
Abstract
Procreation is increasingly perceived as an essential expectation of marriage and is often seen as a symbol of social status and acceptance. The global prevalence of infertility has been estimated as about 17.5%. The prevalence of psychological distress associated with infertility is about 25%–60%. Assisted reproductive technology (ART) also has a significant impact on the overall quality of life, sexual life, and marital harmony. This study qualitatively assessed the sexual and marital satisfaction among couples opting for ARTs. The study was conducted in couples with primary infertility who were taking ART. In-depth interviews were conducted with 12 couples with a preset interview guide structured in simple language. The interview was voice-recorded, transcribed verbatim, and analyzed using a manual content analysis method. In the analysis, six major themes emerged: Psychological impact of infertility, marital dynamics, intimacy and sexual satisfaction, coping strategies, support systems, and perceptions of ART. The couples experienced mental stress secondary to self-perceived stigma and role expectations. The involvement of family and society had been more supportive and less detrimental. Couples demonstrated adaptive coping, strong spousal support, and openness to treatment despite financial burdens. There was a significant impact on the sexual functioning of the couples secondary to treatment for infertility; however, there was adequate emotional fulfillment. Addressing both partners’ mental health and sexual well-being may improve treatment outcomes and quality of life, while promoting a more compassionate societal outlook on infertility and ART.
Background
Procreation is increasingly perceived as an essential expectation of marriage and is often seen as a symbol of social status and acceptance. This has moved from a personal perspective to a social concern. Eventually, a failure to procreate has a greater psychological impact on the couple and their family. By definition, infertility is an inability to achieve a clinical pregnancy after more than one year of regular and unprotected sex. 1 The global prevalence of infertility has been estimated as about 17.5%. 2 The prevalence of psychological distress associated with infertility is about 25%–60%. 3 To overcome the rising burden of infertility, assisted reproductive technologies (ARTs) have been developed and utilized by a wide population.
Psychological well-being of the couples is essential for success with ART. However, ART may influence or be influenced by psychological stressors. Couples undergoing ART have reported a higher prevalence of psychological disorders such as depression, anxiety, somatic symptom disorders, and delusions. 4 ART also has a significant impact on the overall quality of life, sexual life, and marital harmony. Various factors such as age, gender, duration of marriage, economic status, education, cultural beliefs, and family dynamics may predispose patients adopting ART to psychological distress. 5
Most studies on sexual satisfaction and knowledge have been conducted using a cross-sectional design. The other associated factors, such as self-perception of sexuality, support systems, emotional satisfaction of the couple, understanding of physical and emotional components of procreation, and social influences, are less concentrated. A qualitative approach will be a better design to explore these aspects associated with sexual functioning, satisfaction, and fertility. However, the main challenge is to break the psychological barriers to acknowledging and disclosing the issues concerning sexuality. Hence, this study will provide a deeper understanding of this topic.
Aims and Objectives
The study aimed to qualitatively explore the sexual and marital satisfaction among couples opting for ARTs. We also attempted to understand the difficulties faced by couples due to infertility and the coping mechanisms adopted by them.
Methodology
Study Area and Setting
This was a hospital-based qualitative study conducted in the ART clinic at a tertiary care hospital. All the couples availing ART for primary infertility were evaluated, and those who fulfilled the inclusion and exclusion criteria and consented to participate were included in the study. Those couples who have stayed away from each other for most of the time during the past year due to reasons other than infertility were excluded from the study. The ethical approval for the study was obtained from the institutional ethics committee.
Study Design and Sampling
A qualitative study design with a phenomenological approach was adopted. Purposive sampling was done. The primary investigator, who has training in qualitative research, conducted in-depth interviews. There is no fixed sample size for a qualitative study. We approached 14 couples, and two couples did not give consent for the interview. We reached data saturation by the 12th interview, after which no new information was found.
Data Collection
Semi-structured proforma: The sociodemographic details were collected from both husband and wife using a semi-structured proforma.
Interview guide: In-depth interviews were conducted with a preset interview guide. The interview guide covered areas of general sexual knowledge, marital relationship, sexual relationship, attitude toward infertility and ART opted, understanding of the relationship between sexual activity and fertility, and change in sexual and marital health after infertility treatment.
