
Abstract
Introduction:
Sexual dysfunction (SD) is a significant but often-overlooked complication among women with Type 2 diabetes mellitus (T2DM). This study aimed to examine the prevalence and severity of SD among women with T2DM attending the diabetes clinics of the teaching hospitals in Ogun State, Nigeria.
Methods:
A descriptive cross-sectional study was conducted among 90 women with T2DM attending the diabetes clinics of two teaching hospitals. Data were retrieved using a validated questionnaire comprising socio-demographic characteristics, the female sexual function index (FSFI), and the Female Sexual Distress Scale-Revised (FSDS-R). Descriptive and inferential (ANOVA) were used for data analysis at a 0.05 level of significance.
Results:
The prevalence of SD was exceptionally high, with 86.7% of respondents experiencing some degree of dysfunction. Arousal (mean = 2.63 ± 1.4) and orgasm (mean = 2.67 ± 1.5) were the most affected domains. Additionally, 81.1% of respondents experienced high sexual distress, with a mean FSDS-R score of 19.9 ± 1.9. Sexual distress was significantly associated with age (F = 33.12, df = 2.87, P < .001), education (F = 8.13, df = 2.87, P = .001), diabetes duration (F = 10.90, df = 2.87, P < .001), hypertension (F = 83.71, df = 1.88, P < .001), and treatment type (F = 45.56, df = 2.87, P < .001).
Conclusion:
This study reveals a high burden of SD and distress among participants. Older age, higher education, longer diabetes duration, hypertension, and complex treatment regimens significantly influence the severity of dysfunction. Therefore, routine assessment of sexual health should be integrated into diabetes care, and targeted interventions are essential to address this neglected aspect of women’s health.
Keywords
Introduction
Diabetes is a significant, long-lasting health condition that develops when blood sugar (glucose) levels become elevated due to the body’s inability to produce adequate insulin, produce any at all, or use the insulin it makes effectively. Insulin is key in the movement of glucose from the blood into the body’s cells, where it is used for energy or stored for later use. Also, insulin plays a key role in processing proteins and fats. When the body lacks insulin or cannot respond to it appropriately, glucose builds up in the bloodstream, resulting in hyperglycemia, the main sign of diabetes. 1
Globally, around 589 million adults between 20 and 79 years old-about 11.1% of adults in this age group, are estimated to have diabetes. By 2050, this number is expected to rise to 852.5 million. 2 Approximately 252 million adults with diabetes do not know they have it. Among those diagnosed, one in four (158 million) are over 65. Additionally, about 635 million adults aged 20-79 (12%) have impaired glucose tolerance. In 2024, over $1 trillion was spent on diabetes care, accounting for 12% of worldwide health spending. Diabetes led to more than 3.4 million deaths in 2024, which is 9.3% of all global deaths.
In 2024, there were an estimated 9.15 million people worldwide diagnosed with Type 1 diabetes (T1D), with 22.3% (2.04 million) living in low- and lower-middle-income countries. Of these, 1.81 million (19.8%) were under 20 years old, 6.28 million (68.6%) were aged 20-59, and 1.06 million (11.8%) were 60 or older. 3 Type 2 diabetes is the most prevalent form, making up over 90% of cases globally. It is currently the eighth leading cause of disease burden worldwide and is projected to become the second leading cause by 2050. 3 About one in five births (23 million) are affected by some type of high blood sugar during pregnancy. 2
While the global population is expected to grow by 25% over the next 25 years, the number of people with diabetes is anticipated to increase by 45%. Notably, 95% of this rise will occur in low- and middle-income countries, where population growth is outpacing that of high-income nations. 2 In Africa, one in 20 adults (about 25 million people) has diabetes. By 2050, this figure is expected to jump by 142% to 60 million, the most significant percentage increase among all IDF regions. Four out of five adults (73%) with diabetes in Africa are undiagnosed, the highest rate globally. Diabetes caused 216,000 deaths in Africa in 2024. The continent also has the lowest diabetes-related healthcare spending, at $10 billion, representing just 1% of global expenditure. One in seven births in Africa is affected by high blood sugar during pregnancy. According to the IDF, Nigeria is among the top five countries for the number of adults (aged 20-79) with diabetes, with an estimated 3 million cases in 2024, projected to rise to 6.6 million by 2050. 2
Persistently high blood glucose levels, if not properly managed, can gradually harm multiple organs in the body. This damage can result in serious and potentially life-threatening complications, including cardiovascular diseases, nerve damage (neuropathy), kidney disease (nephropathy), lower-limb amputations, and eye problems (retinopathy), leading to vision loss or blindness. In addition, diabetes is increasingly being linked to other complications such as cognitive decline, liver disease, cancer, and frailty. However, maintaining blood glucose close to normal levels can help delay or even prevent many of these severe complications.1,4
Among the many complications of diabetes, sexual dysfunction (SD) in women with Type 2 diabetes mellitus (T2DM) is a significant but often-overlooked issue worldwide. Although diabetes is widely recognized as a chronic condition with multiple complications, its impact on women’s sexual health is still insufficiently addressed in both clinical practice and research, particularly in African settings. Female sexual dysfunction (FSD) is characterized by persistent or recurring problems with sexual desire, arousal, pain during intercourse (dyspareunia), and difficulty or inability to achieve orgasm. 5 Research indicates that women with T2DM are more likely (71.03%) to experience SD. 6 The prevalence of FSD among women with T2DM ranges from 20% to 80%, compared to about 40% in the general female population, with some recent studies reporting rates as high as 87%.7,8
The causes of SD in women with T2DM are complex and multifactorial. Biological mechanisms include hyperglycemia, insulin resistance, chronic low-grade inflammation, endothelial dysfunction, nerve damage, and hormonal imbalances. These factors can affect genital blood flow, nerve signalling, and vaginal lubrication, all of which are important for normal sexual response.5,9 As a result, women may experience decreased libido, difficulties with arousal and lubrication, problems achieving orgasm, pain during sex, and overall reduced sexual satisfaction.
