
Abstract
Introduction:
Depression-associated sexual dysfunction (SD) is a pervasive and ignorant problem among the general population. The antidepressant used to treat depression may further alter the sexual response cycle in one way or another. This study aims to assess the prevalence of SD in females with major depressive disorders and the effects of antidepressant therapy after 4 weeks of follow-ups.
Material and Methods:
In a prospective observational survey, 94 women diagnosed with depression and on antidepressant therapy were purposively enrolled. Female Sexual Functioning Index (FSFI) and Montgomery-Asberg Depression Rating Scale (MADRS) are administered at baseline and 4 weeks of treatment to measure sexual function and depression changes. Relevant descriptive and inferential statistics are applied to compute the results.
Results:
The mean age of the participants was 35.87 (±5.10) years. A total of 95.7% of participants showed SD at baseline assessment. There was a significant difference (31.87 vs 18.51, P < .001) in depression from baselines to 4 weeks after antidepressant therapy. Further, a significant negative correlation was reported between the MADRS scores and the scores of arousals (r = −0.396, P < .001), lubrication (r = −0.453, P < .001), orgasm (r = −0.342, P < .001), satisfaction (r = −0.407, P < .001), pain (r = −0.362, P < .001), and total domains of FSFI (r = −0.412, P < .001) after 4 weeks. Using cut-off scores of different areas, decreased sexual desire was reported in 97.9%, poor vaginal lubrication (100%), a problem with arousal (100%), reduced satisfaction (96.8%), reduced ability to achieve orgasm (100%), and pain during sexual intercourse in 100% of the participants.
Conclusions:
There is a high prevalence of SD in women with depression. There is a marked improvement in depression at the end of 4 weeks. However, sexual function status remains unchanged and indicates the need for time to improve, suggesting different study designs.
Introduction
Sexual dysfunction (SD) is pervasive and distressing alterations in the normal sexual response cycle. 1 Sex is more than a physical act consisting of 4 phases, desire, arousal, orgasm, and resolution, mediated by neurotransmitters, hormones, and enzymes. 2 Prevalence of depression associated with SD varies between 50 and 70%.3,4 In some cases, SD was associated with predisposing depression and vice versa. 5 Poor motivation, lack of pleasurable social activities, and increased risk of smoking and substance abuse are common risk factors for alteration in SD. 3
However, many patients experience an alteration in SD, 20% to 45%, after antidepressants use. 6 Further, this prevalence varies with antidepressants, 30% with imipramine, 25% to 73% with selective serotonin reuptake inhibitors, and 93% of women and men on clomipramine show partial or total anorgasmia.7,8 However, this incidence of SD is lower with a newer generation of 5-HT2 blockers.9,10
Different antidepressants are known for one or another alteration in the sexual response cycle. Further, it has been observed that antidepressant-induced SD can alter one or more phases of the normal sexual response cycle, including alteration in libido, vaginal lubrication, anorgasmia, and delayed orgasm. 11 In population subgroups, women are relatively at higher risk for anxiety and depressive episodes and have a higher risk of SD. 12 In contrast, their findings are inconsistent with another work that reported a higher prevalence of SD in men than women (62% and 60%). 8
Of note, the use of antidepressant drugs is not limited to mood disorders; they are equally helpful in treating many physical and psychological problems including migraine, smoking, anxiety, alcohol, excessive weight, and controlling postmenopausal symptoms. 3 These contentious findings need more controlled studies.
The management of SD in women with depression is a challenging work. In developing countries like India, publicly talking about sexual functions is freely considered taboo and, therefore, a barrier to delivering adequate and effective treatment for SD. 13 Therefore, it is imperative to ask female patients about their sexual functioning before and after the initiation of antidepressant drug treatment. The authors feel a crunch of regional data on the impact of antidepressant uses on SD in women undergoing treatment for depression. We believe that the depreciation of antidepressant-induced SD could play an essential role in recovery and health-related quality of life. Therefore, we have decided to see the impact of antidepressants on SD and depression, and vice-versa.
