
Abstract
Introduction:
Depression is a widespread issue among women in India, affecting all age groups. It can lead to sexual dysfunction, which is more commonly found in females than males, but often goes unreported. The purpose of the study was to evaluate the sexual functioning of females with depression.
Methods:
The study utilized a cross-sectional research approach to assess 60 females who were diagnosed with depression according to International Statistical Classification of Diseases, Tenth revision (ICD-10) in a psychiatric outpatient department (OPD). The assessment included the use of Mini International Neuropsychiatry Interview (MINI) 6.0.0 screener, sociodemographic and clinical variables, Hamilton Depression Rating Scale (HAM-D) scale, and Female Sexual Functioning Index (FSFI). The study sample only included married females who were drug-naive for the last three months, stayed with their husband for the majority of the time, and were willing to participate in the study.
Results:
The FSFI test revealed that 61.67% of the participants experienced sexual dysfunction across all domains, with the greatest impact observed in the desire, arousal, and orgasm domains. Lower mean percentages were indicative of more severe sexual dysfunction. Correlation analysis revealed a weak negative relationship between age, the severity of depression, and the duration of the current episode with sexual functioning; however, the results were not statistically significant.
Conclusion:
According to this study, depressed females experience sexual dysfunctions. Therefore, healthcare providers should ask and consider the sexual aspect while treating patients with depression. Identifying, discussing, and managing problems related to sexual health at an early stage are crucial.
Introduction
Everyone can experience depression. Depression is more likely to strike those who have experienced abuse, significant losses, or other stressful situations. Compared to men, women experience depression at a higher rate.
An estimated 3.8% of people suffer from depression, including 5.7% of individuals over 60 and 5% of adults (4% of males and 6% of women). Depression affects over 280 million people worldwide. 1 Women are around 50% more likely than men to experience depression. Moreover 10% of expectant mothers and recent mothers experience depression globally. 2
An estimated 57 million people (18% of the total global population) suffer from depression in India. In the upcoming years, depression is probably going to rise in India due to the country’s major developments (globalization, urbanization, migration, and modernization) combined with a fast changing sociodemographic landscape. According to the National Mental Health Survey (NMHS) (2015-16) in India, one in twenty (5.25%) adults over the age of eighteen had experienced depression at least once in their lives, making approximately 45 million people with depression in 2015. 3
Lowered self-esteem, decreased energy, disinterest, and an inability to enjoy life—that is, social disengagement and irritability—are all signs of depression. It can also make it difficult to maintain close relationships. Depression has long been linked to sexual problems, and these symptoms are thought to cause issues in sexual interactions. 4 A person’s sexuality is an aspect of their investigation, interest, and curiosity. The physiological ability to go through different phases of the sexual process, such as arousal, desire, and orgasm, is known as sexual function. This process includes intricate interactions between the neurological, vascular, and endocrine systems as well as psychological elements that are crucial for arousal, sex, and satisfaction. Inherited cultural norms, specific medical conditions, psychological conflicts, interpersonal issues, and cultural influences can all contribute to sexual dysfunction. 5
While depression can strike anyone at any age, the National Institute of Mental Health (NIMH) notes that it is more common in women. Hormonal shifts have been linked to a higher risk of depression in women, according to the NIMH. Because of this, a woman’s risk of depression may rise before to, during, and following her menstrual cycle, as well as throughout the perimenopause and menopause. The majority of women are prone to having enduring “bluesy” sensations, which can lower their self-esteem and sense of worth. Overall sex life might be significantly altered by these feelings. Natural lubrication can also be interfered with by low estrogen levels. If women do not seek assistance to obtain relief, these issues may be distressing to them. 6