In addition to physiological factors, a range of psychosocial issues can contribute to SD in women with T2DM. These include depression, anxiety, negative body image, relationship problems, and side effects from medications. Cultural beliefs and societal attitudes about sexuality and diabetes can further intensify feelings of guilt, stigma, and low self-esteem.5,9 FSD can affect women of all ages, including those of reproductive age, perimenopausal, menopausal, and postmenopausal women. The interplay between biological and psychosocial factors is complex and varies between individuals, cultures, and even within the same person over time. 10
FSD can be classified as primary or secondary. Primary FSD is not caused by any medical, psychiatric, or substance-related condition, whereas secondary FSD is. The choice of assessment tool is important, as different questionnaires evaluate sexual function over varying timeframes and populations. For example, the Arizona Sexual Experience Scale (ASEX) assesses sexual function over the past week, while the female sexual function index (FSFI) covers the previous month. 11
Despite the growing evidence, there is limited data on the prevalence and severity of SD among women with T2DM in Nigeria, specifically in Ogun State. Cultural taboos, stigma, and a general lack of awareness often cause many women with diabetes to keep their sexual health struggles hidden, leading to underreporting and neglect of these important issues. 12 In addition, due to the subjective nature of the problem, many healthcare providers may not be adequately equipped or feel comfortable discussing SD, which means these problems may frequently go undiagnosed and untreated. 13
This gap in knowledge and care can create a barrier to truly comprehensive diabetes management and can have a profound adverse effect on women’s overall health and well-being. Therefore, the current research focuses on examining the prevalence and severity of SD among women living with T2DM in Ogun State.
Methodology
A cross-sectional study at the teaching hospitals in Ogun State was conducted. Samples were taken only from women with T2DM attending the diabetes clinic in the teaching hospitals, Ogun State, Nigeria, for the last three months, willing to participate in the study. The purposive sampling technique was utilized. A total of 100 samples were screened during the period of data collection, and 90 samples were included in the study.
Inclusion Criteria
Women diagnosed with Type 2 diabetes for at least 3 months. Women diagnosed with Type 2 diabetes were between 18 and 65 years old. Women diagnosed with Type 2 diabetes and sexually active in the last 6 months. Women diagnosed with Type 2 diabetes who consented to the study.
Exclusion Criteria
Women diagnosed with Type 2 diabetes who are critically ill in a hospital bed. Women diagnosed with Type 2 diabetes who had a record of mastectomy, bilateral hysterectomy-oophorectomy, heart failure, and any other underlying pathology.
Questionnaire
The instrument for data collection was a validated questionnaire, which was divided into three sections:
Section A—The Socio-demographic characteristics and Clinical Factors: This section contained seven items in total, which are age, ethnicity, religion, marital status, duration of diabetes, Hypertension, and type of diabetes treatment.
Section B—Prevalence of SD (using the FSFI Scale): The FSFI is a 19-item self-report test of female sexual function that yielded scores on both the major components of sexual function in women and overall levels of sexual function, including arousal, orgasm, pain, satisfaction, and sexual desire. The 19 items of the FSFI use a 5-point Likert scale ranging from 1 to 5, with higher scores indicating better sexual functioning on the respective item. 14 To score the measure, the sum of each domain score is first multiplied by a domain factor ratio (0.6 for desire, 0.3 for arousal, 0.3 for lubrication, 0.4 for orgasm, 0.4 for satisfaction, and 0.4 for pain) in order to place all domain totals on a more comparable scale, and a total FSFI score is subsequently derived by addition of all. 14 Fifteen (15) of the items contain a zero option in the response set to indicate either “no sexual activity” (12 items) or “did not attempt intercourse” (3 items) within the past 4 weeks. The score ranges from 2 to 36, with 36 being the maximum score, indicating better functioning, and two being the minimum score, which indicates poor function. The cut-off score is 26.5, which is used to diagnose FSD. Scores less than 26.5 are taken as an indicator of SD.
Section C—Severity of SD (Measured by the Female Sexual Distress Scale-Revised [FSDS-R]): The FSDS-R is a carefully developed and validated tool designed to measure the emotional distress women experience related to problems with sexual function. Initially, the FSDS was tested on 500 women, resulting in a reliable 12-item questionnaire that effectively captured this distress as a single, consistent dimension. 15 Building on this, researchers created an updated 13-item version—the FSDS-R, which demonstrated strong reliability and validity. This revised scale is particularly useful for identifying women experiencing hypoactive sexual desire disorder and is a screening tool to distinguish between women with higher or lower levels of sexual functioning. 16
In the FSDS-R, women respond to each of the 13 items by indicating how often they experience certain feelings or problems, using a scale from 0 (never) to 4 (always). The responses are then added together to produce a total score that ranges from 0 to 52. Higher total scores reflect greater levels of sexual distress. Clinically significant distress is typically indicated by a score of 11 or higher. 17
Method of Data Analysis
The data was screened and checked for missing data and outliers. The collected data were analyzed using Statistical Product and Service Solutions (SPSS) version 27. Descriptive (mean and standard deviation) and inferential (one-way Analysis of Variance [ANOVA]) statistics were conducted to determine whether levels of sexual distress, as measured by the FSDS-R, varied significantly across selected socio-demographic and clinical variables among female respondents living with diabetes (N = 90). The level of significance was set at 0.05.