Material and Methods
A prospective hospital-based study enrolled 94 women with depression undergoing treatment with antidepressants. Women aged 18 to 45 years staying with husbands diagnosed with depression as per ICD-10 criteria and on antidepressants were enrolled in the study. Women were asked for a stable, monogamous sexual relationship for at least 6 months before being included. Women who can speak Hindi/English language and are willing to participate in the study were included. Women with a significant history of physical and psychological problems, pelvic and retroperitoneal issues/surgery, alcohol and other psychoactive substance abuse, and other medication than antidepressants were excluded from the study. The baseline and 4-week follow-up assessments measured depression and sexual function.
Socio-Demographic Profile Sheet
A semi-structured validated and pretested proforma was used to enquire about sociodemographic details like age, education status, marital status, age of menarche, place of residence, socioeconomic status, age at first pregnancy, number of children, and age of the oldest child. The sociodemographic sheet sought validation from psychology psychiatric nursing, and public health experts.
Female Sexual Functioning Index (FSFI)
It is a brief self-reported scale created for evaluating the core elements of sexual function in females. It consists of 19 questions to evaluate 6 areas of sexual function, including desire, arousal, lubrication, orgasm, satisfaction, and pain. The scale gives a total score of 26.55, an ideal cut-off score for distinguishing females with or without sexual problems. The scale has been used in many earlier similar Indian studies, indicating transcultural validity for its use.14,15 The scale has acceptable reliability coefficient (from 0.89 [satisfaction] to 0.96 [lubrication]). The test-retest reliability coefficient ranged from 0.75 (pain) to 0.86 (desire). 16
Montgomery-Asberg Depression Rating Scale
A 10-item scale developed by Stuart Montgomery and Marie Asberg (1979) was used to measure depression. 17 Montgomery-Asberg Depression Rating Scale (MADRS) consists of 10 items; 1) apparent sadness; 2) reported sadness; 3) inner tension; 4) decreased sleep; 5) decreased appetite; 6) concentration problem; 7) lassitude; 8) inability to feel; 9) pessimistic thoughts, and 10) suicidal thoughts. Participants were asked to rate responses on a 7-point Likert scale ranging from “Not at all” (0) to “definitely” (6), with higher scores indicating more severe depression and vice-versa. Further, the total scale score was also categorized into normal (0–6), mild (7–19), moderate (20–34), and severe and very severe (>34) for SD. The scale has an excellent reliability index (r = 0.93) and an intraclass coefficient of 0.96, indicating an excellent test-retest reliability. 18
Sample Size Analysis
The sample size was calculated considering the prevalence of SD in an earlier Indian study. 19 A sample size considering 42.5% expected prevalence and 10% margin of error was used to calculate the survey and was 94. Initially, 110 participants enrolled in the work and reported dropout (n = 14) at the end of the work. Further, the authors followed the participants at home or insisted telephonically on attending the follow-up to achieve the estimated sample size.
Ethical Consideration
The Institutional Ethics Committee approved the project (AIIMS/IEC/21/508). A consent form was supplemented with the questionnaire as a mandatory requirement to participate in the survey. However, researchers refrain from collecting any personal information of the participants during the study.
Data Analysis
Data are transferred to a Microsoft Excel sheet and analyzed using SPSS version 23.0. Descriptive statistics used frequency, percentage, means, and standard deviation. An independent sample t test was applied to see the changes in sexual function and depression from baseline to 4 weeks’ follow-ups. All test statistics are measured at P < .05 level (2-tailed).
Results
Table 1 depicts the sociodemographic characteristics of the study participants. The participants’ mean age was 35.87 (±5.10) years. In terms of religion, 61.7% of the participants belonged to the Hindu religion and 28.7% were Muslim.