The questionnaire was drafted with open-ended questions. It was evaluated for effective coverage of the research question with two pilot interviews. All the interviews were conducted by the primary investigator, separately for the husband and the wife, in a quiet room, ensuring privacy. Informed consent was obtained at the beginning of the interview for participation and recording of the interview. The initial phase of the interview was concentrated on rapport building. Later, the interview was conducted according to the interview guide, and at the end, a comprehensive summary of the interview, identifying areas of concern, was discussed with the couple. The interview was concluded with clarifications of participants’ queries. The total time taken for the interview was about 50–60 minutes for one person. The entire interview was voice-recorded and transcribed verbatim with notes on the non-verbal reactions of the participants.
Rigor of the Methodology
The trustworthiness of the study was strengthened based on the criteria by Guba and Lincoln. 6 The internal validity that marks the study’s credibility was ensured by selecting a highly informative purposive sample and establishing rapport before the interview. The interview was transcribed on the same day as the interview. The external validity was examined by coding the interview transcript by two investigators independently, checked by a third researcher, and a consensus was reached for the correctness of the code. The confirmability was ensured by providing the interview transcript codes to the couples at the end of the interview, and member-checking was done to know if the codes reflected their experiences. The reliability was enhanced by structuring the interview with a simple-worded interview guide in the local language. We have used the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines for reporting the study findings.
Data Analysis