Ethical Considerations
Administrative permission from the Research Health Ethical Committee was obtained - (BUHREC684/24). Informed consent was obtained from the entire participants.
Results
Out of 100 individuals screened and meeting the inclusion criteria during the data collection period, 90 participants took part in the study, yielding a response rate of 90%. The analysis presented is therefore based on data obtained from these 90 eligible respondents.
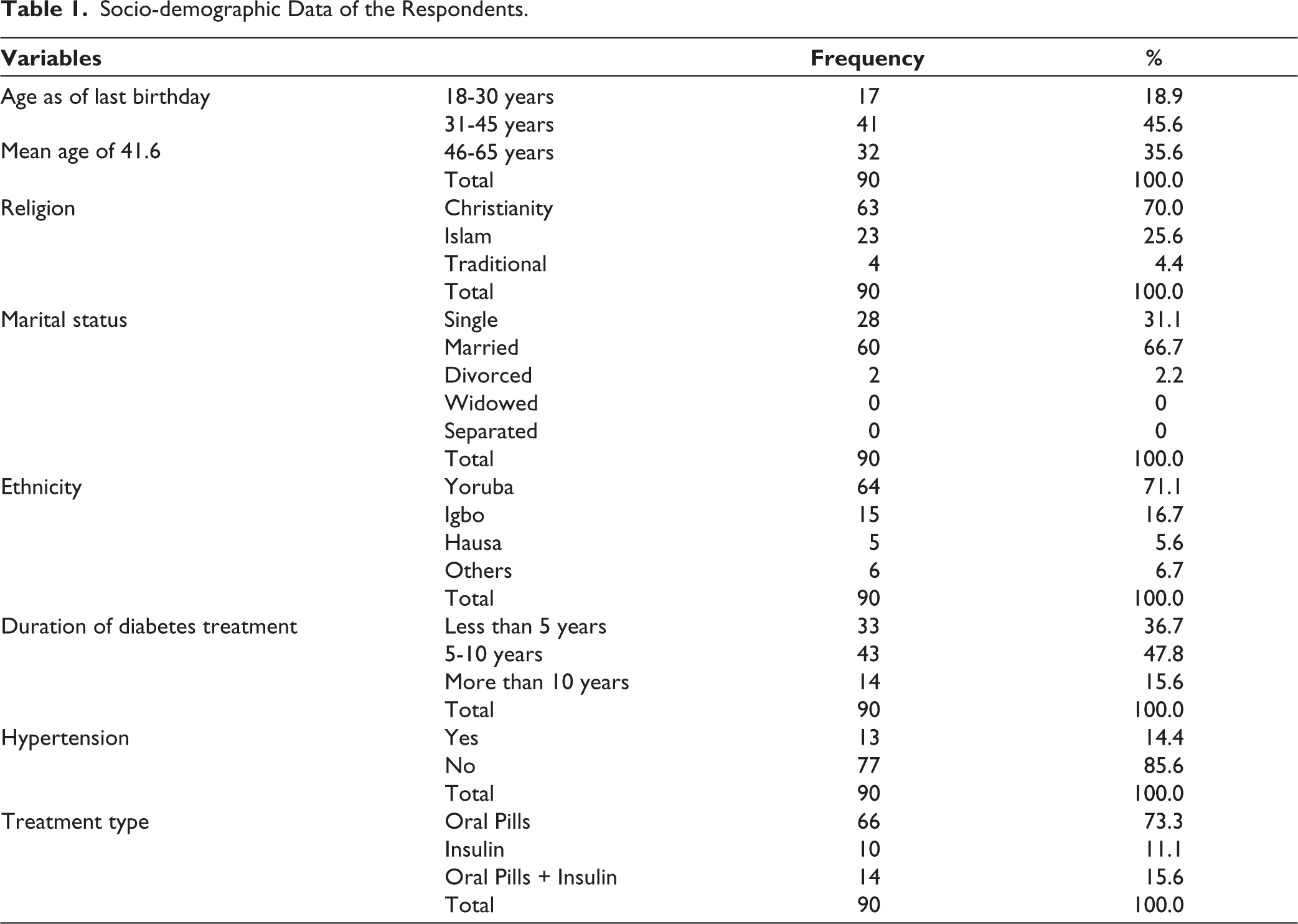
Table 1 revealed that a total of 90 respondents participated in the study, with 18.9% between 18 and 30 years, 45.6% aged 31 to 45 years, and 35.6% between 46 and 65 years. The mean age of the participants was 41.6 years. Regarding religion, the majority of respondents identified as Christians (70.0%), followed by Muslims (25.6%), while 4.4% practiced traditional religions. Most participants were married (66.7%), with 31.1% single, 2.2% divorced, and no respondents reported being widowed or separated. The largest group was Yoruba, which comprised 71.1% of the sample. The Igbo accounted for 16.7%, Hausa 5.6%, and other ethnic groups made up 6.7%. Concerning the duration of diabetes treatment, 36.7% of respondents had been on treatment for less than 5 years, 47.8% for 5 to 10 years, and 15.6% for more than 10 years. In addition, out of the 90 respondents included in the study, the majority (n = 77; 85.6%) did not have a diagnosis of hypertension, while 13 participants (14.4%) reported having comorbid hypertension. Regarding the type of diabetes treatment, most participants (n = 66; 73.3%) were being managed with oral hypoglycemic agents alone. A smaller proportion were exclusively on insulin therapy (n = 10; 11.1%), while 14 participants (15.6%) received a combination of oral pills and insulin.