Sociodemographic Characteristics of Participants (N = 94)
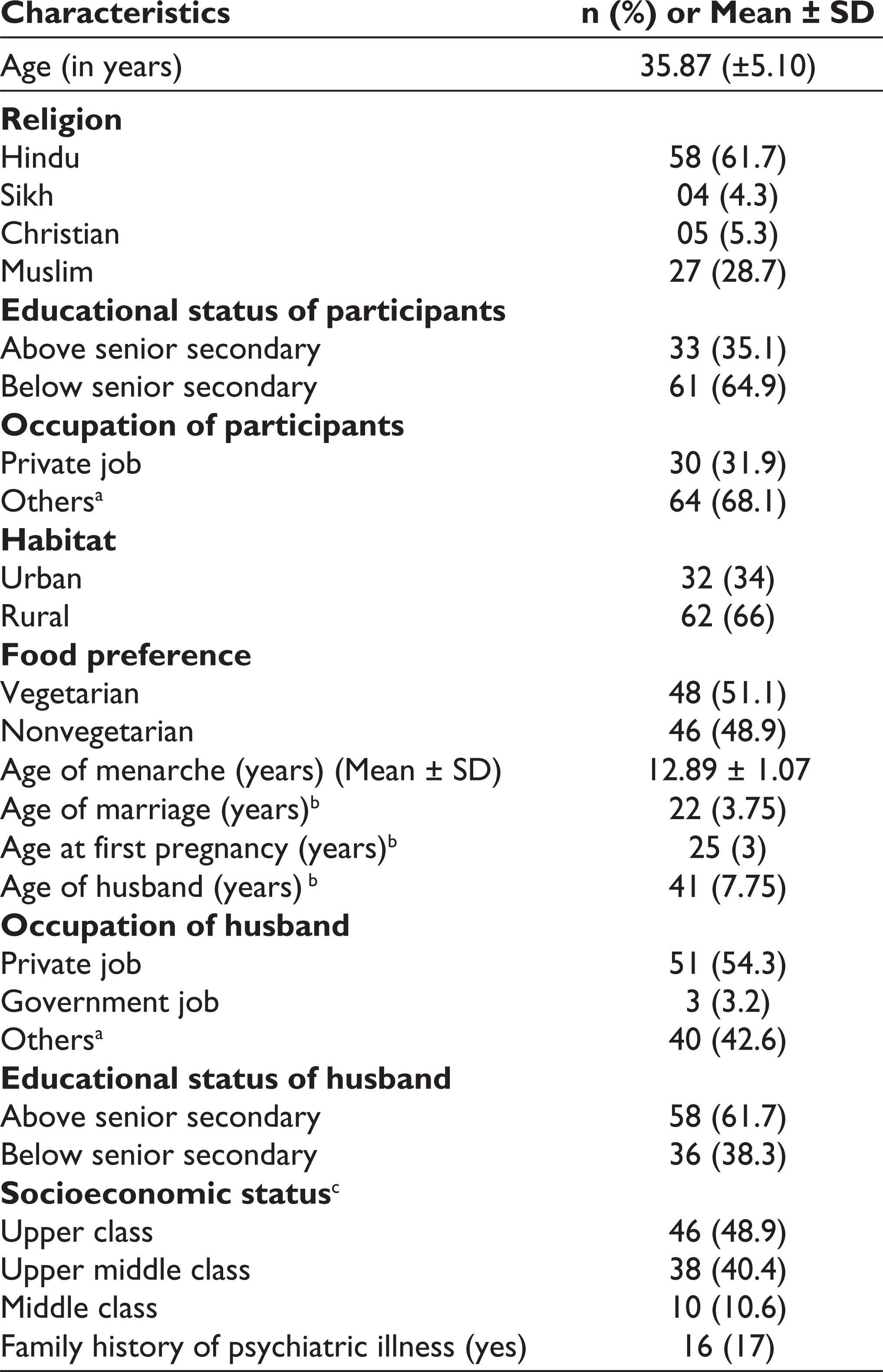
Further, the educational status of 35.1% of participants was above senior secondary level, and 64.9% were educated up to senior secondary level. In terms of the participants’ occupations, 31% were private employees and 68.1% were involved in farming and labor. More than half of the participants (66%) lived in a rural area and 34% belonged to an urban area. Regarding food preference, 51.1% of the participants were vegetarian and 34% were nonvegetarian.
