
Abstract
Aim:
This study assessed the various aspects of marital functioning among the spouses of patients with schizophrenia and recurrent depressive disorder (RDD).
Methodology:
Spouses were assessed on Dyadic Adjustment Scale (DAS), Marital Forgiveness Scale, Quality Marriage Index, New Sexual Satisfaction Scale, and Arizona Sexual Experience Questionnaire.
Results:
Compared to the spouses of patients with RDD, spouses of patients with schizophrenia reported poor marital adjustment (in the consensus and satisfaction domains of DAS), lower quality of marriage, and significantly lower sexual satisfaction. Spouses did not differ significantly on account of marital forgiveness and prevalence of sexual dysfunction. Higher age of onset of schizophrenia in the patients was associated with better quality of marriage as assessed by using quality of marriage scale, better consensus, and satisfaction as per the DAS. Higher residual psychopathology and poor socio-occupational functioning in patients with schizophrenia were associated with poor marital adjustment and sexual satisfaction.
Conclusion:
To conclude, the present study depicts that the spouses of patients with schizophrenia have poorer marital adjustment and sexual satisfaction, in comparison to the spouses of patients with RDD.
Introduction
Schizophrenia usually has onset of illness in late teens or early twenties and is frequently associated with residual symptoms along with psychosocial deficits. 1 Due to this, many patients are not able to perform some of the important social roles. 1 One of the impacts of residual symptoms and resultant psychosocial deficits in persons with schizophrenia is low marital rates when compared to those without any mental disorder or those with other psychiatric disorders.2-7 However, some of the studies suggest that 70% of patients with schizophrenia eventually get married. 1 Other studies from India, which have looked at the various psychosocial aspects of patients with schizophrenia and their caregivers,8-10 suggest that the percentage of married patients in the study sample of schizophrenia varies from 30% to 60%.11-13 Studies from other countries, such as Ethiopia, also suggest the marital rate of 70.5% among patients with schizophrenia. 14 A cross-cultural study, which compared patients from India and the USA, reported that patients from the USA were more often males and single; however, no such gender difference emerged from India. 15 Accordingly, it can be concluded that the marital rates of patients with schizophrenia in India are higher than those in some of the developed countries and there is no difference in the marital rates with respect to the gender of the patient in India. High marital rates for patients with schizophrenia, in India, can be also attributed to the prevalent cultural beliefs, according to which marriage is considered as a cure for mental disorders. 16
High marital rates suggest that there is a need to understand the spouse’s perspective. Studies among patients with schizophrenia, which have evaluated spouses, have mostly focused on their role as caregivers. Available data suggest that for about 20% to 30% of the patients with schizophrenia, their spouses are the primary caregivers.9-11,17,18 The studies which have focused on the caregiver burden and relationship suggest a lack of difference in the caregiver burden experienced by parents and spouses. 19 A study from Ranchi specifically assessed the caregiver burden among spouses and reported a moderate level of caregiver burden on the spouses, with no significant difference between male and female spouses. 17 However, other researchers suggest higher perception of burden by female spouses.20,21
In India, over the years there has been a breakdown in the structure of Indian families. 22 Consequently, more and more patients with schizophrenia and other mental disorders live in nuclear family setups in contrast to extended or joint family setups earlier.23,24 Due to this on many occasions spouses are the primary caregivers of patients with schizophrenia. This trend is going to increase over time. However, it is also important to note that a nuclear family setup gives more opportunity for sexual intimacy. This makes it important to understand the marital issues between the patients and the spouses, which can determine the continuation of spouses being in the caregiver role. A limited number of studies have assessed various aspects of marital functioning as perceived by the spouses of patients with schizophrenia. A study using the marital adjustment questionnaire reported that when compared to patients with affective disorders, a significantly higher rate of marital maladjustment is reported by patients with schizophrenia. Compared to patients, spouses reported lower rates of marital maladjustment. 25 However, data on sexual functioning and satisfaction among the caregivers of patients with schizophrenia is lacking. Accordingly, this study aimed to assess the various dimensions of marital and sexual functioning from the perspective of spouses of patients with schizophrenia and contrast the same with the spouses of patients with recurrent depressive disorder (RDD).
Methodology
This study followed a cross-sectional design and was executed at the psychiatry outpatient services of a tertiary care multispecialty teaching hospital. Ethics Committee of the Institute approved the study, and participants were enrolled into the study after seeking written informed consent. This study involved an assessment of marital and sexual functioning of patients with schizophrenia and their spouses. Data of patients have been published earlier. 23 This paper focuses on the marital and sexual functioning as reported by the spouses of patients. Detailed methodology of the study is described in the previous paper and it is briefly discussed here. Interested readers can refer to the previous paper. 23
Purposive random sampling was used to collect the study sample. The study sample comprised of 76 and 58 married patients with schizophrenia and RDD and their spouses, respectively. Patients in both the groups were in clinical remission and were clinically stable, ie, did not require any major changes in the medications in the previous 3 months. The inclusion criteria for spouses were as follows: age more than 18 years, married to the patient for at least 1 year, free from any diagnosed physical illness or psychiatric disorder (with only exception being tobacco dependence), and able to read Hindi and/or English. The residual psychopathology in patients with schizophrenia was evaluated on Positive and Negative Syndrome Scale (PANSS), 26 and patients with RDD were evaluated on Hamilton Depression Rating Scale (HDRS) 27 to record the residual psychopathology. Level of functioning of patients of both the groups was assessed by using the Global Assessment of Functioning scale. 28 Socio-occupational functioning in both the groups was assessed by using the Socio-Occupational Functioning Scale (SOFS). 29 SOFS is a 14-item, brief, and easy-to-administer instrument to assess social functioning. Each item is weighted on a 5-point rating scale (1 to 5), with higher level of impairment indicated by higher scores. It has adequate psychometric properties in terms of reliability and validity. The scale has 3 subscales, ie, adaptive living skills, social appropriateness, and interpersonal skills. 29
RDD was selected as a comparison group, because of the chronic nature of the disorder, which can also influence the marital and sexual functioning of the patients.