Socio-demographic Data of the Respondents.
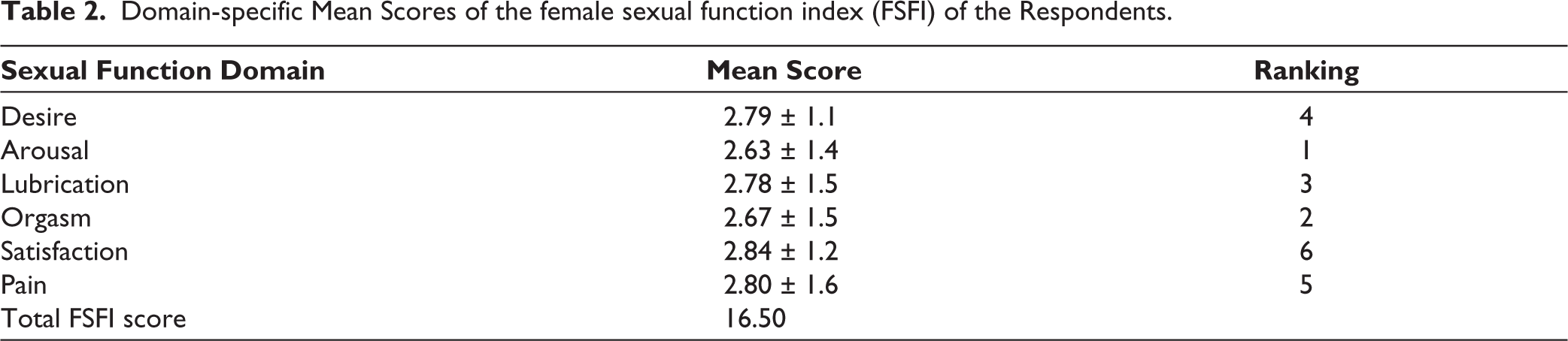
From Table 2, the analysis of the FSFI scores among respondents revealed that sexual arousal was the most affected domain, with a mean score of 2.63 (±1.4), this was followed by orgasm, which recorded a mean score of 2.67 (±1.5). Lubrication was the third most affected domain, with a mean score of 2.78 (±1.5), followed by sexual desire, ranked fourth, with a mean score of 2.79 (±1.1), and pain, with a mean score of 2.80 (±1.6), was the fifth most affected domain. Satisfaction was the least affected domain despite having the highest mean score of 2.84 (±1.2), which was still below the normal threshold.
Domain-specific Mean Scores of the female sexual function index (FSFI) of the Respondents.
The prevalence of SD among the respondents was notably high. Based on the FSFI threshold score of 26.55, about 78 (86.7%) were categorized as experiencing SD, while only 12 respondents (13.3%) maintained normal sexual function (Table 3).
Prevalence of Sexual Dysfunction Among the Respondents.

These findings indicate a high burden of SD within the studied population, with arousal being the most affected domain.
The analysis of sexual distress among respondents using the FSDS-R revealed varying levels of distress across multiple aspects of sexual experience (Table 4). The most frequently reported issue was feeling sexually inadequate, with 46 respondents (51.1%) indicating they rarely experienced this feeling, while 24 respondents (26.7%) experienced it occasionally. Distress about sex life was also notable, with 36 respondents (40.0%) experiencing it rarely and 17 respondents (18.9%) always feeling distressed. Feelings of unhappiness about sexual relationships were reported by 28 respondents (31.1%) as a rare experience, and 19 respondents (21.1%) experienced this occasionally or frequently. Additionally, 36 respondents (40.0%) felt guilty about sexual difficulties rarely, while another 16 respondents (17.8%) experienced guilt occasionally and frequently. Frustration with sexual problems was evenly distributed, with 28 respondents (31.1%) each reporting never or rarely feeling frustrated, and 16 respondents (17.8%) experiencing it frequently.
Sexual Distress Among the Respondents (FSDS-R Scale).