The mean age of the menarche of the participants was 12.89 (±1.07) years, and the median of marriage was 22 ([interquartile range] IQR: 3.75) years. The median age at first pregnancy was 25 (IQR: 3) years. Likewise, 17% of the participants reported a family history of psychiatric illness and belonged to the upper class (8.9%) as per BG Prasad Socioeconomic Scale 2019. 20
For husbands, the median age was 41 (IQR: 7.75) years, 54.3% worked in private jobs and 42.6% had some of their own business, including farmer, laborer, and shopkeeper (Table 1).
Prevalence of Depression and SD
Prevalence of depression and sexual function are measured at baseline and 4 weeks of follow-ups. Findings revealed that 33% of participants reported severe depression and the remaining 67% were mild to moderate depression. Further, in SD, 95.7% of the participants reported disturbances in one or other sexual functions. In terms of domains of sexual function, 100% of participants complained of disturbances in sexual arousal, lubrication, achieving orgasm, and pain during sexual intercourse at baseline, which was improved to 97.9% in arousal and pain (96.8%) at 4 weeks of antidepressant therapy. Though, these findings look absurd and surprising and need to be validated using other suitable designs, that is, longitudinal or phenomenological study, in the future. This may be presumed because of sensitive topics and hesitation among participants to talk about sexual functions freely, conservative nature, and prevalent taboos about sexual health in the Indian subcontinent for such distinct findings in work. Variations in the results need further research to reach a specific conclusion about sexual functions in women with depression. However, it is also a matter of research to explore the impact of a different kind of specific antidepressant drug on sexual function among women with depression. The authors recommend a large-sample multicentric study is needed to determine the prevalence of each SD in the population in hilly areas.
Effects of Antidepressants Therapy on Depression and Sexual Function
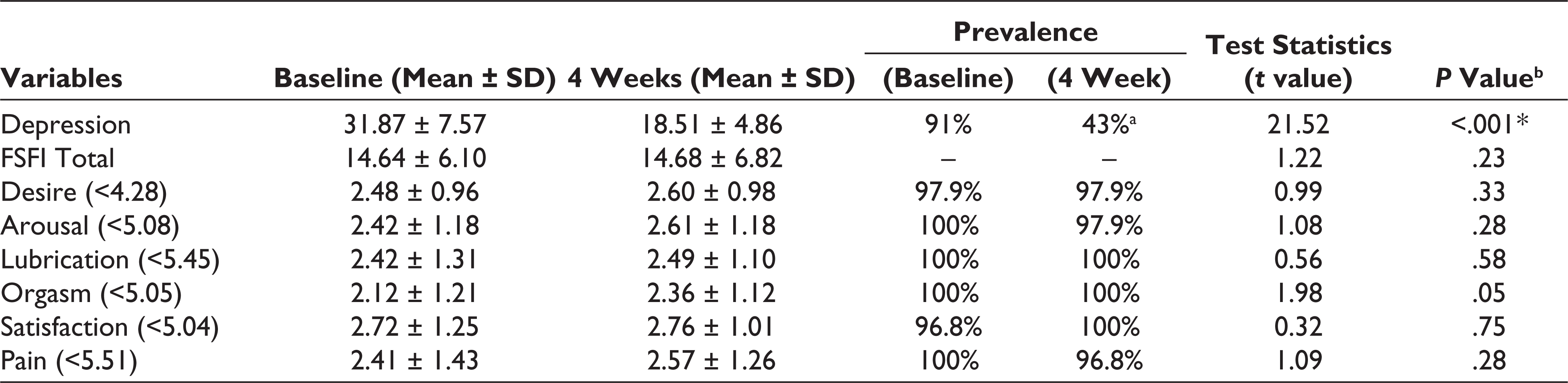
Table 2 displays the mean and standard deviation of the SD and depression at baseline and 4 weeks of the treatment. The finding reported a significant change in depression at (P = <.001) 4 weeks of interval (18.51 ± 4.86) from baseline depression (31.87 ± 7.57). However, there were no significant changes observed in SD simultaneously (4 weeks) (P = .23). The higher sexual function was reported in the orgasm domain (2.36 ± 1.12), followed by lubrication (2.49 ± 1.10). However, there were no significant changes in the mean domains scores of FSFI at baseline to 4 weeks of follow-ups in the study cohort, indicating the need for more time to improve sexual function and suggesting future extensive sample size research (Table 2).