Spouses of patients of either group were evaluated on Dyadic Adjustment Scale (DAS), 30 Quality Marriage Index (QMI), 31 and Marital Forgiveness Scale (MFS) 32 for the assessment of marital functioning. Sexual functioning was assessed by using Arizona Sexual Experience Questionnaire (ASEX) 33 and New Sexual Satisfaction Scale (NSSS). 34 These scales were selected to have a comprehensive assessment of various dimensions of marital and sexual functioning.
Dyadic Adjustment Scale (DAS)
This 32-item scale is divided into 4 subscales. The scale has high internal consistency (α = .80) and reliability for various subscales.30,35 The test-retest reliability is not influenced much by the demographic variables (age and educational attainment) and family variables, such as the number of children and duration of relationship. 30 Hindi-translated version was used for the study.
Quality Marriage Index (QMI)
It assesses marital satisfaction based on the 6 items, first 5 of which are rated on a 7-point scale and the final item is graded on a 10-point scale. Higher scores on the scale suggest better marital satisfaction. The scale has high internal consistency (α coefficient ranged from .93 to .96 for husbands and from .94 to .95 for wives). 31
Marital Forgiveness Scale (MFS)
This scale assesses the ability to forgive the partner when they have “wronged” or “hurt” the responder. The scale has 6 items, each rated on a 6-point scale, with higher scores suggesting higher agreement with the statements. Values of Cronbach’s α are high for both husbands and wives (.78 to .81), for both positive and negative dimensions of the scale. 32
Arizona Sexual Experience Questionnaire (ASEX)
The ASEX is a 5-item self-report inventory using a 6-point Likert rating, with each item assessing 1 domain of sexual functioning, ie, drive, arousal, penile erection/vaginal lubrication, ability to reach orgasm, and satisfaction from orgasm. A total score of ≥19 or a score of >5 on any single item or a score of >4 on any 3 items points toward clinical sexual dysfunction. The scale has good psychometric properties. 33 Hindi-translated version of the scale was used.
New Sexual Satisfaction Scale (NSSS)
This scale has 20 items which are categorized into 2 dimensions, ie, the first dimension focusing on self (“ego-centered”) and the second dimension focusing on other (a “partner- and sexual activity-centered” factor). 34 The scale has good construct validity and also has satisfactory reliability.
Statistical Package for Social Sciences (SPSS-14) was employed to analyze the generated data. Frequencies and percentage were determined for the categorical variables, and the mean and standard deviation were generated for the continuous variables. Comparisons of data were done by using unpaired t tests, Mann-Whitney U tests, and chi-square tests. Association between different variables was studied by using Pearson’s correlation analysis.
Results
Sociodemographic and Clinical Profile of Patients With Schizophrenia and RDD
The mean age of patients with schizophrenia and RDD was 40.86 (SD=8.43) and 43.44 (SD=7.69) years, respectively, with no statistical difference between the 2 groups. No statistical difference was noted for the 2 study groups in terms of mean education in years, with mean duration of education being slightly more than 10 years for both the groups. Females comprised 55.3% and 51.7% of patients with schizophrenia and RDD, respectively. More than half of the patients were not on paid employment in either of the groups (schizophrenia: 55.3% and RDD: 69%), from lower-middle or lower socioeconomic status (schizophrenia: 61.8% and RDD: 60.3%), from non-nuclear families (schizophrenia: 53.9% and RDD: 55.2%), Hindu by religion (schizophrenia: 75% and RDD: 62.1%), and from rural background (schizophrenia: 82.9% and RDD: 77.6%). A small proportion of patients were the sole earning family member (schizophrenia: 13.2% and RDD: 19%), and about one-fourth of patients were head of the family in the either group (schizophrenia: 25% and RDD: 25.9%). Patients of both the groups did not differ significantly on any of the demographic variable.
