
Abstract
Background:
Infertility is a significant psychosocial stressor that adversely affects sexual satisfaction, marital quality, and psychological well-being in couples. While standard infertility counseling (SC) addresses individual distress, it often neglects relational and dyadic concerns. This study evaluates the effectiveness of couple-based intervention (CBI) compared to SC in improving sexual, relational, and emotional outcomes in couples with primary infertility.
Methods:
A randomized controlled trial (RCT) was conducted among 60 heterosexual couples with primary infertility at Saveetha Medical College and Hospital. Participants were allocated into two groups: CBI (n = 30) and SC (n = 30). CBI involved six joint sessions incorporating emotionally focused couple therapy (EFT), Cognitive Behavioral Therapy (CBT)-based couple work, sexual communication, and mindfulness. SC involved individual-focused cognitive and supportive counseling. Outcomes were measured at baseline and post-intervention using the Index of Sexual Satisfaction (ISS), Dyadic Adjustment Scale (DAS), and General Health Questionnaire-28 (GHQ-28).
Results:
The CBI group showed statistically significant improvement across all domains: ISS (P = .0001), DAS (P = .0003), and GHQ-28 (P = .0001). The SC group did not show significant improvements in any scale. Urban residence was associated with better intervention outcomes (P = .042), suggesting sociodemographic factors may influence therapy engagement.
Conclusion:
CBI was more effective than SC in improving sexual satisfaction, marital quality, and psychological well-being in infertile couples. Couple-focused approaches should be integrated into infertility treatment, especially for urban, and educated populations.
Keywords
Introduction
Infertility is a significant life stressor with profound psychological and relational consequences. While the medical management of infertility has advanced, its psychosocial dimensions remain underaddressed. Among affected couples, infertility often results in reduced sexual satisfaction, deterioration in marital quality, and a decline in psychological well-being. These challenges are compounded by societal stigma, treatment burdens, and emotional isolation.
Standard infertility counseling (SC) typically focuses on individual coping and medical education. However, emerging evidence highlights the importance of addressing infertility as a dyadic issue, where both partners are affected emotionally and relationally. Couple-based interventions (CBI), incorporating joint therapy sessions, communication training, sex therapy modules, and emotion-focused approaches, have shown promise in enhancing both psychological and relational outcomes. 1
Despite growing research, there is a paucity of randomized controlled trials (RCTs) comparing couple-based models directly with SC in the Indian context. This study aims to fill that gap by evaluating the effects of CBI versus SC on sexual satisfaction, marital adjustment, and psychological well-being in couples experiencing primary infertility.
Methodology
Study Design and Setting
A six-month, parallel-group, RCT was conducted at the Department of Psychiatry in collaboration with the Department of Obstetrics and Gynecology, Saveetha Medical College and Hospital, Chennai.
Participants
A total of 60 heterosexual couples with primary infertility were recruited from the infertility clinic. After screening and consent, couples were randomized into:
Group A: CBI Group B: SC
Inclusion Criteria
Married heterosexual couples diagnosed with primary infertility (>1 year without conception)
Both partners aged 20–45 years
Willingness of both partners to participate in counseling
Adequate literacy to complete questionnaires
Exclusion Criteria
Presence of major psychiatric disorders (e.g., psychosis, substance use)
Severe marital conflict or ongoing domestic violence
One or both partners are already undergoing psychiatric or sex therapy
Current use of psychotropic medications
Randomization and Blinding
Couples were randomized using simple randomization
Allocation concealment was ensured using sealed opaque envelopes
Outcome assessors were blinded to group allocation
Intervention Protocols
Group A: Couple-based Intervention
Six joint sessions over six weeks
Components included:
Emotionally focused couple therapy (EFT)
Cognitive behavioral couple therapy (CBCT)
Sexual communication and intimacy enhancement
Joint mindfulness and stress-reduction exercises
Psychoeducation on infertility.
Group B: Standard Counseling
Six individual sessions (one or both partners may attend)
Focus on:
Coping strategies
Information about infertility treatments
Individual stress and emotional regulation techniques.
Outcome Measures
Assessed at Baseline and Six Weeks Post-intervention
At both baseline and six weeks post-intervention, three domains were assessed. Sexual satisfaction was measured using the Index of Sexual Satisfaction (ISS). Marital quality was evaluated with the Dyadic Adjustment Scale (DAS). Psychological well-being was assessed using the General Health Questionnaire-28 (GHQ-28). 2
For each domain, the best scale and rationale were as follows: The ISS was chosen for its dyadic focus and because it has been validated in infertility research. The DAS was selected for marital quality as it is the most validated and comprehensive measure of marital adjustment. The GHQ-28 was used for psychological well-being due to its clinical sensitivity and its applicability to infertility-related stress.