The most significant component of being human is one’s sexuality, which encompasses sex, gender identities and roles, sexual orientation, pleasure, eroticism, intimacy, and ultimately reproduction. Attitudes, wants, ideas, fantasies, beliefs, values, different roles and relationships, behaviors, and practices are all examples of how sexuality is experienced and expressed. Women are often sexually active during their youth, but they don’t reach their peak orgasmic frequency until they are 30 years old. After that, they maintain a steady level of sexual capability until they are 55 years old, and there is not much evidence to suggest that aging has an impact on later life. Numerous illnesses affecting the sexual response cycle are common in females. In general, the prevalence ranges from 35% to 40%. 7
According to International Statistical Classification of Diseases, Tenth revision (ICD-10), sexual dysfunction is a change in sexual function that is considered unsatisfying, inadequate, or unrewarding. It can also be defined as a harmful change in sex response. 8 Studies indicate that sexual dysfunction is a prevalent issue, with 43% of women and 31% of men reporting some level of trouble. However, many people are ashamed to discuss their sexual problems and are reluctant to do so. 9
Psychotropic medications are known to cause sexual dysfunction. But it can be challenging to distinguish between side effects of medication and the impacts of psychiatric disorders, especially when mental illnesses have a significant impact on interpersonal connections. Although sexual dysfunction brought on by antidepressants may be significant to patients and a factor in treatment non-compliance, there is a dearth of scientific data on this topic. 10
Several Indian studies attempted to evaluate sexual dysfunction among women suffering from a depressive episode.11-13 Studies measured sexual function in heterogeneous groups of patients (who are already on different antidepressant medications, who is on a specific antidepressant, all patients irrespective of their antidepressant treatment status, and drug-free patients of depression). It was found that the sexual dysfunction is profound in patients with depression. It can be difficult to distinguish between sexual dysfunction and sadness when it comes to sexual dysfunction. Thus, in order to evaluate sexual dysfunction in females with depression who had not used antidepressants for the previous three months, the patient who was not getting antidepressant medication was included in this study.
Methodology
A cross-sectional study at a tertiary care unit in North India was conducted. Samples were taken only from outpatient department (OPD) since the inpatient patient gets started with antidepressants which could have brought bias in the study. The sample was females coming for treatment at the OPD of psychiatry, King George’s Medical University Lucknow, who are diagnosed with depression, drug-naive for the last three months, willing to participate in the study. The sampling technique used was the purposive sampling technique. A total of 86 samples were screened during the period of data collection and 60 samples were included in the study; they should be married female who are diagnosed with depression and drug-naive, staying with a spouse for the majority of days. Written and informed consents had been obtained; patients with severe depression with psychotic symptoms were excluded from the study.
Questionnaire
The survey was carried out in the clinical area; demographic and clinical data were collected from the patients. The questionnaire was in six parts: Mini International Neuropsychiatry Interview (MINI) 6.0 for co-morbidities, sociodemographic and clinical data, Hamilton Depression Rating Scale (HAM-D) for depression, and female sexual functioning index (FSFI) for the assessment of female sexual function.
Female Sexual Functioning Index
Female sexual functioning is a multidimensional self-report instrument for the assessment of female sexual function. It was prepared by R. Rosen, C. Brown, and J. Heiman et al. 15 It includes six-domain desire, subjective arousal, lubrication, orgasm, satisfaction, and pain. It includes a total of nineteen items in it. FSFI score ranges from 2 to 36. Scores less than 26.55 are taken as an indicator of sexual dysfunction.
Ethical Consideration
Administrative permission from the University Ethics Committee of King George’s Medical University was obtained. Ref. code: 82nd ECM IID-a/P3 No.144/ethics/R.Cell-17. Informed consent was obtained from the entire participant.