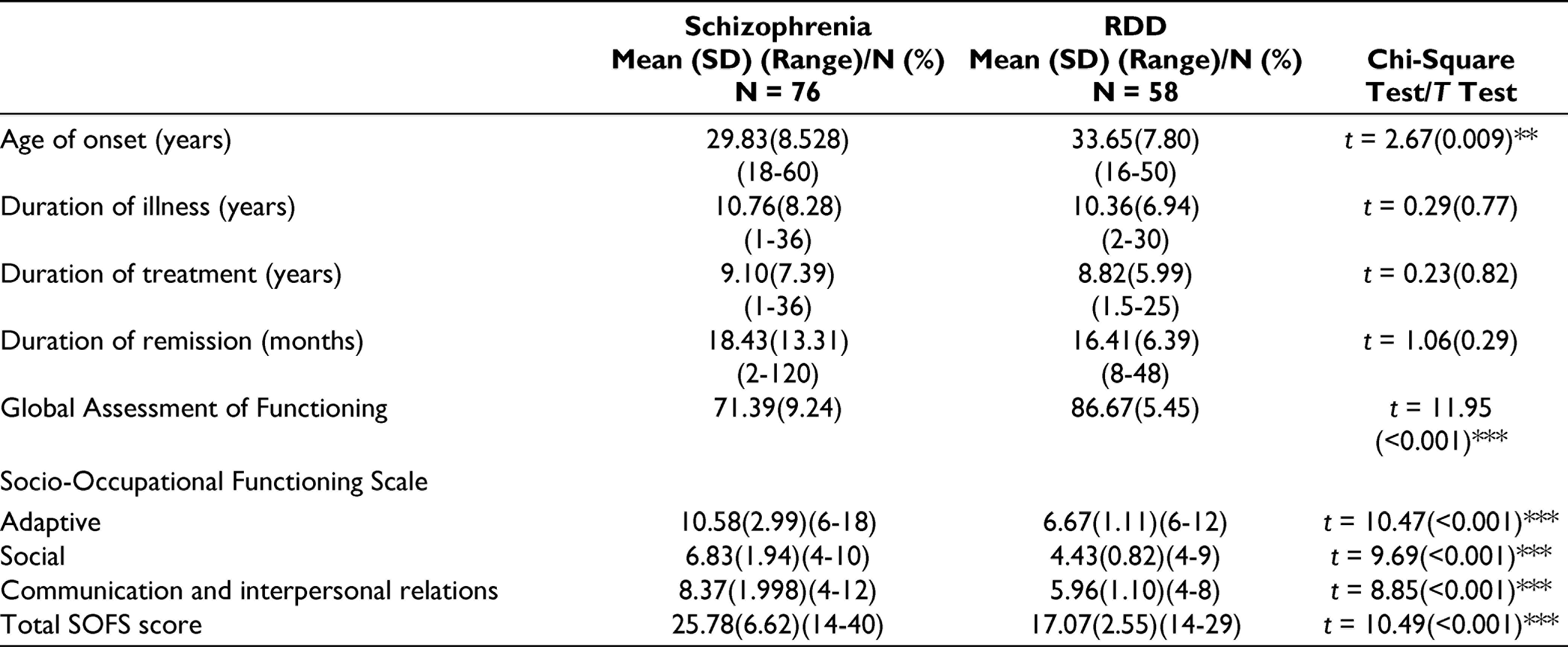
As expected, compared to the RDD group, the age of onset was lower for patients with schizophrenia. However, no significant difference was noted for the duration of illness, duration of treatment, and duration of current remission between the 2 study groups. Total PANSS score for the patients with schizophrenia was 44.66 (SD=10.43), and the mean HDRS score for patients with RDD was 4.15 (SD=1.04). The level of socio-occupational functioning of patients with RDD was better than patients with schizophrenia (Table 1).
Level of General and Social Functioning of Patients With Schizophrenia and Recurrent Depressive Disorder (RDD)
Sociodemographic Profile of Spouses
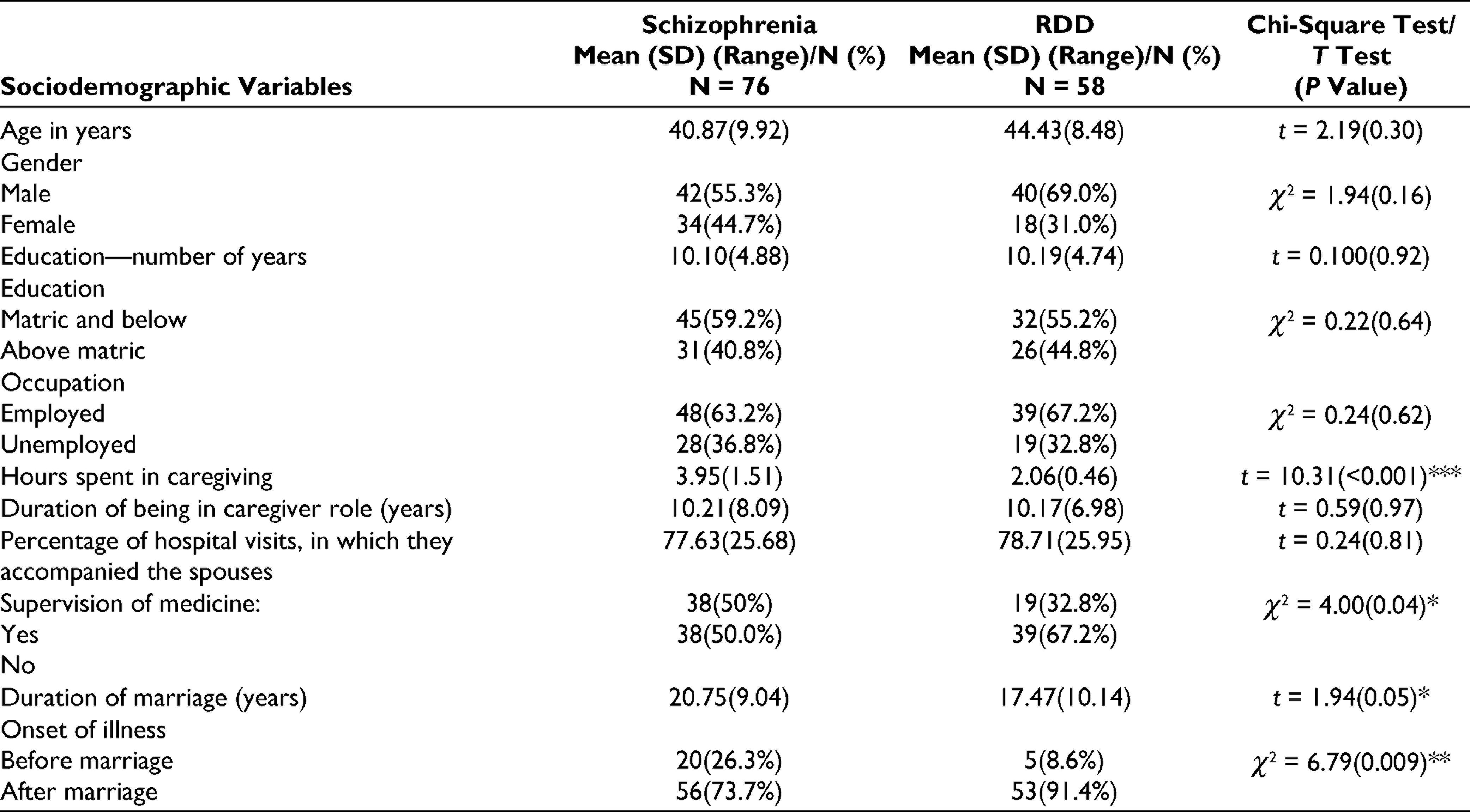
There was no significant difference in the demographic profile of spouses of both the groups, except for the time spent per day in caregiving (Table 2). In both the groups, spouses accompanied the patients for three-fourth of all the hospital visits in the last 3 months. Compared to spouses of patients with RDD, significantly higher proportions of spouses of patients with schizophrenia were supervising the medications. Compared to RDD, the duration of marriage was significantly longer and a higher percentage of the patients had onset of illness before marriage, when one of the partners had schizophrenia.