Changes in Depression and Sexual Function From Baseline to 4 Weeks (N = 94)
Correlation of Depression With SD
The MADRS scores show a significant negative correlation with different domains of FSFI scores at baseline and 4 weeks of follow-ups on correlation analysis. It reveals that depression and SD are negatively related at baseline (r = −.412, P < .00) and 4 weeks (r = .412, P < .001) of follow-ups (Table 3).
Correlations Between Scores of MADRS and FSFI at Baseline and 4 Weeks (n = 94)

Discussion
This study was conducted to assess sexual function and change of depression among women at 4 weeks at a tertiary care center in North India. Female sexual dysfunction (FSD) remains undiagnosed, considering the complex sociocultural barriers and taboos compared to males around the globe. 21
The present study reported a high prevalence of SDs in women with depression. The findings revealed 95.7% of SD at the baseline, higher than the previous study that reported 90% SD in women with depression taking antidepressant therapy. 22 Likewise, another study reported the prevalence rate of SD among females taking antidepressant treatment to vary from 2% to 82%. 3 Studies from India have reported a higher prevalence of SD ranging from 46.66% to 73.3% when the Arizona Sexual Experience Scale (ASEX) scores are considered and 40% to 70.3% when the SD is measured using total FSFI.23,24 However, rates of SD vary in different studies depending on the heterogeneous study population, assessment methods, time of assessment, and type of SD around the globe.25–27 In comparing our findings with previous studies, the prevalence reported in our study is higher than the reported range.
The present study reported a significant negative relationship between depression and sexual function, which is concurrence with the earlier Indian work conducted in Maharashtra, which conveyed a strong link between SD and depression. 28 Notably, studies from India reported SD in a significant proportion of the patients with depression receiving antidepressants.24,25 However, the prevalence of FSD is higher in advanced age (>40 years) as compared to younger age cohort. 26
Studies from Western countries have also reported a higher prevalence of sexual disorders in depressed participants concurrent with our study findings.29,30 Authors speculate that depression is associated with low self-esteem, feelings of hopelessness, hormonal disturbances, and negative self-evaluation as a reason for sexual impairment. These findings strongly suggest a mandatory screening of all the patients with depression for the possible sexual impairments in a clinical setting.
In terms of various aspects of sexual functioning, higher prevalence is reported for the elements of sexual functioning lubrication (100%), orgasm (100%), and satisfaction (100%). Compared to problems in these sexual domains, dysfunction in other sexual aspects is less commonly reported, including desire (97.9%), arousal (97.6%), and pain (96.8%). The prevalence of SD is relatively higher in our work than in previous work that reported a higher prevalence in sexual desire (83%) and sexual desires and fewer dysfunction in other aspects of sexual function.4,31 Likewise, studies from India that used FSFI reported a prevalence of up to 90% in the sexual desire domain followed by sexual arousal (86%), decreased orgasm (68%), reduced satisfaction (62), a problem with lubrication (54%), and painful intercourse (32%). 23 Furthermore, in another study prevalence of SD was slightly lower, including lubrication problem (53%), organic dysfunction (51%), painful intercourse (49%), low desire, sexual satisfaction, and arousal dysfunction (45%). 32 However, very contrasting findings on sexual function need future research attention and indicate a large multicentric work to reach a specific conclusion.