The text data collected was analyzed using the manual content analysis method. 7 The transcripts were classified into codes, which were then grouped into categories. The categories were then sorted into broad themes based on the research questions.
Results
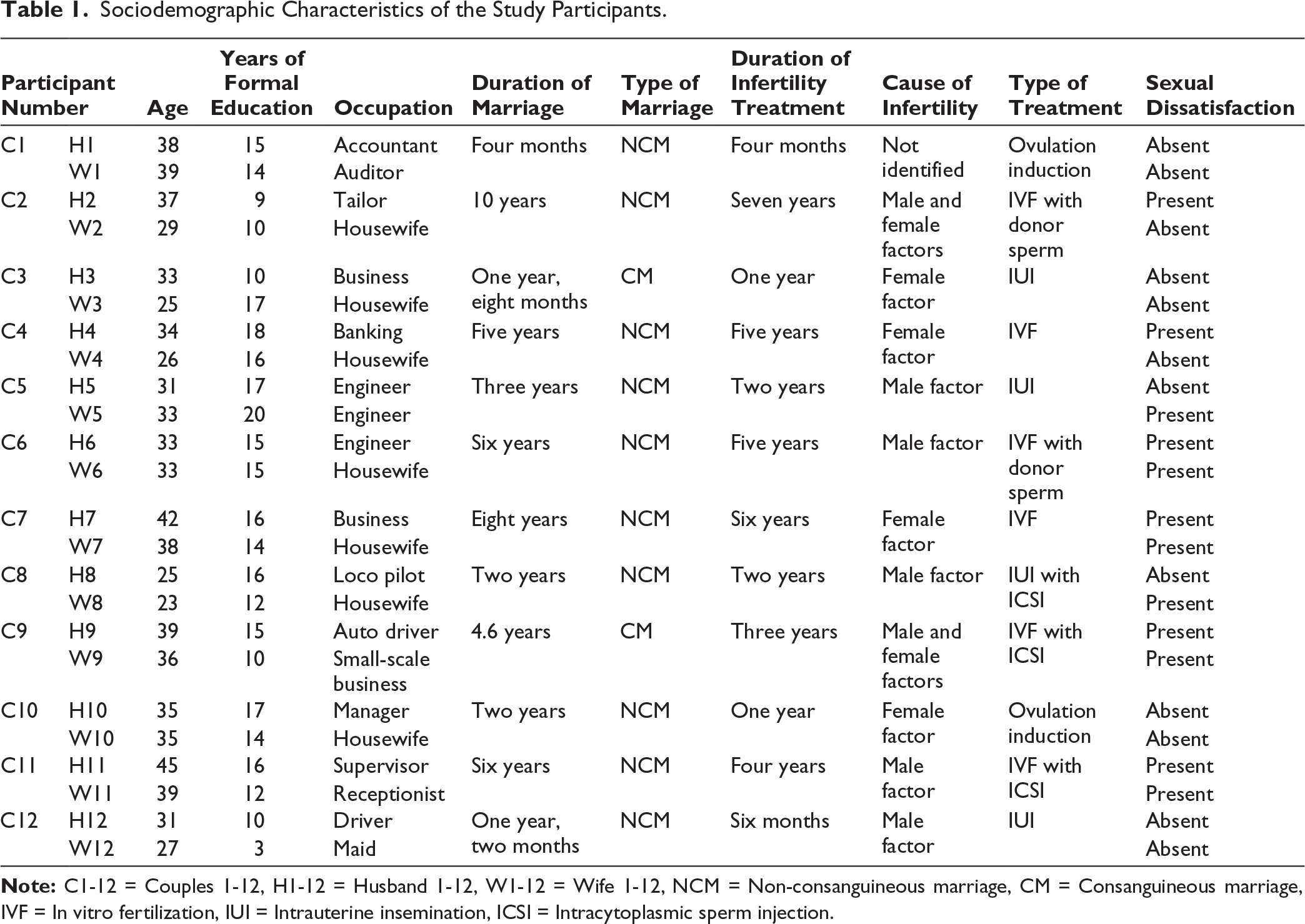
A total of 12 couples with primary infertility opting for ART were interviewed. The average age of the husbands was 35.17 (+5.27) years and that of the wives was 32 (+5.77) years. The minimum age of the husband and wife was 25 and 23 years, respectively. The minimum duration of marriage was four months, and the maximum duration was 10 years. The duration of infertility treatment spanned 3.5 (+2.26) years. The average duration of marriage after which infertility treatment was sought was 1 (+0.93) year.
Among the 12 couples, the reason for infertility was male factor in five couples, female factor in four couples, and combined in two couples. The reason was unidentified in one couple.
Out of the 12 couples, two couples underwent ovulation induction, four couples had intrauterine insemination (IUI), and five underwent in vitro fertilization (IVF). Two couples used donor sperm for the procedure (Table 1).
Sociodemographic Characteristics of the Study Participants.
Psychological Problems Faced by the Female Partners
All of them had expressed psychological disturbances such as insomnia and low mood at some point during the treatment. Three participants had death wishes. Two participants had weight loss, but six participants had weight gain.
Psychological Problems Faced by the Male Partners
All participants experienced low mood, irritability, and decreased concentration at work at some point during the treatment. Seven participants reported low self-esteem.
The data obtained from the interview are grouped into six main themes.
Themes
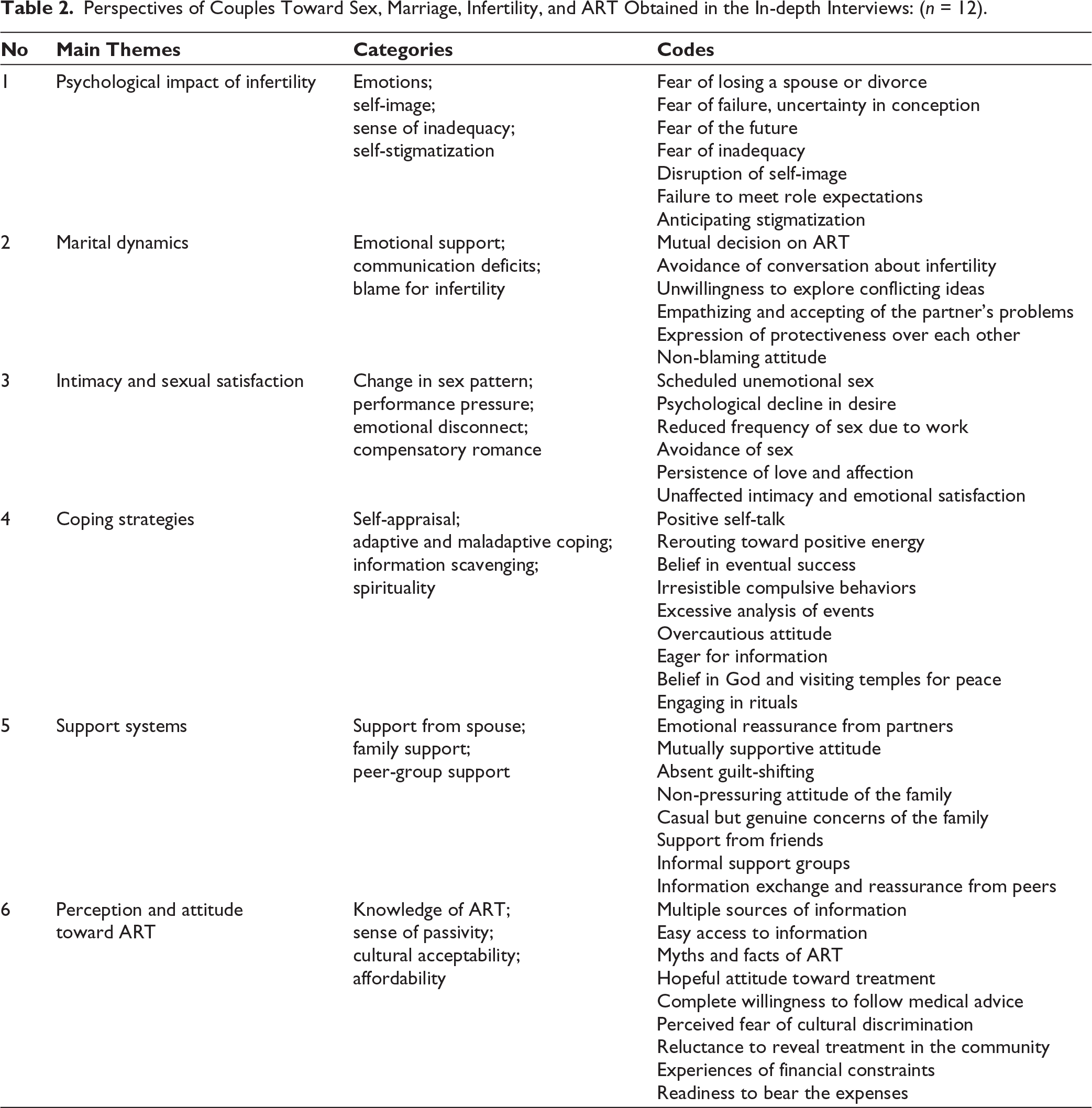