Sociodemographic Profile of Spouses
Dyadic Adjustment, Marital Forgiveness, and Quality of Marriage
When the duration of marriage was compared, patients with RDD had a significantly shorter duration of marriage and more often had onset of illness after marriage. However, the 2 groups did not differ significantly in terms of the number of children (Table 3).
Details of Marriage, Marital and Sexual functioning as per the Spouses
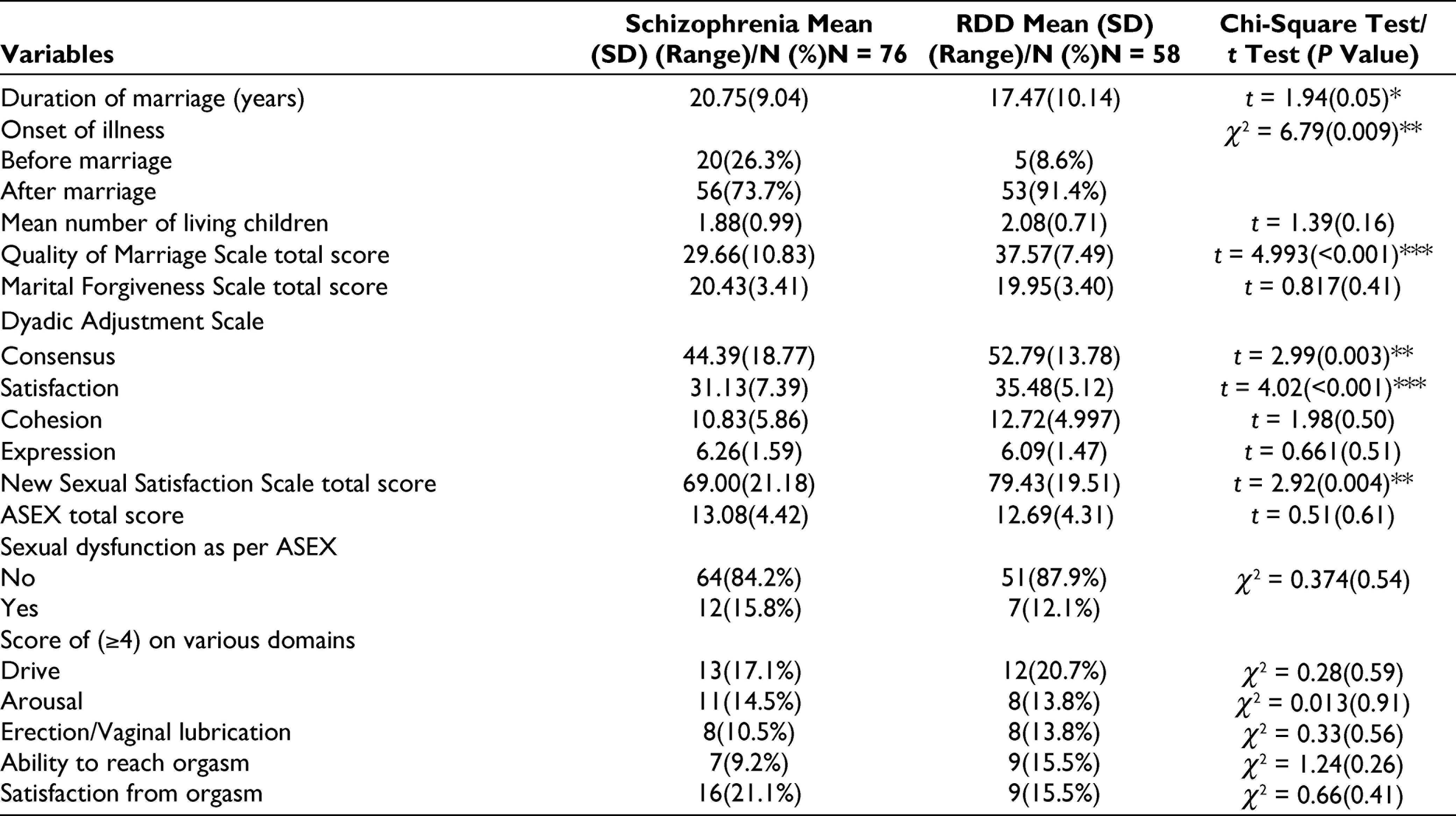
In general, spouses of patients with RDD had better marital functioning in some of the aspects such as consensus and satisfaction. However, no significant difference emerged in terms of sexual dysfunction. Spouses of patients with schizophrenia most commonly reported sexual dysfunction in the form of a lack of satisfaction with orgasm, whereas spouses of patients with RDD most commonly reported sexual dysfunction in the domain of sexual drive, closely followed by difficulty in reaching orgasm and satisfaction with orgasm (Table 3).