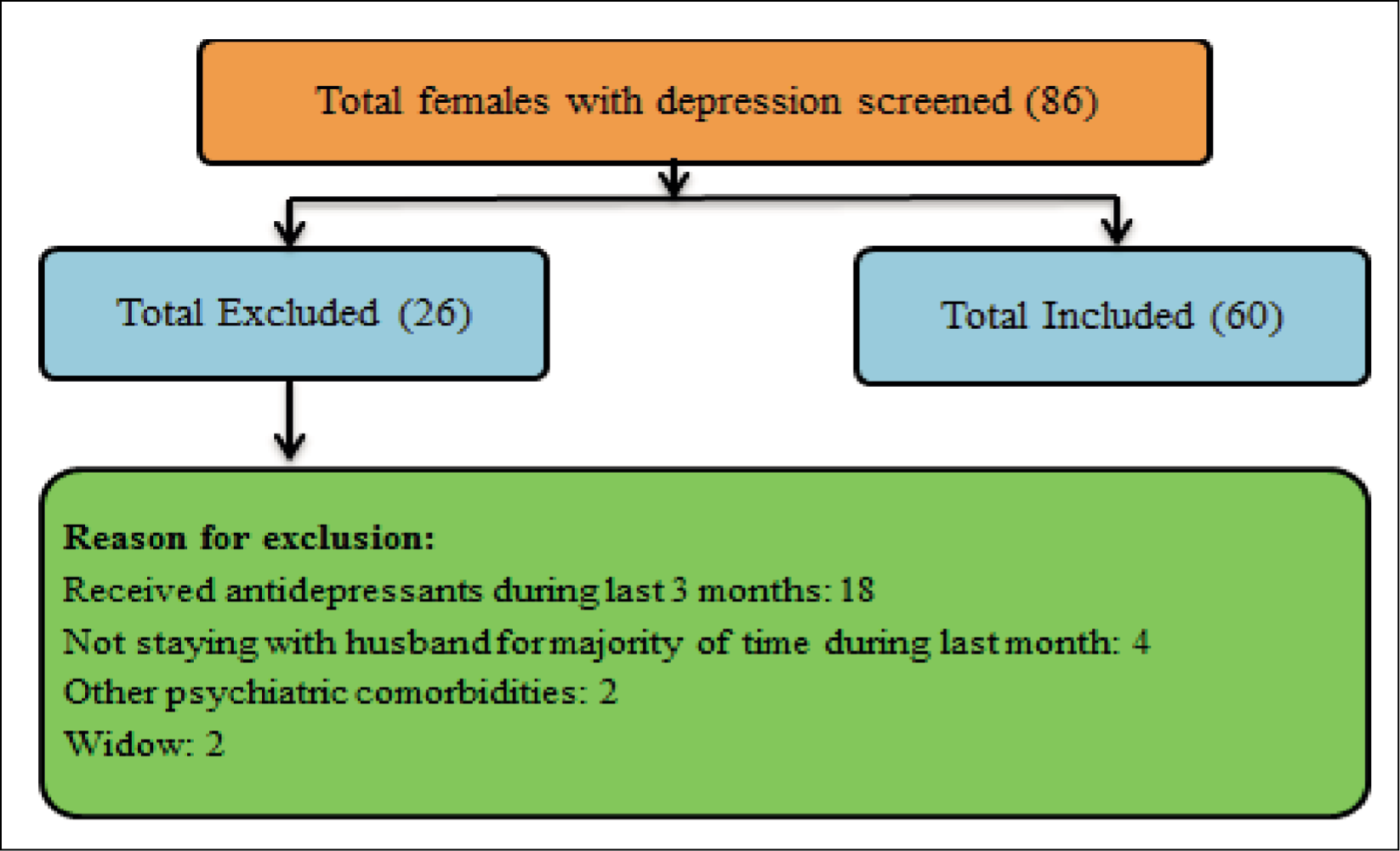
Diagrammatic Presentation of Selection of the Sample
The Selection of Sample and Reason for Exclusion.
Result
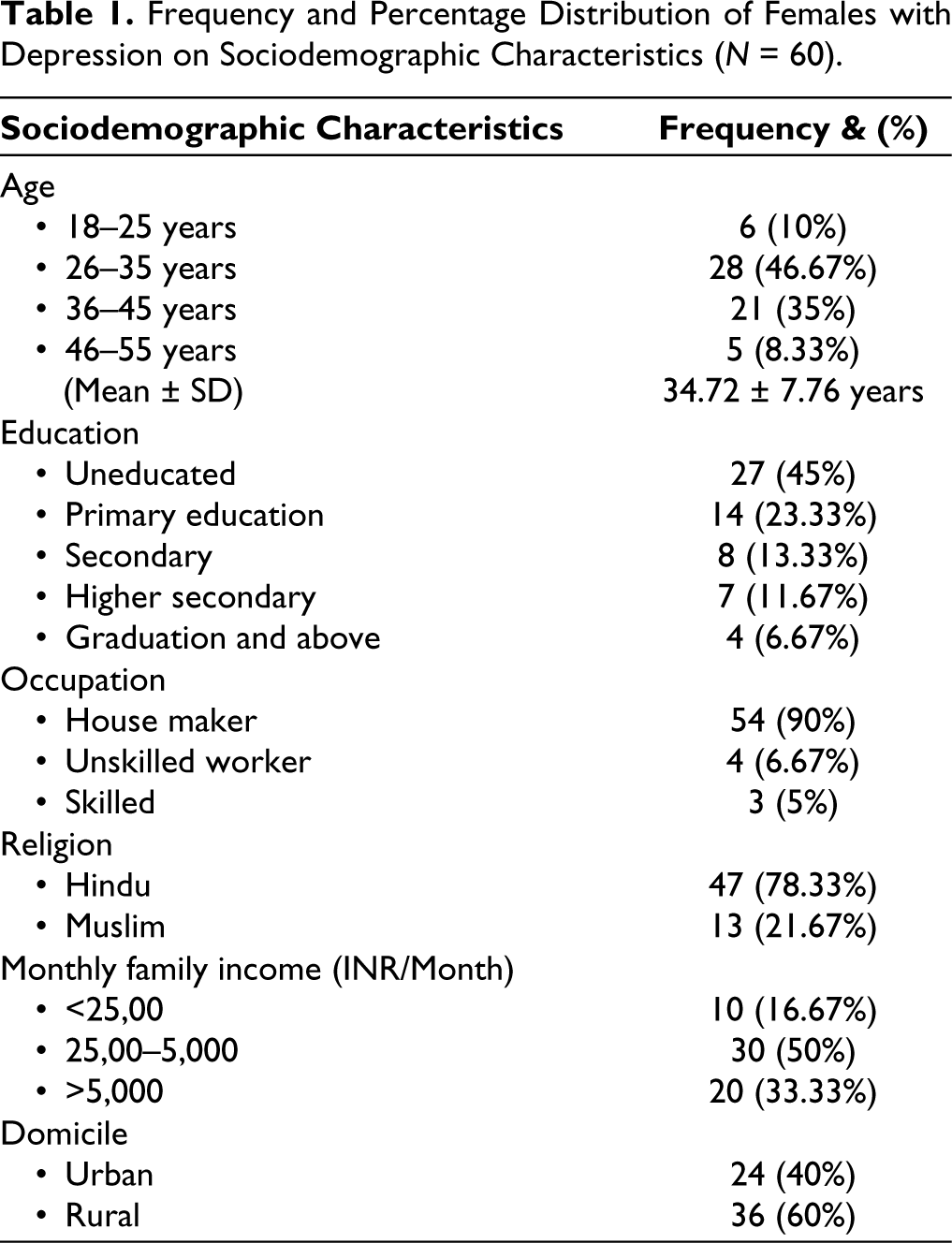
The findings of the study revealed total 86 subjects were screened, out of which 26 were excluded and 60 were included (Figure 1). The mean age of the subjects was 34.72 ± 7.76 years. The age range was 18-55 years and most subjects (27; 46.67%) were aged between 26 and 35 years and 27 (46.15%) subjects were uneducated. Fifty-four (90%) subjects were house makers. Forty-seven (78.33%) subjects were Hindus. Thirty (50%) subjects had monthly family income between 25,00 and 5,000. The majority of the sample (60%) belongs to the rural area (Table 1).