The content analysis of the interview rendered 1,016 codes, which were categorized into 25 categories. The categories were then grouped under six themes: (a) Psychological impact of infertility, (b) marital dynamics, (c) intimacy and sexual satisfaction, (d) coping strategies, (e) support system, and (f) perception and attitude toward ART (Table 2).
Perspectives of Couples Toward Sex, Marriage, Infertility, and ART Obtained in the In-depth Interviews: (n = 12).
Psychological Impact of Infertility
The main emotional component of this theme is fear. The participants experienced fear of losing their spouse, fear of loss of identity, and fear of losing importance in society. One of the female participants (aged 25) said, “My husband’s family is quite orthodox. My mother-in-law might get my husband married to another woman if I do not conceive at the earliest.” However, no family members verbally expressed such thoughts. This also brings out the sense of responsibility to keep up the family tradition. There was high anticipation reported by both male and female partners. A 38-year-old male participant, married four months back, said, “I got married late, I do not want to waste time. My friends who got married before me are going through hardship because of childlessness.” A 26-year-old female participant tearfully said, “I have huge expectations every month. But when I get my menses, I become very frustrated.”
A few participants expressed concerns over self-image. One 33-year-old female participant stated, “Having a child gives us dignity in society.” Another participant (a 35-year-old female) said, “My husband is in a high position; everyone will talk behind him if we do not have a child.” Most of the female participants expressed feelings of inadequacy. A 33-year-old woman graduate said, “Being childless was kind of defective. I feel abnormal when I go out to social gatherings.” Fear of the future was reported as being alone without any support in their old age. A male, 42 years old, claimed, “I am worried that I will not have an heir to light my funeral pyre.”