Sociodemographic and Clinical Factors Associated With Marital and Sexual Functioning as Rated by the Spouses of Patients With Schizophrenia
Older spouses reported better quality of marriage as assessed by QMI (Pearson’s correlation coefficient = 0.22; P value = .05*) and poorer sexual functioning as assessed by the ASEX score (Pearson’s correlation coefficient = 0.23; P value = .04*). Compared to female spouses, male spouses reported better quality of marriage (t test value = 2.38; P = .02*), better dyadic adjustment in 3 out of 4 domains of DAS, ie, consensus (t test value = 2.01; P = .04*), satisfaction (t test value = 2.75; P = .007**), and cohesion (t test value = 3.32; P = .001***), and better sexual satisfaction as assessed by NSSS (t test value = 2.5; P = .01**). Compared to spouses, who were currently unemployed, spouses who were employed reported better sexual satisfaction as assessed by using NSSS (t test value = 2.02; P = .04*). Compared to spouses from non-nuclear families (ie, joint or multigenerational), spouses from nuclear families had significantly higher marital forgiveness (t test value = 4.06; P < .001***). Compared to spouses from lower-middle/lower socioeconomic status, spouses from upper/upper-middle socioeconomic status reported significantly higher cohesion on DAS (t test value = 2.98; P = .004**). Other demographic variables did not have any significant association with the marital and sexual functioning.
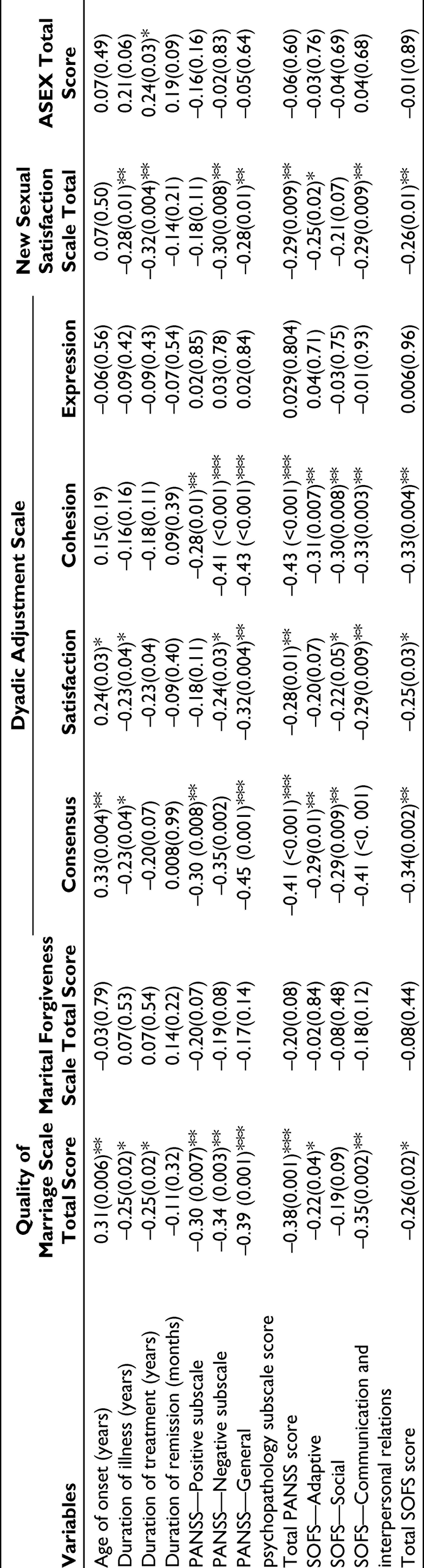
Association of Clinical Variables of Patients With Marital and Sexual Functioning as Perceived by the Spouse of Patients With Schizophrenia
Higher age of onset of schizophrenia in the patients was associated with better quality of marriage as assessed by using QMI, and better marital consensus and satisfaction as per the DAS. Shorter duration of illness was associated with better quality of marriage as assessed by using QMI, better consensus and satisfaction as assessed on DAS, and better sexual satisfaction assessed with NSSS. Shorter duration of treatment was associated with better quality of marriage as assessed by using QMI. In general, higher residual psychopathology and poor socio-occupational functioning were associated with lower marital adjustment and lower level of sexual satisfaction (Table 4).