Frequency and Percentage Distribution of Females with Depression on Sociodemographic Characteristics (N = 60).
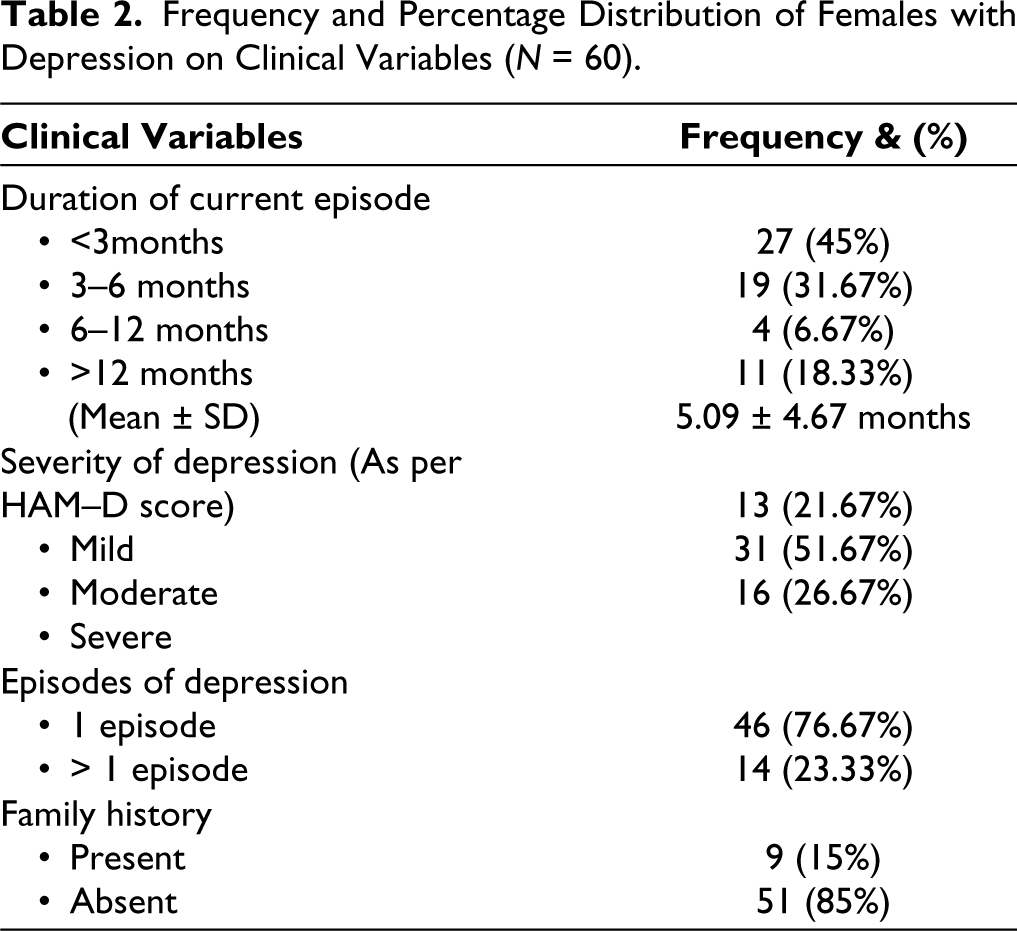
The mean duration of depression was 5.09 ± 4.67 months. Twenty-seven (45%) subjects had less than three months of duration of illness and four subjects (6.67%) had between 6 and 12 months of duration. Almost half of the patients (31, 51.67%) had moderate depression. Forty-six (76.92%) subjects had the first episode of depression. Fifty-one (85%) subjects had no family history of mental illness (Table 2).
