction may be perceived differently in South Asian cultures compared to Western contexts due to differing gender norms, marital expectations, and privacy concerns. These cultural distinctions necessitate not just linguistic translation but also semantic, experiential, and conceptual adaptation of each questionnaire item.8,9 Furthermore, psychometric validation involving statistical assessments of reliability (e.g., internal consistency, test-retest reliability) and validity (e.g., construct, discriminant, and known-group validity) is essential before an instrument can be recommended for routine use. The methodology followed internationally accepted standards for cross-cultural validation of patient-reported outcome measures, including guidelines from the WHO, the International Society for Pharmacoeconomics and Outcomes Research (ISPOR), and the Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN). We hypothesized that the FSFI-H would demonstrate acceptable internal consistency, test-retest reliability, factorial structure consistent with the original FSFI, and the ability to discriminate between women with and without clinically diagnosed FSD. By providing a validated FSFI-H tool, this study aims to bridge a critical gap in sexual medicine in India and facilitate the systematic evaluation of female sexual function in both clinical and community settings.
Methods
Study Design and Setting
This was a cross-sectional, instrument validation study conducted between January and April 2025 at the outpatient gynecology department of a tertiary care teaching hospital in Western India. The study protocol was approved by the Institutional Ethics Committee (No. TXUR 2024–28), and written informed consent was obtained from all participants before enrollment.
Participants
A total of 200 sexually active, Hindi-speaking women aged 18–50 years were recruited using consecutive sampling. Inclusion criteria were: (a) Heterosexual women in a stable sexual relationship for ≥6 months, (b) ability to read and comprehend Hindi, and (c) provision of informed consent. Exclusion criteria included: (a) Diagnosed psychiatric illness, (b) active pelvic pathology (e.g., malignancy, pelvic inflammatory disease), (c) current pregnancy or postpartum period <6 months, and (d) use of medications known to affect sexual function (e.g., Selective Serotonin Reuptake Inhibitor [SSRIs], antipsychotics, hormonal therapy).
Instrument: Female Sexual Function Index
The FSFI is a 19-item, self-report questionnaire designed to evaluate female sexual function across six domains: Sexual desire (two items), arousal (four items), lubrication (four items), orgasm (three items), satisfaction (three items), and pain (three items). Each item is scored using a 0 or a 1–5 Likert scale, and domain scores are weighted to yield a composite total score ranging from 2 to 36. A total score below 26.55 indicates possible sexual dysfunction.
The original English FSFI was translated into Hindi in accordance with WHO and ISPOR guidelines for the cross-cultural adaptation of patient-reported outcome measures.2,3 The process involved:
Forward translation Reconciliation Backward translation Expert panel review Cognitive debriefing
Data Collection
Eligible participants were invited to complete the final FSFI-H in a private outpatient setting. For test-retest reliability assessment, a subset of randomly selected participants (n = 40) completed the FSFI-H again after a two-week interval under similar conditions. Participants were categorized into two groups based on clinical evaluation: (a) Women with diagnosed sexual dysfunction (based on Diagnostic and Statistical Manual of Mental Disorders, 5th Edition [DSM-5] criteria), and (b) women without any self-reported or clinically evident dysfunction, to evaluate known-group validity.
Data were analyzed using IBM Statistical Package for the Social Sciences (IBM SPSS) Statistics version 20.0. Statistical significance was set at P < .05.
Internal consistency: Assessed using Cronbach’s alpha for the total FSFI-H and each domain. Values ≥0.70 were considered acceptable.
Test-retest reliability: Evaluated using the intraclass correlation coefficient (ICC) (two-way mixed-effects model). ICC values ≥0.75 indicated good reliability.
Construct validity: Assessed using exploratory factor analysis (EFA) with principal component extraction and varimax rotation. Sampling adequacy was determined by the Kaiser-Meyer-Olkin (KMO) statistic and Bartlett’s Test of Sphericity.
Known-groups validity: Total and domain-wise FSFI-H scores were compared between women with and without sexual dysfunction using independent samples t tests, with Cohen’s d used to estimate effect size.