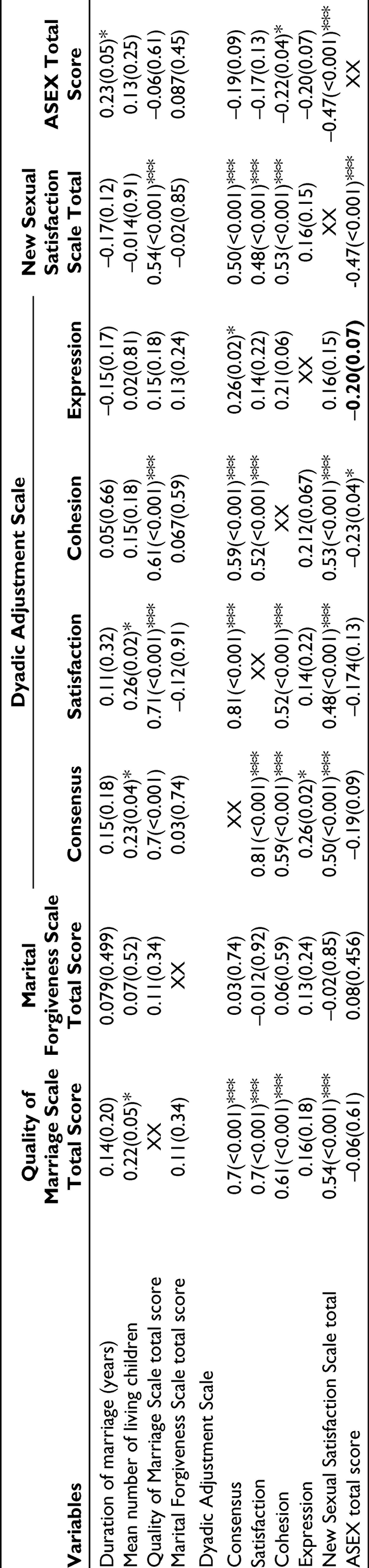
Clinical Correlates (Pearson’s Correlation Coefficient) of Marital and Sexual Functioning in Spouses of Patients With Schizophrenia
Correlates of Marital and Sexual Functioning
When the relation of duration of marriage and number of children with various aspects of marita and sexual functioning was assessed for the schizophrenia group, a higher number of living children was associated with better quality of marriage, better consensus, and satisfaction as per the DAS (Table 5).
Correlates (Pearson’s Correlation Coefficient) of Marital and Sexual Functioning in Spouse of Patients With Schizophrenia
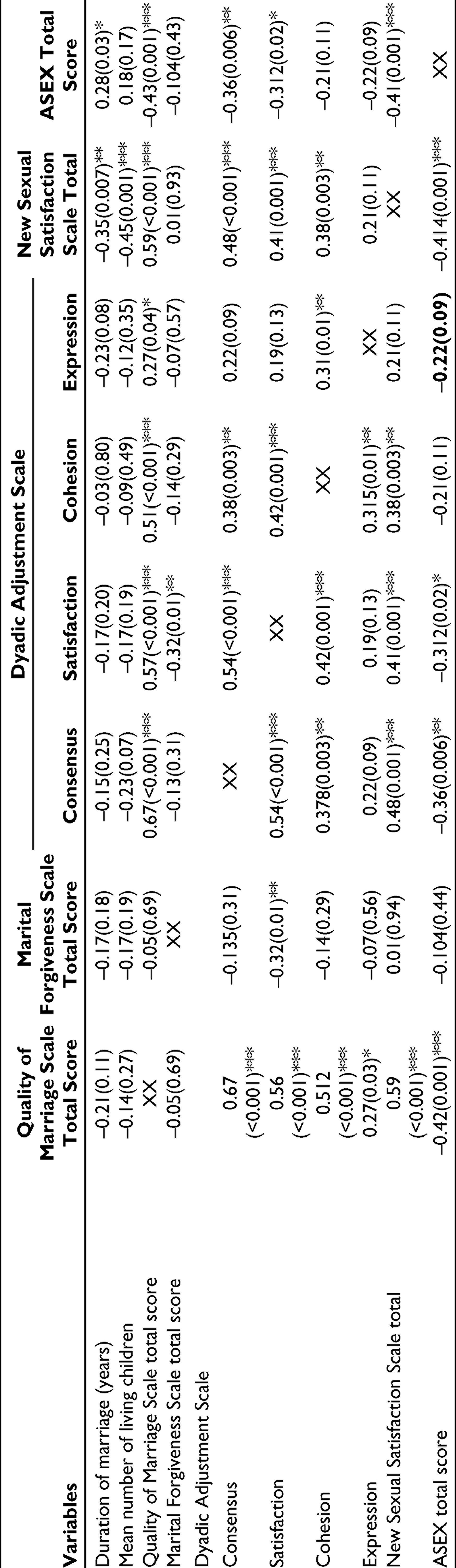
Among the spouses of patients with RDD, age, education, and income of spouses did not correlate significantly with QMI, MFS, DAS, NSSS, and ASEX total score, except that younger spouses reported lower sexual satisfaction as assessed by using NSSS (Pearson’s correlation coefficient = –0.27; P = .04*).