Frequency and Percentage Distribution of Females with Depression on Clinical Variables (N = 60).
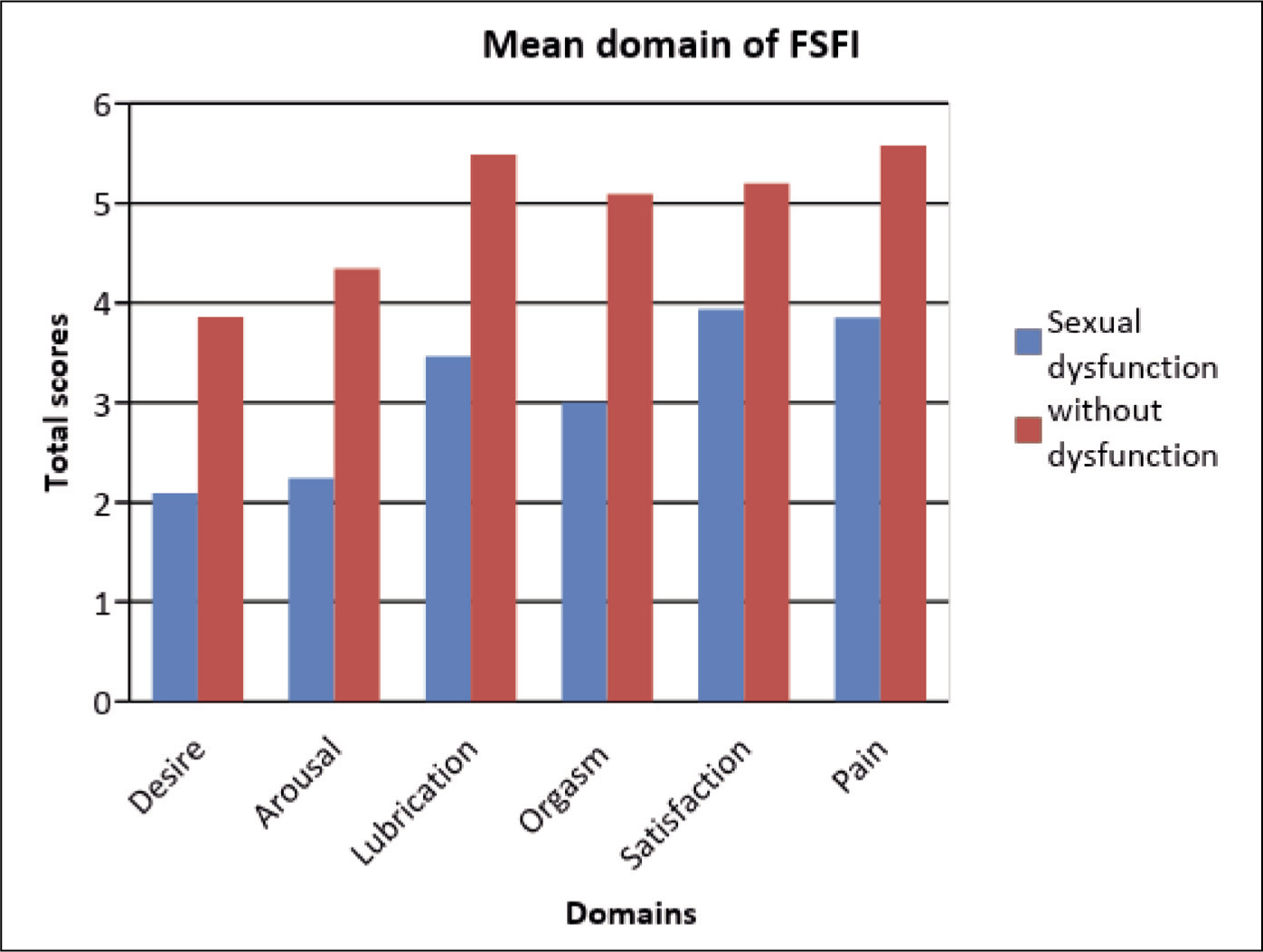
To assess sexual functioning, FSFI tool was applied; out of total 60 subjects, 37 (61.67%) of the females had sexual dysfunction, which says that there is the presence of sexual dysfunction among drug-naive patients with depression, which means that in more than half of the patients depression might have attributed to sexual dysfunction. Total mean score of FSFI was 25.64 ± 4.90. Most of the domains were affected in sexual dysfunction in which desire domain was highly affected; mean score was 2.09 ± 0.87, arousal domain mean was 2.24 ± 1.33, orgasm domain means was 3.01 ± 2.04, lubrication domain was 3.46 ± 2.17, satisfaction domain was 3.85 ± 2.33, the least affected domain was pain, and mean score was 3.85 ± 2.33.
Out of a total of 60 subjects, 37 (61.67%) of them had sexual dysfunction. The mean score of FSFI among the sexual dysfunction group was 18.57 (standard deviation (SD) = 8.44) and 29.57 (SD = 2.39) in the without sexual dysfunction group. There was a significant difference between both groups (P = < .0001; Table 3 and Figure 2).
Frequency and Percentage Distribution of Sexual Functioning Among Females with Depression as Assessed on Female Sexual Functioning Index (FSFI) (N = 60).