Self-stigmatization was mostly seen in women. A 29-year-old female participant claimed, “I avoid performing rituals in family functions, and sometimes I avoid playing with small children because I am scared that someone may say something offensive.” A 36-year-old female participant said, “I stopped talking to my friends who have children or have gotten pregnant recently. The main reason is I am scared that they think I will cast an evil eye.”
Marital Dynamics
Marital dynamics reflected more positive concepts. The couples expressed a high degree of understanding, especially in terms of fertility. Most of the couples claimed that the decision for ART was taken unanimously. A 23-year-old wife stated, “My husband is very supportive. No one in the family will ask me about pregnancy because they are scared of my husband. He will get very angry if anyone hurts me.” A 39-year-old wife, who studied up to the 12th standard, said, “This (low sperm count) is something happening inside the body without our control. I cannot blame him (husband) for that.” When a wife (aged 27) was asked about less frequent sexual intercourse, she preferred to support her husband, saying, “My husband is working hard. He comes home late and tired. That is why we do not have sex frequently.”
However, communication deficits have been noticed to a considerable extent. A 26-year-old female participant stated, “I avoid talking about pregnancy and infertility to my husband as I am scared it will end up in arguments over who is the one with a problem.”
Intimacy and Sexual Satisfaction
There was a significant change in the pattern of sexual activities in all the couples. One of the female partners (aged 38) claimed, “Before infertility treatment, we had sex whenever we wanted, but now it is all scheduled by the doctor, like homework.” The male partners felt a performance pressure that had a negative effect on their sexual well-being. A 25-year-old male graduate recollected, “Last month, the doctor had asked us to have sex on a particular date, but I had to go to Bangalore for important office work on those days. I had hurried back home without finishing my work, but after the scan, they said I had to wait two more days.” Following such a timetable for sex makes the act less emotionally enhanced, and eventually, an emotional disconnect is reported by both partners. Over a period of time, there was avoidance of sex, mostly by the male counterpart. One of the husbands (aged 45) stated, “I sometimes feel less interested in sex when compared to the beginning.” One of the wives claimed, “We have sex less frequently nowadays; my husband finds some reason every time to avoid sex.” However, they report reduced desire, and males had difficulty in maintaining an erection because of frequent sexual activity for conception. Even if their sexual activity was less frequent or less satisfying, most of the couples enjoyed a romantic relationship. They spent adequate time on non-sexual intimate activities such as hugging, kissing, and cuddling. A 34-year-old female participant said, “We always sleep hugging each other even if we do not have sex.” Another 28-year-old male participant said, “I express my love by kissing and hugging, and it makes her feel good.” They had emotional fulfillment in the marital relationship.
Coping Strategies
Self-appraisal was a coping strategy followed by many of the couples. A 28-year-old woman said, “I will say to myself every day that I am a good person and good things are bound to happen to me. It gives a positive energy.” A 34-year-old male partner of the couple who had three failed IUIs said, “We are doing everything in our control, and we reassure ourselves that we will succeed soon.” There were a few maladaptive coping methods reported by both male and female partners. A 31-year-old male who has a low sperm count stated, “I tend to smoke excessively when I get frustrated. I am not able to cut down, even though I understand smoking will further reduce the count.” A 29-year-old woman said, “I frequently order food online and eat it as it makes me feel better. My doctors insist I lose weight for a better outcome. If not, I will do online shopping.” A few productive coping methods were also reported, which include learning new skills such as embroidery, adopting pets, cleaning the house, and growing plants, among others.
Almost all the couples had “information scavenging” in the early treatment periods or every time there was a treatment failure. They tried to get information from neighbors, friends, relatives, and multiple doctors. They spent too much time browsing the internet for fertility tips. A 42-year-old male participant stated, “I had searched so much about infertility that all my media websites auto-suggest only fertility-related videos now.” There was a couple who had visited nine doctors for reassurance regarding fertility treatment.