Results
Participant Characteristics
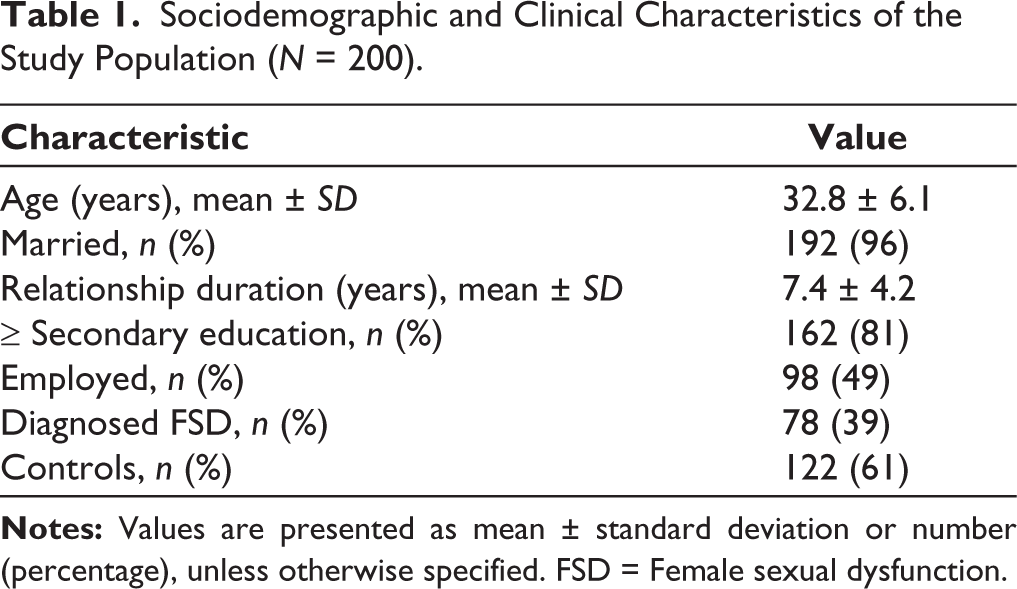
A total of 200 sexually active, Hindi-speaking women completed the study. The mean age was 32.8 ± 6.1 years (range: 21–50 years). The mean duration of the relationship was 7.4 ± 4.2 years. Based on clinical evaluation and DSM-5 criteria, 78 women (39%) were categorized as having FSD, while 122 (61%) served as controls, as shown in Table 1.
Sociodemographic and Clinical Characteristics of the Study Population (N = 200).
Internal Consistency
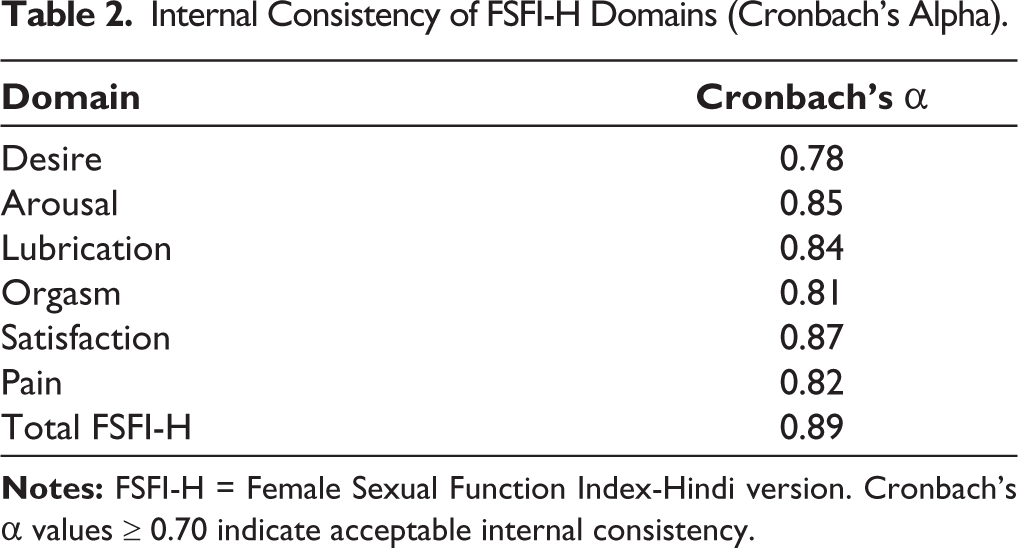
The FSFI-H demonstrated excellent internal consistency, which is shown in Table 2. The overall Cronbach’s alpha for the 19-item FSFI-H was 0.89, indicating strong reliability. Domain-specific alpha values were also acceptable to excellent:
Internal Consistency of FSFI-H Domains (Cronbach’s Alpha).