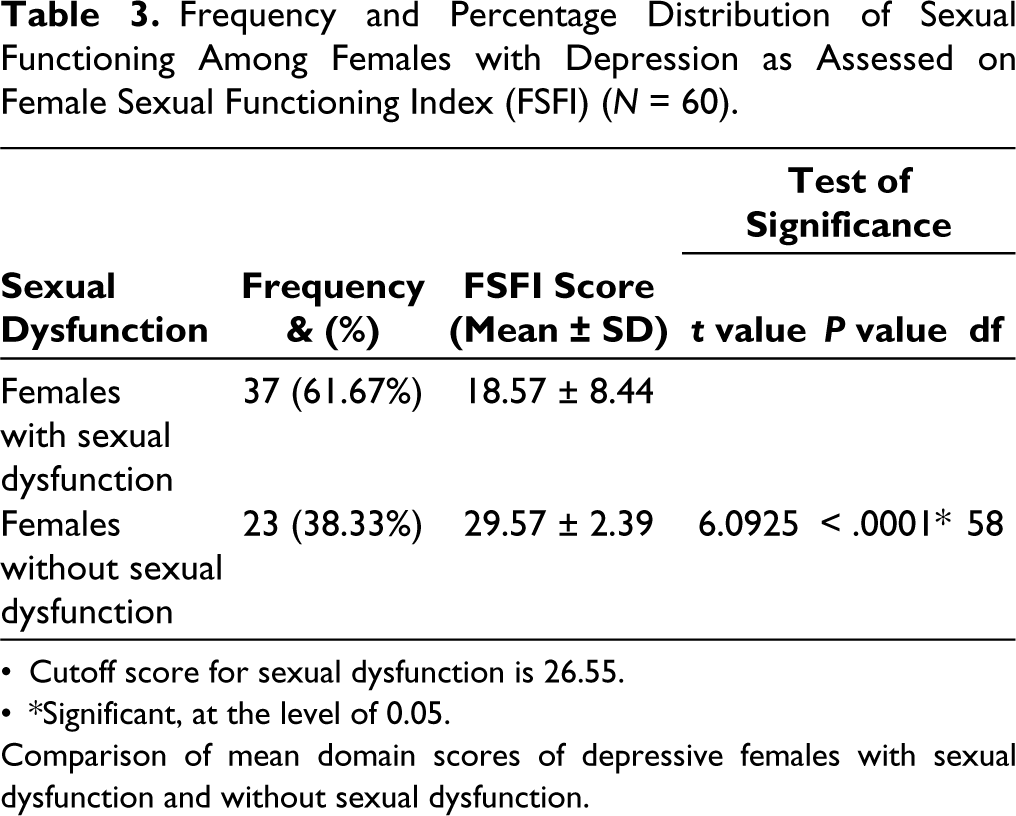
Cutoff score for sexual dysfunction is 26.55. *Significant, at the level of 0.05.
Comparison of mean domain scores of depressive females with sexual dysfunction and without sexual dysfunction.
Bar Diagram Showing Mean Domain Score of Depressive Females with Sexual Dysfunction and Without Sexual Dysfunction.
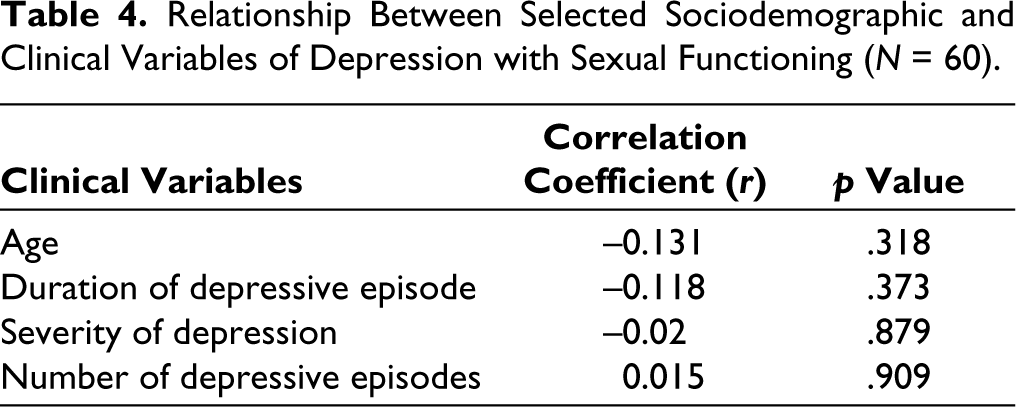
There is negative correlation with age and the sexual functioning (r = −0.131) (p = .318). Between the duration of depression and the sexual functioning the r value is −0.118, P value is .373 which shows that there is negative correlation with duration of depression and the sexual functioning. Between the severity of depression and sexual functioning, the r value is −0.02 P value is .879 which shows that there is negative correlation with severity of depression and sexual functioning. Between the number of depressive episode and the sexual functioning, the r value is 0.015 and P value is .909 which shows that there is no significant correlation with number of depressive episodes and the sexual functioning (Table 4).
Relationship Between Selected Sociodemographic and Clinical Variables of Depression with Sexual Functioning (N = 60).
Discussion
In developing countries like India, where there are significant cultural challenges and a stigma against openly discussing sexual health, female sexual dysfunction is one of the conditions that is underdiagnosed worldwide. It is frequently underreported or undiagnosed globally in comparison to male sexual dysfunction. 11 According to research conducted in India, the percentage of nondepressed women with female sexual dysfunction ranges from 33.3% to 73.2%.12,13 It was reported that the widely disparate research samples, methodological variances, and cultural disparities in sexual conduct in India were the causes of the variable rates. 13 Studies on female sexual dysfunction in depressed women are even very few.