In the RDD group, there was no significant difference on the QMI, MFS, any of the domains of DAS, NSSS, and ASEX score between spouses of patients of either gender, those belonging to nuclear and non-nuclear families (ie, joint or multigenerational), upper/upper-middle socioeconomic status and lower-middle/lower socioeconomic status, and Hindu and non-Hindu religion. Compared to those unemployed, spouses who were employed reported significantly better marital forgiveness (t test value = 2.49; P = .01**), lower marital consensus (t test value = 2.24; P = .03*), and lower marital satisfaction (t test value = 2.19; P = .03*) as per the DAS.
In the RDD group, lower age of onset of illness of patients was associated with higher marital forgiveness by the spouses. Shorter duration of illness and shorter duration of treatment were associated with significantly better quality of marriage as assessed by QMI, better dyadic adjustment as indicated by DAS, and better sexual satisfaction as assessed by NSSS. Longer duration of illness was associated with significantly higher sexual dysfunction as assessed by using ASEX.
Residual psychopathology did not correlate with marital adjustment, sexual satisfaction, and sexual dysfunction as reported by the spouses. However, higher socio-occupational dysfunction of the patients was associated with lower sexual satisfaction among the spouses as assessed by using NSSS (Table 6).
Clinical Correlates (Pearson’s Correlation Coefficient) of Marital and Sexual Functioning in Spouse of Patients With Recurrent Depressive Disorder
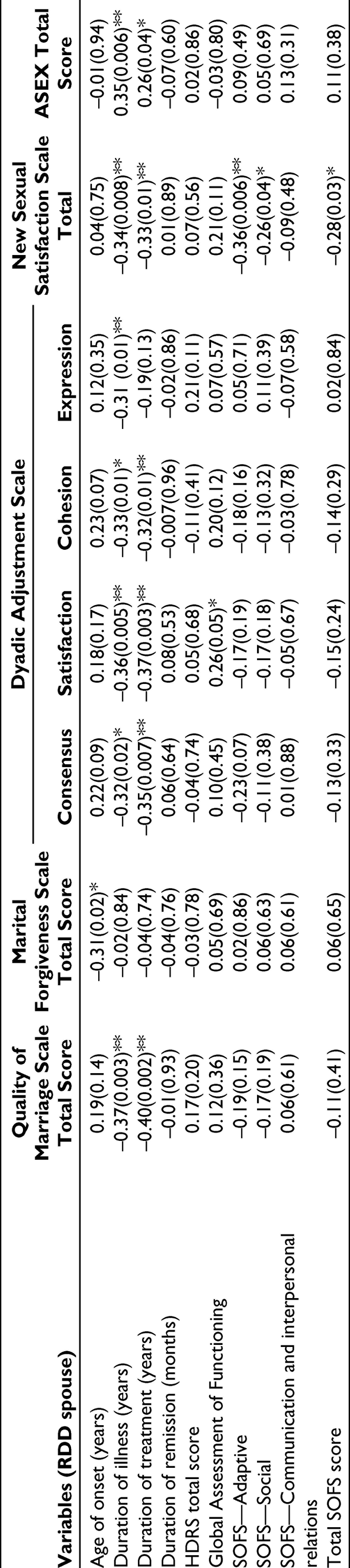
Longer duration of marriage and higher number of living children were associated with lower sexual satisfaction among the spouses as assessed by using NSSS (Table 7).
Association (Pearson’s Correlation Coefficient) of Marriage Related Variables With Marital and Sexual Functioning in Spouse of Patients With Recurrent Depressive Disorder
Relationship of Different Scales Used for Assessment of Marital and Sexual Functioning Among the Spouses
In terms of association of various marital and sexual functioning scales, various domains of DAS correlated positively with each other, QMI, and NSSS score in the schizophrenia group. MFS score did not have any significant association with any of the other scales. Similarly, NSSS score had a positive association with quality of Marriage Scale score and 3 of the 4 domains of DAS. Higher level of sexual dysfunction as assessed by using ASEX was associated with poor cohesion domain of DAS and poor sexual satisfaction as assessed by NSSS (Table 5).
In the RDD group, the domains of DAS correlated positively with quality of marriage scale. Higher marital adjustment as assessed by DAS was associated with better sexual satisfaction as indicated by NSSS. Quality of marriage as assessed by QMI correlated positively with NSSS and negatively with ASEX total score. MFS score correlated negatively with the satisfaction domain of DAS. NSSS score correlated negatively with ASEX total score (Table 7).
Discussion
Spouses of patients with severe mental disorders form an important subgroup of caregivers, who provide care to patients with schizophrenia. The psychosocial impact of caregiving on spouses or caregivers in general has been understood as caregiver burden, 36 experience of caregiving, 37 caregiver distress, 38 stigma, and psychological morbidity.18,39,40
Patients with schizophrenia are known to have emotional and social deficits, 1 which can impact the intimacy with the partner. These deficits also contribute to a higher rate of marital failure in the form of divorce, marital discord, and separation in patients with schizophrenia. 41 It can be hypothesized that emotional, social, and sexual deficits in the patients lead to lot of distress among the spouses, which can then lead to marital disharmony and disruption of caregiving role. Although information is available for the prevalence of sexual dysfunction among the patients with schizophrenia, how this affects their spouses is not understood. Thus, it is important to understand the marital and sexual adjustment between the patients and the spouses. Accordingly, we aimed to evaluate the marital and sexual functioning among spouses of patients with schizophrenia and RDD.