Test-retest Reliability
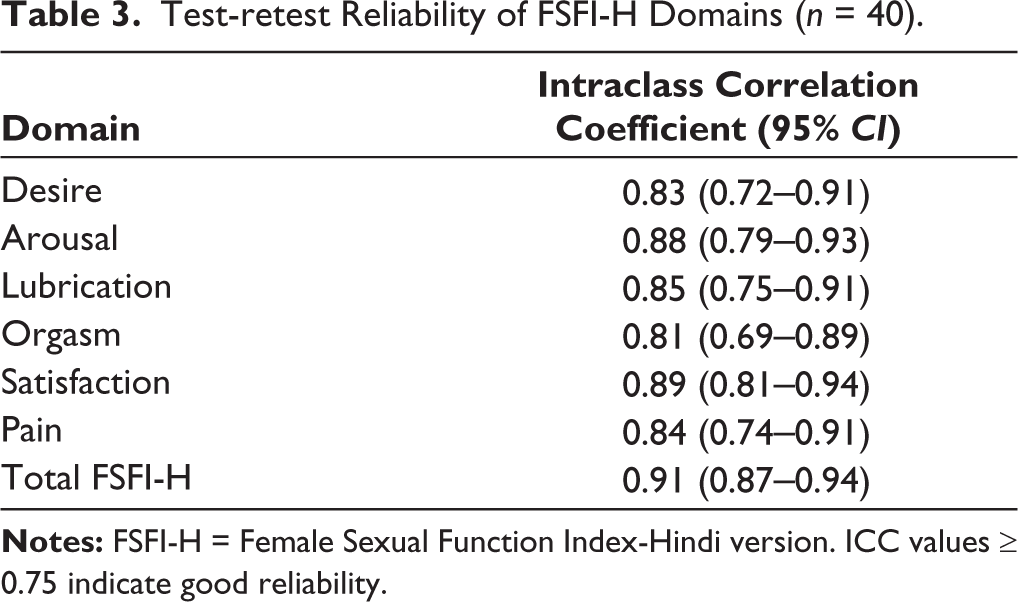
A subgroup of 40 participants completed the FSFI-H again after a two-week interval. The ICC for the total score was 0.91 (95% CI: 0.87–0.94), indicating excellent temporal stability. ICCs for individual domains ranged from 0.81 to 0.93, reflecting robust reproducibility of the FSFI-H across time, as shown in Table 3.
Test-retest Reliability of FSFI-H Domains (n = 40).
Construct Validity
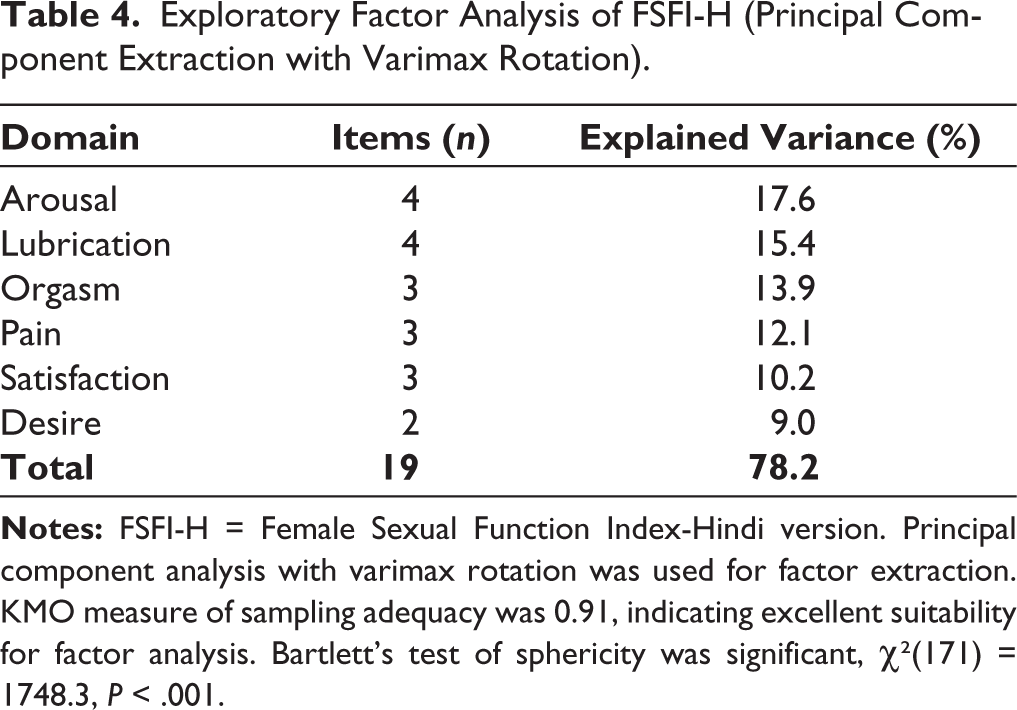
EFA was performed to examine the underlying structure of the FSFI-H. The KMO measure of sampling adequacy was 0.91, and Bartlett’s test of sphericity was statistically significant (χ² = 1,748.3, df = 171, P < .001), indicating suitability for factor analysis. Principal component analysis with varimax rotation extracted six factors with eigenvalues >1, accounting for 78.2% of the total variance. Each factor corresponded to one of the six original FSFI domains, supporting the theoretical construct of the instrument as shown in Table 4.