The study population in our research mostly have mild-to-moderate depressive episodes, which is in accordance with the predominant population of a similar study that evaluated sexual functioning in women with depression, but this study also included psychotic depression. Another similar study has a predominant population with mild-to-moderate depression. 16 The study by Roy et al. 17 included patients with depression who are in remission and on stable dose of escitalopram. Most of the sociodemographic characteristics of our study population also resemble the population characteristics of the above three studies. A variation in prevalence of sexual dysfunction was reported in these studies and our study, which can be largely explained due to difference in the clinical characteristics of the study population (i.e., severity of depressive episode, remission, antidepressant, other psychotropic medications, psychotic depression). Antidepressants and other psychotropic medications affect the sexual functioning of women adversely. 18 However, the study population in our study are not on any medications. It indicates the sexual dysfunction in our study population is largely attributable to the depressive episode. All domains of sexual functioning are affected in our patients, indicating that depression affects all the domains of sexual functioning in women.
In our study, the correlation between age, duration of depressive episode, severity of depression, and number of depressive episodes with sexual functioning is insignificant. This is quite possible due to narrow age range (majority of the patients are between 26 and 45 years of age), narrow duration of depressive episode (>75% had duration of episode less than 6 months), >75% patients had single episode of depression, and mostly having moderate depression. As the data dispersion is less in a smaller sample population, finding a significant correlation becomes difficult. Perhaps a larger population with dispersed data may give significant correlation. Stringent selection criteria sometimes give such type of findings due to inclusion of more homogeneous population.
In this study, 37 (61.67%) of the sixty female individuals in this study experienced sexual dysfunction; this suggests that in over 50% of the patients, sexual dysfunction may have been a contributing factor to their depression. Sexual dysfunction impacted in majority of domains, desire domain being mostly affected. Our finding was consistent with the study done by Reddy et al. 16 They found that all components of sexual functioning were affected, and the majority reported lubrication dysfunction, pain, and orgasmic dysfunction. Low desire, low arousal, and low satisfaction were also reported.
In this study, we found there is negative correlation between age, duration of depression and severity of depression with the sexual functioning. A study done by Fabre and Smith19 found that with increasing severity of depression (increased HAM-D scores), sexual dysfunction becomes greater (lower DISF scores).
Limitation
Small sample size is a limitation of this study. Due to stringent selection criteria, generalizability is limited to specific group of clinical population (drug-naive patients with depression in clinical settings).
Conclusion
In this study, there was a severe sexual dysfunction of sexual activity in depression in all domains of female sexual cycle which was the drive, arousal, lubrication, orgasm, satisfaction, and pain. Moderate depression was highest among the group. There was negative correlation with the age, duration of depressive episode, severity of episode, and no significant correlation between numbers of episode with the FSFI score. Poor sexual functioning can be distressing for the patients. Hence, we being a psychiatric nurse and the first listener of the patients should dutifully and empathetically assess the female sexual needs and functions ensuring privacy and confidentiality using rating scales; therefore, we can report the patient problem to the clinicians which can aid in treatment and drug selection. If asked, we can assess and addressed regularly, so that women will feel less hesitant and report more freely their problems.
Implications
Individuals need to have adequate knowledge regarding sexuality and its importance to develop a positive attitude towards sexuality. During sex, an individual undergoes various physiological and psychological changes; hence, it is important to identify the normal sexual cycle and its response in the body. People usually do not know the normal cycle of sex, so they do not recognize that they are having problems, and they never report their problems. Therefore, while being with the patient in their treatment, the patient needs to ventilate about their sexual problem and identify the problems, so that it can aid in the treatment of the patient and the early recovery of depression. There is a need to psycho-educate about treatment compliance and early identification of any adverse effects, especially those related to sexual behavior. Some studies show that poor sexual function leads to depression; thus, it needs to ventilate the patient’s emotions and identify the main reason for developing depression.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical Approval was taken from Institutional Ethical Committee at King George’s Medical University. No. 144/Ethics/R. cell-17 Ref. code:82nd ECM IID-a /P3.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from the entire participant.