In view of lack of significant difference in the demographic profile between both the groups, it can be said that the difference between the 2 study groups in the marital and sexual functioning observed in the present study cannot be attributed to the demographic variables. The sociodemographic profile of patients with schizophrenia included in our study is similar to previous studies from this center which has focused on clinically stable patients with schizophrenia42-45 and other parts of the country,29,46 suggesting that the study population was representative of the patients with schizophrenia seen in this center and other centers in the country.
The demographic profile of spouses is also similar to the profile of caregivers reported for patients with schizophrenia in previous studies.43,44 Spouses of both the study groups did not differ significantly on the demographic profile, except that spouses of patients with schizophrenia were spending higher amount of time and were more often involved in the supervision of the medications. These findings are in expected lines, considering the fact that the caregiving needs are higher for patients with schizophrenia.
Marital Functioning as per the Spouses of Patients With Schizophrenia and RDD
This study indicates that compared to the spouses of patients with RDD, spouses of patients with schizophrenia have poorer dyadic adjustment (domains of consensus and satisfaction) and quality of marriage. Consensus domain of DAS reflects the level of agreement with the partner, whereas the satisfaction domain reflects the level of satisfaction with the partner. Accordingly, it can be said that compared to spouses of patients with RDD, spouses of patients with schizophrenia have poor marital adjustment. As there are no previous studies which have used similar instruments to assess marital functioning in spouses, findings of the present study cannot be compared with the existing literature. However, based on our findings, it can be concluded that spouses of patients with schizophrenia have poor marital functioning. Clinicians managing patients with schizophrenia, who are married, need to evaluate the marital issues both from the perspective of patients and spouses and address the issues.
In terms of sexual dysfunction among spouses, a small proportion of spouses (12.1% to 15.8%) were found to have sexual dysfunction. This prevalence is toward the lower end of prevalence of sexual dysfunction reported in the general population.47,48 The lower prevalence in the present study could be because of a limitation of the study sample of married subjects. When a comparison was done for the spouses of patients with RDD and schizophrenia, significantly lower sexual satisfaction was reported by the latter group. When the association of different scales was evaluated, it was seen that ASEX and NSS have a good correlation, suggesting that sexual dysfunction influences sexual satisfaction. Accordingly, any effort to reduce the sexual dysfunction among patients can lead to improvement in sexual satisfaction among the spouses.
Relationship of Marital and Sexual Functioning With Other Variables Among Spouses of Patients With Schizophrenia
Duration of marriage was not associated with marital functioning and sexual satisfaction. However, a longer duration of marriage was associated with poor sexual functioning. Higher numbers of children were associated with better dyadic adjustment in the consensus and satisfaction domains. In terms of patient’s variables, it was seen that younger age of onset of schizophrenia, longer duration of illness, longer duration of treatment, higher residual psychopathology, and poorer socio-occupational functioning of patients were associated with one or the other aspects of marital functioning and sexual satisfaction among the spouses of patients with schizophrenia. However, these associations were not seen or were not as robust for the RDD group. As previous studies have not looked at these associations, a finding of the present study requires replication. However, these associations suggest that adequate control of symptoms of patients and better socio-occupational functioning of the patients can influence marital functioning and sexual satisfaction of the spouses. Hence, there is a need to control the symptoms and optimize the functioning of the patients. This can possibly help in stabilizing the marital unit of patients with schizophrenia.
Associations of different scales suggest that there is an overlap in the marital functioning assessed by these scales, and these associations lend concurrent validity for these scales. Marital forgiveness stood out in not having any significant correlation with other aspects of marriage which suggests that forgiveness is more of a personality virtue, which may be beyond the marital relationship only. The association of better quality of marriage and dyadic adjustment with sexual satisfaction suggests that sexual satisfaction goes hand in hand with marital adjustment. Similar associations were also seen in the patient group, as reported in the previous paper from this study. 23 Poor sexual satisfaction and poor dyadic adjustment were associated with higher level of sexual dysfunction. Accordingly, addressing sexual dysfunction among spouses of patients with schizophrenia and RDD can lead to improvement in marital functioning.
The findings of the present study must be interpreted in the light of its limitations. This study was limited to the spouses who were also acting as caregivers for the patients. Hence, the results cannot be generalized to the spouses of other patient populations. A cross-sectional assessment precludes any information about change in marital and sexual functioning over time. Further, the study participants were recruited by purposive sampling, there was a difference in the severity of illness between the 2 groups, and no sample size calculation was done for the study. Additionally, we did not assess the personality characteristics of the spouses, which can also influence the marital and sexual functioning and satisfaction. These limitations need to be addressed by the future studies.
Conclusions
This study suggests that compared to the spouses of patients with RDD, the spouses of patients with schizophrenia have poorer marital adjustment and sexual satisfaction. A higher level of sexual dysfunction possibly results in poor sexual satisfaction and poor marital adjustment. Hence, clinicians should pay due importance to the marital and sexual issues between the couple and address the same. Since marital maladjustment and sexual dissatisfaction correlate with each other, this issue must be kept in mind while selecting the psychotropic medications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.