Exploratory Factor Analysis of FSFI-H (Principal Component Extraction with Varimax Rotation).
All domain values exceeded the minimum threshold of 0.70, supporting high internal reliability of the instrument.
Known-groups Validity
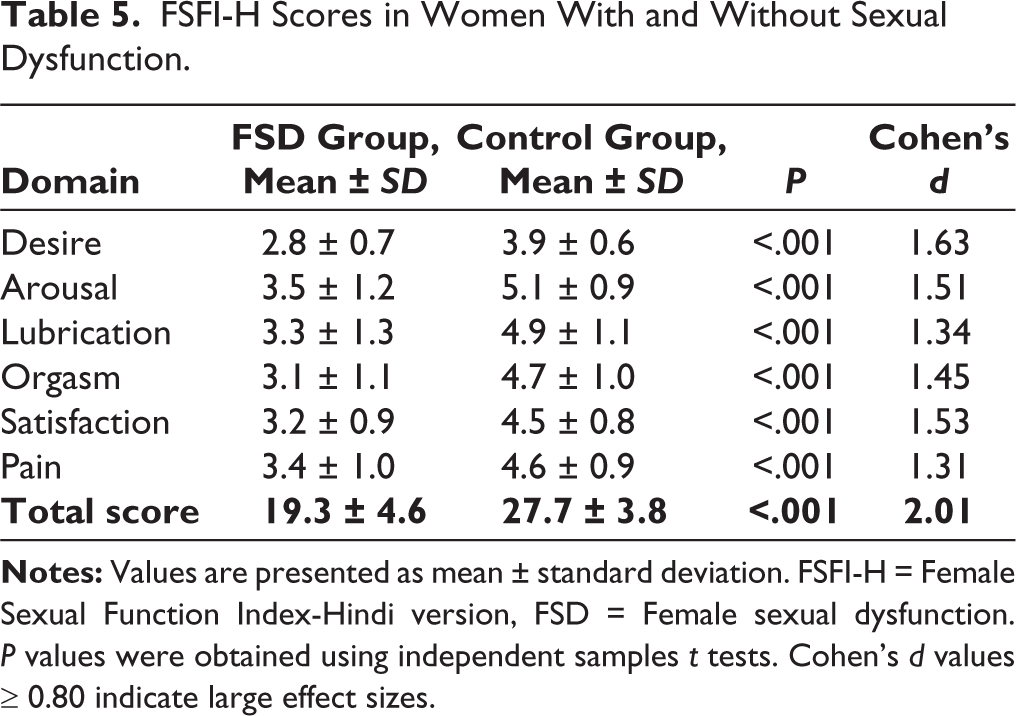
Women with clinically diagnosed sexual dysfunction had significantly lower total FSFI-H scores compared to controls (mean ± SD: 19.3 ± 4.6 vs. 27.7 ± 3.8, P < .001). Domain-wise scores also showed statistically significant differences between groups: The effect size for the total FSFI-H score difference was large (Cohen’s d = 2.01), confirming the instrument’s ability to discriminate between known-groups as shown in Table 5.
FSFI-H Scores in Women With and Without Sexual Dysfunction.