All aspects of sexual functioning were impaired in our study participants, including problems in lubrication, difficulties achieving orgasm, pain, low desire, low arousal, and low satisfaction. These findings are in line with the previous study from Southern states of India that women attending general medical clinics reported difficulties with desire (78%), arousal (91%), lubrication (97%), orgasm (87%), problems with pleasure (81%), and pain (64%). 26 Further, studies using ASEX reported the highest prevalence in the sexual aspect of desire or drive (47.9–81.7%), lubrication (35.2–76.05%), achieving satisfaction (18.3–60.56%), and problems in reaching orgasm during sex (18.3–50.7%). 33 Further, 60.56% to 90.1% of the participants reported dysfunction in one of the more sexual domains. 33 These findings are in line with the work of Singh et al 26 who said that women attending general medical clinics said reduced desire (78%), arousal (91%), problems in lubrication (97%), trouble achieving orgasm (87%), issues with pleasure (81%), and pain (64%). These findings are comparable to our work and existing literature.25,34 Contrasting differences in the findings need further research to reach a specific conclusion regarding the high prevalence of SD in women with depression.
A previous study conducted on a group of patients by Montejo et al 35 revealed the side effects of antidepressants on SD. Further, after 6 months, 55% still had at least some type of SD, including 90% had decreased libido and 86% decreased arousal in another earlier work. In the present study, 95% of participants still reported SD after 4 weeks of treatment with antidepressants. Authors speculate the variations in the findings in light of the low sample size, use of the different methodology in studies, use of other assessment tools, development and validation of FSFI on Western population, and cultural variation. This variation in findings warrants an extensive multicentric investigation using an instrument from an Indian setting to generalize the results.
Further, it has been reported in previous research that only a handful of patients (13.3%) discussed their SD with their treating psychiatrists. 33 Similarly, in another last work, this proportion was low (14%), which rose to a staggering 58% when doctors actively asked for the information. 35 These findings necessitate an imperative need to evaluate all patients for SD diagnosed with depression on a routine basis.
Limitations and Recommendations
This study has certain limitations, which must be kept in mind while interpreting and extrapolating the study’s findings. The study sample size was relatively small and did not include a control group, which may impede the results’ generalization. A large and multicentric study would throw more light on the extent of SD in women with depression. Furthermore, the study findings are self-reported on sexual functions, which is subjective and may have chances of reporting bias and accuracy. We did not study dose- and drugs-specific changes in sexual function; hence, the prevalence of SD, as reported in this study, for antidepressants cannot be generalized to a particular antidepressant. The study instruments are developed and validated on the Western population and hence may over or under present the findings on SD, which must be taken care of the future researchers.
Future multicentric studies must carry out on a large population to better understand the effect of specific antidepressants on sexual functions. For health-care institutes, it is recommended to provide best practices by assessing sexual functions among every depressed woman and for best policies of community education through health education. This will help improve the patients’ compliance and quality of life on the antidepressant.
Conclusions
The prevalence of SD is high in the study cohort. All dimensions of sexual function are impaired in depressed women. Again, rates of SD with antidepressant use are very high. The present study shows a significant negative relationship between sexual function with depression. Further research is needed to explore this area of research in the future to improve treatment adherence and the quality of life of the patients.
Author Contribution
SC: Concept, the definition of intellectual content, data curation, writing the manuscript, and review the draft; RK: Data analysis, preparation of tables, and approval of final draft. The author works as a guarantor and will correspond with the journal from this point onward; JR: Concept, the definition of intellectual content, and data curation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.