Spirituality plays a major role in psychological well-being in Indian society. Most of the couples were staunch believers in spirituality. It serves as a cultural support system. A 36-year-old female participant claimed, “Whenever my relatives visit me, they will suggest many temples that are special for praying for pregnancy.” A 45-year-old male participant said, “We go to temples whenever we are upset about not having a child; it gives us peace of mind.” On the other hand, superstitions also had a significant interplay. A 35-year-old female participant claimed, “We have spent about one lakh to do rituals suggested by astrologers. Sometimes, my neighbors take me to samiyars who ask me to do weird things.”
Support Systems
The major support for couples experiencing psychological distress due to infertility was their spouse. The statement given by one of the wives was, “Whenever anyone asks me why I did not conceive, my husband always says that the problem can be with any one of us. He never let me down.” One 33-year-old said, “I was scared that she would be upset about my problem (azoospermia), but she was very understanding.” Some families were also supportive of the couple. A 36-year-old male participant said, “My mother usually says, just spend time with each other and enjoy. Do not worry about having a child. Everything will happen when it has to happen.” A 29-year-old wife said, “Everyone (family and friends) said I am young and can wait before going for treatment.”
Another interesting source of support was peers who were taking treatment in the same hospital. They formed a “self-help” group and have regular discussions about the treatment progress. A 25-year-old female participant claimed, “When my first IUI failed, all my friends kept calling and consoling me.” There was another female participant who said, “Since we have friends undergoing various types of infertility treatment, we share experiences and support each other.”
Perception and Attitude Toward ART
The knowledge of ART was usually gained from friends who had undergone it previously. The next common source of information was hospital advertisements. After commencing the treatment, the couples, especially the female partners, felt passive. A 38-year-old female participant on treatment for six years said, “I feel less responsible now. I come when I have an appointment and feel like all the work is done by someone else.” However, this passivity had a positive effect on the women, as they felt less burdened and this thereby reduced their stress. They had reassurance that they were being taken care of by experts.
Ethical concerns were not a problem for most of the couples. One couple undergoing IVF with donor sperm stated, “As long as we get a healthy child, I do not have any problem.” However, one female claimed, “Some people say some others’ sperm will be used for better results without our knowledge by the hospital.” This also reflected the inadequacy of the knowledge of the procedure.
Cultural acceptability is still a fear among couples opting for ART. A 35-year-old male participant claimed, “One of my relatives had a child using IVF more than 10 years ago, but still, I hear people point their child out as a test-tube child.” They also expressed fear of being seen differently by others, due to which they were reluctant to disclose their treatment to anyone.
Affordability for the treatment was reported as a deterrent for infertility treatment. Although the participants expressed readiness to spend on the treatment, their inability to continue the treatment without a break was due to financial constraints. A 26-year-old female participant, a graduate, claimed, “When starting infertility treatment, I quit my job to avoid strain. So, we are facing financial difficulties to cover the treatment expenses.” Another 39-year-old male partner of a couple taking the second cycle of IVF claimed, “I had to take a loan for this cycle of IVF. There was a delay in the treatment process because it took a while for the loan approval.”
Discussion
Sexuality and fertility are almost always read together by most married people. Fertility has been considered a social and familial concern rather than a personal factor. 8 The impact of infertility extends to various domains of life, including the general quality of life, marital harmony, and overall emotional well-being of the person.9–11 Though childbearing had similar psychological effects across various cultures and countries, developing countries had greater concerns about infertility. 12
Factors such as socio-economic status, spouse’s occupations, duration of married life, period of infertility, cause of infertility, and the patterns of sexual intercourse have a significant association with sexual satisfaction. 13 We found that the pattern of sexual intercourse had an impact on the psychological well-being, but other factors such as socio-economic status, occupation, and duration of marriage did not have any obvious effect.
Infertility impacts the perceived social status of women. This causes a significant effect on the psychological health of women with infertility. 14 This was reflected in our study. The stigma perceived was predominantly self-implicated, secondary to anticipated discrimination by the couples.