Discussion
This study aimed to translate, culturally adapt, and psychometrically validate the FSFI-H for use among sexually active women in India. Our findings demonstrate that the FSFI-H is a linguistically appropriate, culturally sensitive, and psychometrically robust instrument that can be confidently used in both clinical practice and research to assess female sexual function in Hindi-speaking populations. The FSFI-H exhibited excellent internal consistency, with a Cronbach’s alpha of 0.89 for the overall instrument and acceptable to excellent alpha values (ranging from 0.78 to 0.87) across the six individual domains. These values are consistent with previous validations of FSFI across different cultures and languages. For example, a study by Aygin et al. reported α = 0.89 for the Turkish FSFI, while Sun et al. found α = 0.87 for the Chinese version.4,6 This consistency underscores the cross-cultural robustness of the FSFI’s theoretical structure, even when adapted to diverse linguistic and social environments such as India. Our study also confirmed the temporal stability of the FSFI-H. The test-retest reliability, assessed using ICCs over a two-week interval, yielded a strong ICC of 0.91 for the total score, with domain-specific ICCs all exceeding 0.80. These results reinforce the stability of the FSFI-H when administered over time, a critical feature for use in both longitudinal studies and repeated clinical assessments. The construct validity of the FSFI-H was supported through EFA, which yielded a six-factor structure aligning closely with the theoretical domains of the original FSFI. These factors explained over 78% of the total variance, suggesting a strong underlying structure. The adequacy of our sample size and the high KMO value (0.91) further supported the factorability of the correlation matrix. Previous validation studies have reported comparable explained variance in the range of 70%–80%,3,4 reinforcing the psychometric soundness of the FSFI-H. One of the most compelling findings was the demonstration of known-groups validity. Women with clinically diagnosed sexual dysfunction scored significantly lower on the FSFI-H total and domain scores than those without dysfunction. The mean total score for the dysfunction group was 19.3 ± 4.6 compared to 27.7 ± 3.8 in the control group (P < .001), with a large effect size (Cohen’s d = 2.01). These results are consistent with prior research validating the FSFI in different populations and support the scale’s ability to discriminate meaningfully between individuals with and without clinically significant dysfunction.5,6 This study addresses a critical gap in sexual health research in India, where tools to assess FSD in native languages are lacking. Although sexual dysfunction affects a substantial proportion of Indian women, estimates range from 30% to 70% depending on the region and methodology, systematic evaluation has been limited by the unavailability of culturally validated assessment tools.7,8 Given that Hindi is the most widely spoken language in India, used as a first language by over 500 million people, the availability of FSFI-H could significantly enhance the capacity for sexual health screening, diagnosis, and research across the country. The cultural adaptation process was pivotal. The translation followed WHO and ISPOR guidelines and involved a multidisciplinary expert panel and cognitive debriefing with pilot participants. This ensured not only semantic equivalence but also conceptual and experiential alignment with the cultural realities of Indian women. Importantly, feedback from the pilot participants confirmed that the final Hindi version was clear, non-threatening, and acceptable for use in a clinical setting. The availability of a validated, self-administered Hindi tool such as FSFI-H can empower both patients and healthcare providers. 10 For women, it offers a confidential way to express concerns that they may be reluctant to articulate in face-to-face consultations. For clinicians, it enables objective screening and documentation, helping to guide further evaluation or referral when needed.
Strengths of this study include:
This is the first validated FSFI-H, addressing a major unmet need in sexual health assessment tools for the Hindi-speaking population in India. The study followed internationally accepted guidelines for translation and cultural adaptation of patient-reported outcome measures (WHO, ISPOR, COSMIN), enhancing its methodological rigor and reproducibility. A comprehensive psychometric evaluation was undertaken, including internal consistency, test-retest reliability, EFA, and known-groups validity with effect size estimation. The study sample was large (n = 200), well-characterized, and adequate for statistical techniques such as factor analysis. The tool demonstrated robust discrimination between women with and without sexual dysfunction, supporting its clinical applicability.
Limitations of the study:
The study was conducted at a single urban tertiary care center, which may introduce selection bias and limit generalizability to rural, tribal, or lower-literacy populations. All participants were heterosexual, married women aged 18–50 years. The findings may not apply to unmarried women, postmenopausal women, adolescents, or members of the Lesbian, Gay, Bisexual, Transgender, Queer (or Questioning), + encompasses additional identities such as Intersex, Asexual, Pansexual, Non-binary, and others (LGBTQ+) community, who are also in need of validated assessment tools. The cross-sectional design precludes conclusions about responsiveness to change or the scale’s sensitivity to treatment effects. Future longitudinal studies are needed to assess this. Despite efforts to ensure privacy, social desirability bias remains a concern, particularly in conservative cultures where discussing sexuality is often taboo. Participants may have underreported symptoms due to embarrassment or fear of judgment.
Conclusion
The FSFI-H demonstrated strong psychometric properties, including high internal consistency, excellent test-retest reliability, and clear construct, and known-groups validity. As the first validated tool of its kind in Hindi, the FSFI-H fills a critical gap in the clinical assessment of female sexual function in India. It provides healthcare professionals and researchers with a reliable and culturally appropriate instrument to screen for, diagnose, and monitor FSD. Given the linguistic diversity and persistent stigma surrounding women’s sexual health in India, the FSFI-H has the potential to improve access to care, enhance communication, and generate high-quality data for research and public health initiatives.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.