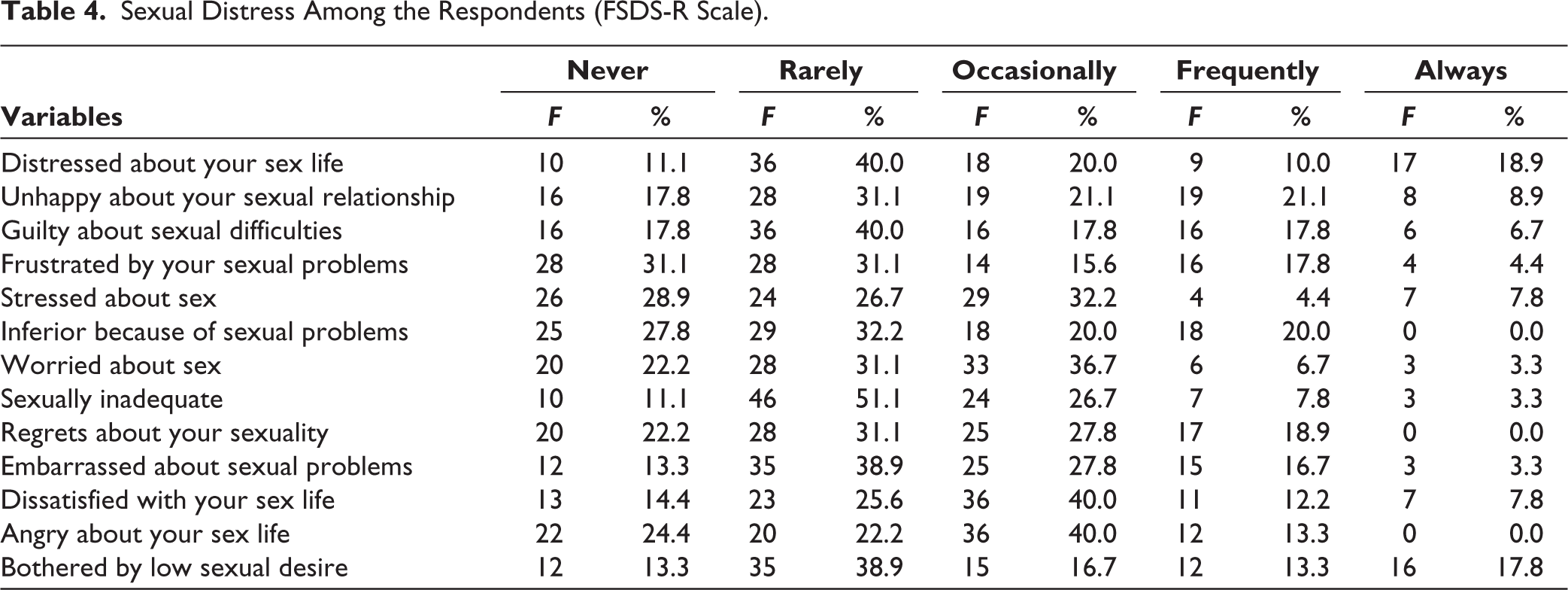
The results further showed that 29 respondents (32.2%) were occasionally worried about sex, while 33 respondents (36.7%) reported being occasionally worried. In terms of feeling inferior due to sexual problems, 29 respondents (32.2%) rarely experienced this, while 18 (20.0%) experienced it occasionally or frequently. Satisfaction was low, with 36 respondents (40.0%) feeling dissatisfied with their sex life occasionally and 12 respondents (13.3%) feeling this way frequently.
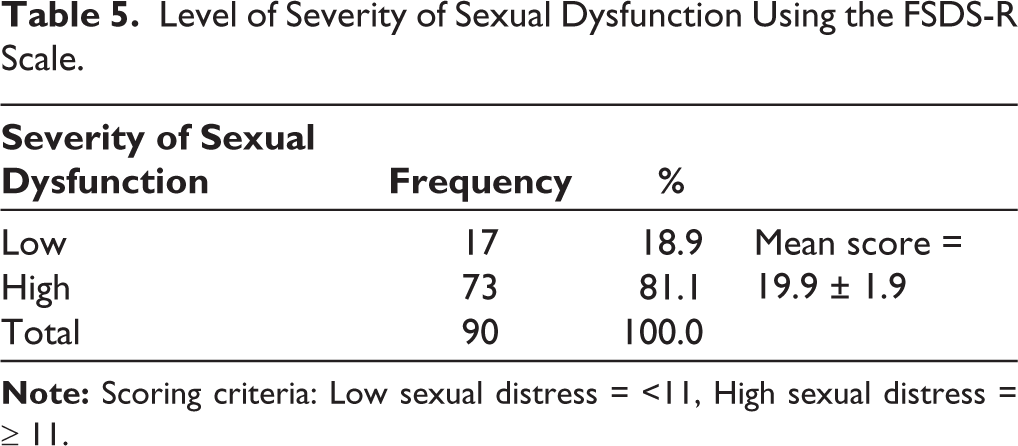
The severity of SD among respondents, determined using the FSDS-R Scale, showed that a majority, 73 respondents (81.1%), experienced high sexual distress (≥11), while only 17 respondents (18.9%) had low sexual distress (<11), with an overall mean score of 19.9 ± 1.9. (Table 5) This finding underscores a high prevalence of significant sexual distress among the study population.
Level of Severity of Sexual Dysfunction Using the FSDS-R Scale.
One-way Analysis of Variance (ANOVA) was used to determine whether levels of sexual distress, as measured by the FSDS-R, varied significantly across selected socio-demographic and clinical variables among female respondents living with diabetes (N = 90). The FSDS-R mean scores, category frequencies, and ANOVA results are presented in Table 6.
One-way ANOVA Summary of FSDS-R Total Scores by Socio-demographic Characteristics (N = 90).