About 40% of infertility is due to male factor, 40% due to female factor, and only 20% is due to combined factors. 15 In our study, male factors were associated in five out of 12 couples interviewed. Whereas four couples had isolated female factor, and two couples had combined male and female factors. Lack of desire was reported by four male participants, compared to two female participants. It is worth noting that those couples with male factor expressed a higher degree of sexual dissatisfaction.
Though infertility treatment, such as ART, was supposed to be the answer for the problems of infertility, many studies have found that undergoing ART can itself cause psychological distress. 16 This paradoxical effect can be attributed to the ethical issues, outcome uncertainty, financial burden, and impact on self-esteem associated with infertility treatment.17,18 Financial constraints were reported in our study, but the couples were ready to bear the burden of the expenses for the ultimate gift of a child.
Norten et al., in a retrospective study, reported that women undergoing infertility treatment had less sexual desire and satisfaction. They also reported difficulty in attaining orgasms and had an overall negative emotional reaction to sex. They studied 89 women and 27 men, but none of the findings were significant in males. 4 Our study found that as the duration of infertility treatment increased, sexual desire and satisfaction reduced.
Masoumi et al. compared sexual satisfaction between fertile and infertile couples. They conducted a cross-sectional analysis on 270 couples. 5 We did not have any comparative data. However, we found that the treatment technique adopted and the duration of treatment had an effect on sexual satisfaction.
Taebi et al. conducted a qualitative study on the stigma associated with infertility. They interviewed 17 couples with primary infertility. They identified negative attitudes from the family members, such as humiliation and sarcasm. 19 However, this study found that the family members were supportive of most of the patients. This can be considered a sign of a changing perspective of society.
Strengths
The qualitative study design is a huge strength of this study. This design allows the participants to elaborate on sensitive topics and eventually facilitates identifying core problems. This study focuses on the mental aspects of the couple as a dyad, which has not been done in the past. The studies conducted on fertility are mostly focused on the female population. The study reports the impact of childlessness and its treatment on both men and women separately. This helps in a deeper understanding of family dynamics.
Limitations
One limitation of this study is that there is no comparison of the sexual dissatisfaction of the infertile couple with that of a fertile couple. The identification of factors other than infertility and ART, such as the effect of hormonal therapy, that could have a significant impact on sexual functioning, could have enriched the study. Further, the sexual dysfunction and the psychological distress were not quantified. Finally, elaboration of the study with quantitative analysis can be more informative.
Future Implications
All the patients undergoing infertility treatment experience psychological problems at one point in time, which range from insomnia to severe depression with intense suicidality. Routine screening and supportive psychotherapy have to be incorporated into the treatment protocol at the earliest, along with obstetrical management. The psychological support has to be extended post-procedure, irrespective of the treatment outcome. After all, emotional stability is required for good parenting. Adequate psychoeducation regarding the procedure, the expected complications, expenditure, and evidence-based treatment options must be provided to the couple to reduce anxiety.
Conclusion
The couples who opt for ART experienced mental stress secondary to self-perceived stigma and role expectation. The involvement of family and society had been more supportive and less detrimental. The affordability was a concern for many couples, but that did not stop them from availing the treatment. There was a significant impact on the sexual functioning of the couples secondary to treatment for infertility; however, there was adequate emotional fulfillment in the marriage and romantic perspective. The couples who opted for infertility treatment were mutually supportive and had a strong non-blaming attitude toward each other.
The global burden of infertility is growing, and on the other hand, developing technology has bridged the gap. However, the perception and reaction of couples toward infertility and the newer treatment strategies still need attention. This study has shown a considerable change in the attitude of society and increased readiness of couples to break the barriers to reach for treatment. However, the perception of self, shame, and dissatisfaction with marriage and sex of the couples needs to be addressed. There is more space for discussion in this context.
Footnotes
Clinical Trial Number
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted after obtaining approval from the Institutional Ethical Committee (SMVMCH-EC/56/2025).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed written consent has been obtained from all the participants for the participation and publication of the results
Use of Artificial Intelligence
There was no generative artificial intelligence used in the preparation of this manuscript.