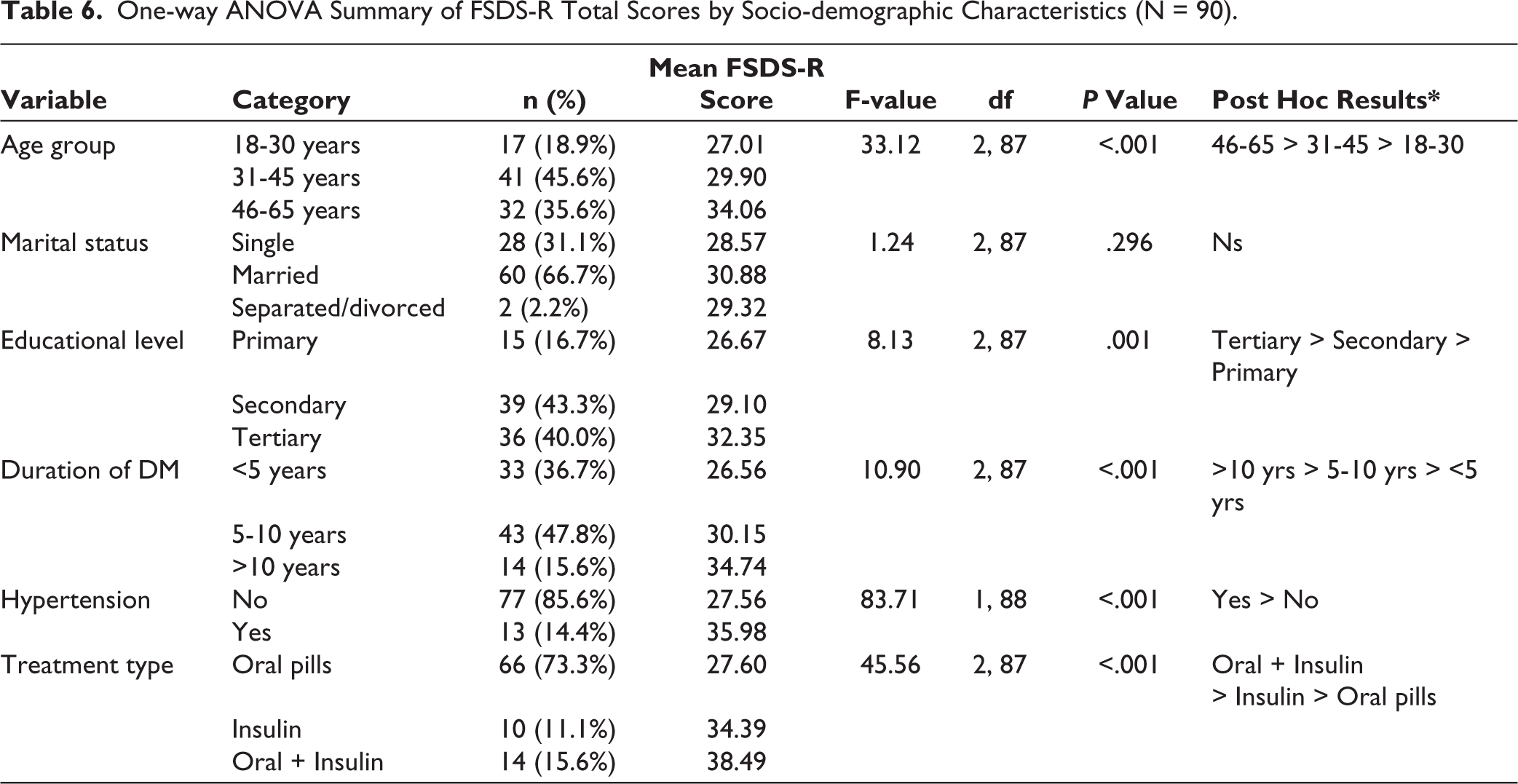
There was a statistically significant difference in FSDS-R scores among age groups: F(2, 87) = 33.12, P < .001. Respondents aged 46-65 years reported the highest mean score (M = 34.06), followed by those aged 31-45 years (M = 29.90) and 18-30 years (M = 27.01). Post hoc comparisons using Tukey’s HSD test showed that the differences between the oldest age group and the other two groups were statistically significant (P < .05), suggesting increased sexual distress with advancing age. The FSDS-R scores varied significantly by educational attainment: F(2, 87) = 8.13, P = .001. Respondents with tertiary education reported the highest level of sexual distress (M = 32.35), followed by those with secondary (M = 29.10) and primary education (M = 26.67). Tukey’s post hoc analysis confirmed statistically significant differences between tertiary and both secondary and primary education groups (P < .05), indicating a possible association between higher education and increased awareness or reporting of sexual distress.
The duration of diabetes treatment was significantly associated with FSDS-R scores: F(2, 87) = 10.90, P < .001. Participants who had lived with diabetes for more than 10 years had the highest mean sexual distress scores (M = 34.74), compared to those with 5-10 years (M = 30.15) and less than 5 years (M = 26.56) of diagnosis. Post hoc testing showed significant differences between the >10 years group and the other two duration groups (P < .05), suggesting increasing sexual distress with longer disease duration. There was a highly significant difference in FSDS-R scores between respondents with and without hypertension: F(1, 88) = 83.71, P < .001. Those with hypertension reported markedly higher levels of sexual distress (M = 35.98) compared to non-hypertensive individuals (M = 27.56), indicating that comorbid hypertension is associated with greater SD distress.
In addition, significant differences were observed in FSDS-R scores across the three treatment groups: F(2, 87) = 45.56, P < .001. Respondents on combined therapy (oral + insulin) reported the highest sexual distress (M = 38.49), followed by those on insulin alone (M = 34.39), and those on oral medications only (M = 27.60). Tukey’s post hoc comparisons confirmed that all group differences were statistically significant (P < .05), suggesting a strong relationship between treatment complexity and sexual distress.
These findings underscore the influence of age, educational status, duration of illness, hypertension comorbidity, and treatment type on female sexual distress among individuals living with diabetes.
Discussion of Findings
In the present study, the mean age is 41.6, and the majority fall within the age range of 31-45 years. A much older age distribution was spotted in a study by Asefa et al. 18 where the majority of the patients are between 41 and 50 years old. This high age distribution could be linked to the disease distribution of diabetes, as it is common in older people compared to the young demographic. Marital status data shows that the majority are married. This finding is supported by a study by Kamrul-Hasan et al. 19 where the majority of the women are also married.
The prevalence of SD among female Type 2 diabetic patients in this study was 86.7%. This prevalence rate is notably higher than the 79% reported by Kamrul-Hasan et al. 19 in Bangladesh and 62% reported by Onung et al. 20 in a Nigerian study. In contrast, Masood et al. 21 reported a much lower prevalence of 43.2%, which may reflect regional differences in awareness, cultural attitudes toward sexual health, or the effectiveness of diabetes management. The variations seen across these studies may be influenced by factors including the duration of diabetes, comorbidities, and differences in how sexual health concerns are reported or managed.
The specific domains of sexual function most affected in this study were arousal and orgasm, a pattern that may be linked to the physiological and psychological impacts of diabetes. Neuropathy, reduced blood flow, and hormonal imbalances could impair arousal, while stress and self-esteem issues may further hinder orgasmic responses. These findings contrast with Cauwenberghe et al. 22 who reported decreased desire and arousal as the most affected domains, possibly due to cultural and demographic differences. Similarly, Saraswati et al. 23 identified hypoactive sexual desire disorder as the most common dysfunction, with sexual pain disorder being the least affected, further emphasizing how a complex interplay of physiological, psychological, and socio-cultural factors shapes SD in diabetic populations.
The severity of SD measured by the FSDS-R revealed that the majority (81.1%, mean score: 19.9 ± 1.9) of the respondents experienced high sexual distress. This finding is notably higher than what has been reported in other studies. For instance, Zheng et al. 24 in Australia reported a prevalence of high sexual distress at 50.2%. In comparison, Hamzehgardeshi et al. 25 in Iran and Gupta et al. 26 in India reported even lower prevalences of 31.8% and 28%, respectively.
The marked difference in the prevalence of high sexual distress between this study and others could be attributed to several factors. First, the population of this study comprised only women with T2DM, a group known to be at higher risk of SD due to the chronic nature of the disease and its associated complications, such as neuropathy, vascular insufficiency, and hormonal imbalances. In contrast, the studies by Zheng et al., 24 Hamzehgardeshi et al. 25 and Gupta et al., 26 included mixed populations, not exclusively women with Type 2 DM, which may have accounted for their lower prevalence of sexual distress.
Furthermore, our study revealed a statistically significant association between age and the severity of SD among the participants. This result implies that as age increases, so does the severity of SD. This finding aligns with previous studies by Ayuk et al. 27 who reported a similar association in a case-control study conducted in Calabar, Nigeria, where older age was significantly associated with SD. Likewise, Yenice et al. 28 in a study involving 149 women with diabetes mellitus (DM), identified age as a significant independent predictor of FSD using multivariable regression analysis with the FSFI.
As women age, it is common to experience changes in sexual health, often driven by the body’s natural decrease in estrogen. This hormonal shift can lead to vaginal dryness and reduced tissue elasticity, making intimacy less comfortable and sometimes less satisfying. 29 For women living with diabetes, these age-related changes can become even more pronounced, as diabetes can accelerate damage to blood vessels and nerves, compounding issues like dryness, difficulty with arousal, and challenges achieving orgasm.30-32 These findings highlight the importance of recognizing age as a crucial factor when assessing sexual health in women with diabetes.
Furthermore, the present study showed that the participants with tertiary education reported higher sexual distress than those with secondary or primary education, with a significant difference across groups (F = 8.13, P = .001). The result of the present study is supported by previous studies, which highlight that higher educational achievement often correlates with greater symptom awareness and willingness to report sexual difficulties.33,34 The authors hypothesized that the result may have been because tertiary-educated women may face increased psychosocial stressors, including work-related pressures and heightened expectations that contribute to sexual distress. Conversely, underreporting due to cultural or educational barriers among less educated women may have been a challenge, which may have resulted in apparently lower sexual distress scores in these groups.
The impact of the duration of diabetes on sexual function is still arguable. The present study showed that the FSDS-R scores significantly increased with longer disease duration, with those having diabetes for more than 10 years reporting the highest distress. This concurs with existing literature that shows that the longer the duration of the disease, the higher the regimen-related distress.35,36 In a study by Islam, the correlation between diabetes distress and disease duration was very strong.37,38 Parsa et al. showed that the highest overall diabetes distress was observed in patients with a disease duration of more than 15 years. 39 On the contrary, some investigators have found poor correlation between sexual difficulty and diabetes duration.40,41
At present, it is difficult to answer exactly how diabetes impairs sexual function. Hypothetically, prolonged duration of diabetes can complicate the neuroendocrine pathway of the sexual response cycle due to the prolonged devastating impacts of diabetes on both neurologic and vascular systems. Such negative interaction may explain the higher mean sexual distress scores of those participants. However, the exact mechanism is still not established. Also, the daily self-control of diabetes and the treatment-related burden that patients experience over many years may lead to therapeutic burnout, a sense of chronic fatigue, and significantly contribute to distress.42,43
Women with comorbid hypertension reported significantly higher sexual distress with FSDS‑R scores than those without hypertension. While past literature has questioned the direct link between hypertension and FSD, and how high blood pressure affects women sexually is not well understood, 44 more recent studies suggest that hypertension can result in vaginal dryness and a decrease in sexual desire.45-47 Persistent elevation of blood pressure results in vessel wall changes, leading to decreased circulation in the peripheral vascular tissues of the body. The decreased genital blood flow as a result of atherosclerotic changes may lead to vascular insufficiency of both the clitoris and the vagina. And because sexual arousal is affected, this will no doubt lead to sexual desire being compromised. In addition, decreased pelvic blood flow can contribute to the development of fibrotic lesions in the smooth muscle tissue of the clitoris and vaginal canal, which in turn may reduce the responsiveness to sexual stimulation.45,48 Furthermore, antihypertensive therapy and vascular changes may impair female sexual function, which can decrease adherence to drug treatment.46,47
In the present study, women on combined treatment (oral antidiabetic pills plus insulin) reported the highest FSDS‑R scores, followed by those on only insulin alone and oral pills. This result finding is consistent with existing literature indicating that both insulin-treated and non-insulin-treated diabetic women were significantly more likely to report reduced overall sexual satisfaction compared to non-diabetic women, and problems with lubrication and orgasm were more common among insulin-treated diabetic women compared to non-diabetic women. 31 Also, a study by Tuncel et al. 49 revealed that SD was significantly higher among women receiving insulin therapy compared to those who were not. In contrast, a study by Entezari et al. 50 showed that in diabetic women, SD in subjects with oral treatment was significantly higher compared with insulin treatment.
Finally, marital status did not significantly impact the severity of SD, and this is inconsistent with prior research demonstrating that marital status was an independent predictor of FSD. The study further revealed that married women were 1.59 times more likely to have FSD than women who were not married. 51
Limitation
The small sample size is a limitation of this study. Due to stringent selection criteria, generalizability may be limited to a specific clinical group (patients with T2DM).
Conclusion
Sexual health is a critical component of general well-being, yet it remains an often-neglected aspect of diabetes care. Our study revealed a strikingly high prevalence of SD among female diabetic patients, and the severity of SD was marked by high sexual distress. A significant association was observed between older age, higher education, longer diabetes duration, hypertension, complex treatment regimens and the severity of SD. Poor sexual functioning can be distressing for patients. These results emphasize the urgent need for comprehensive diabetes management that includes routine assessment of sexual health, as SD can be distressing for patients. Therefore, healthcare providers, especially nurses who are usually at the front lines, should prioritize early identification, provide appropriate counselling, and develop tailored interventions to address SD, and ultimately improve the quality of life of female patients with T2DM.
Implications of Findings
The results from this study have far-reaching implications for nursing practice, education, administration, and research, highlighting an urgent need to address the often-overlooked issue of sexual health among female patients with T2DM.
Implications for Nursing Practice
The present study showed a high prevalence of SD among female patients with T2DM, with arousal and orgasm being the most affected domains. These results emphasize the significance of making sexual health assessments a routine component of diabetes care. Nurses must be prepared to discuss sexual health openly, creating a safe and respectful environment for patients to convey their concerns. Understanding the significant connection between age and the severity of SD will also help nurses deliver age-appropriate support, ensuring that older women who are at higher risk obtain the care they need. Practical strategies include patient education, early identification of sexual health issues, and appropriate referrals to specialists.
Implications for Nursing Education
Given the high burden of SD identified in this study, there is an urgent need to incorporate sexual health education into nursing curricula. Nursing students should be trained to promptly recognize, assess, and manage sexual health situations, particularly among patients with chronic conditions like DM. This education should cover not just the biological aspects of SD but also its psychological and emotional dimensions. Simulation-based learning can be an effective method to build students’ confidence in discussing sensitive matters, while educators should model patient-centred, non-judgmental communication. Equipping prospective nurses to manage sexual health holistically will guarantee they provide compassionate, comprehensive care.
Implications for Nursing Administration
For nursing administrators, these findings highlight the essence of creating a supportive environment where sexual health is recognized as an integral element of diabetes care. Policies should mandate routine sexual health examinations for patients with DM, with clear guidelines on how and when these examinations should be performed. Administrators must ensure that nurses receive continuous developmental programs/training, have access to essential tools, and are supported in maintaining patient privacy during sexual health conversations.
Implications for Nursing Research
This study has revealed a vital aperture in the understanding of SD among women with T2DM, underscoring an area ripe for further investigation. Future studies should investigate the factors that contribute to SD in this population, including the effect of blood sugar control and psychological well-being. Research should also focus on designing and testing targeted interventions that can effectively decrease SD and distress. For instance, longitudinal studies can shed light on the long-term impacts of diabetes on sexual health. Also, qualitative research can provide a deeper understanding of the lived experiences of affected women, ensuring that future interventions are both evidence-based and patient-centred.
Footnotes
Author Contributions
ACCC, BCP, AAQ, AET and OOF contributed equally to this work. ACCC & BCP conceptualized and designed the review, led the literature search and data collection, drafted the initial manuscript, and coordinated revisions and final approval. AAQ and AET performed the data extraction, manuscript structuring, and critical revision. OOF review and edited the document. All authors reviewed and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Administrative permission from the Babcock University Research Health Ethical Committee (BURHEC) (BUHREC684/24).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written and verbal informed consent was obtained from all the participants.