Standard Infertility Counseling
Model Example: Individual CBT-based Counseling
Format: One-on-one or group sessions, not necessarily including both partners
Focus Areas:
Emotional support for treatment burden, uncertainty, grief Psychoeducation about infertility and treatment procedures Cognitive restructuring of maladaptive thoughts (e.g., hopelessness, guilt) Stress and anxiety management techniques (e.g., relaxation, problem-solving).
Limitations:
Little focus on couple dynamics or shared coping Sexual functioning and relationship strain are often underaddressed May reinforce a patient-centered (not dyadic) model of care.
Couple-based Intervention
Model Example: Emotionally Focused Couple Therapy (EFT) + CBT + Sex Therapy
Format: Joint sessions involving both partners (6–12 sessions, weekly or biweekly)
Components:
EFT: Strengthens emotional bonds; reframes infertility distress as a shared challenge CBT for couples: Identifies negative interaction cycles, encourages collaborative problem-solving
3
Sex therapy modules: Rebuilds intimacy, addresses sexual avoidance, and anxiety related to timed intercourse Communication training: Improves empathy, active listening, and shared meaning-making.
Benefits:
Enhances marital quality and dyadic coping Improves sexual satisfaction by reducing conflict and performance pressure Strengthens psychological well-being via mutual emotional regulation
Evidence: Shown to reduce distress, increase treatment adherence, and enhance relationship satisfaction more effectively than individual therapy.
In terms of focus, SC primarily offers individual emotional support, whereas the CBI addresses dyadic emotional, sexual, and relational healing. Regarding the sexual health component, it is rarely included in SC, while in the couple-based approach, it is treated as a central component. Emotional bonding is mostly not addressed in SC but is actively reinforced through structured exercises in the CBI.
For communication enhancement, SC provides minimal focus, whereas the CBI emphasizes communication using structured tools and feedback. In terms of treatment impact, SC is considered moderately effective, while the couple-based model has been shown to improve both relationship and mental health outcomes. Last, the research backing for SC is limited in the context of infertility, whereas the CBI is supported by RCTs and meta-analyses in both infertility and oncology contexts.
Statistical Analysis
SPSS version 23 used for all analyses
Descriptive statistics for demographic data
Independent t tests and chi-square tests for between-group comparisons
Paired t tests for pre-post changes within each group
Significance threshold: P < .05.
Results
Intervention Outcomes
CBI group (n = 30)
Sexual satisfaction (ISS):
Baseline: 67.9 ± 5.0 Post-intervention: 61.5 ± 4.7 t = 4.25, P = .0001 (significant improvement) Marital quality (DAS):
Baseline: 90.8 ± 6.0 Post-intervention: 97.4 ± 5.8 t = 3.92, P = .0003 (significant improvement) Psychological well-being (GHQ-28):
Baseline: 26.0 ± 4.1 Post-intervention: 19.6 ± 3.9 t = 4.68, P = .0001 (significant improvement)
SC Group (n = 30)
Sexual satisfaction (ISS):
Baseline: 68.2 ± 5.1 Post-intervention: 66.9 ± 5.3 t = 1.12, P = .264 (not significant) Marital quality (DAS):
Baseline: 91.5 ± 6.2 Post-intervention: 92.3 ± 6.1 t = 0.97, P = .336 (not significant) Psychological well-being (GHQ-28):
Baseline: 25.8 ± 4.3 Post-intervention: 24.7 ± 4.5 t = 1.03, P = .308 (not significant).
The findings of this RCT clearly demonstrate that the CBI is significantly more effective than SC in improving outcomes across all three domains assessed: Sexual satisfaction, marital quality, and psychological well-being. Participants in the CBI group showed statistically significant improvements in their post-intervention scores on the ISS, DAS, and GHQ-28 (Table 1), while those in the SC group did not show any significant change (Table 2). 4 This suggests that therapeutic approaches that actively engage both partners, such as EFT and structured communication exercises, are more impactful than traditional individual-focused counseling in the context of infertility.
Couple-based Intervention Results.

Standard Infertility Counseling Results.

Additionally, the demographic analysis revealed that urban residence was significantly associated with better outcomes in the couple-based group (Table 3), possibly due to greater access to health information, stronger health-seeking behavior, or better comprehension of psychological concepts. Although other variables such as age, education, duration of infertility, and employment did not show statistically significant differences, there was a notable trend indicating that higher educational status may enhance the uptake and benefit from CBIs. These findings underscore the importance of integrating relational and systemic approaches in infertility counseling, particularly among motivated and engaged couples.
Baseline Demographic Characteristics and Observations.
Discussion
The findings of this RCT highlight the superior efficacy of CBI over SC in improving sexual satisfaction, marital quality, and psychological well-being among couples experiencing primary infertility. These results underscore the critical role of relationship-focused therapeutic approaches in addressing the multidimensional stressors associated with infertility.
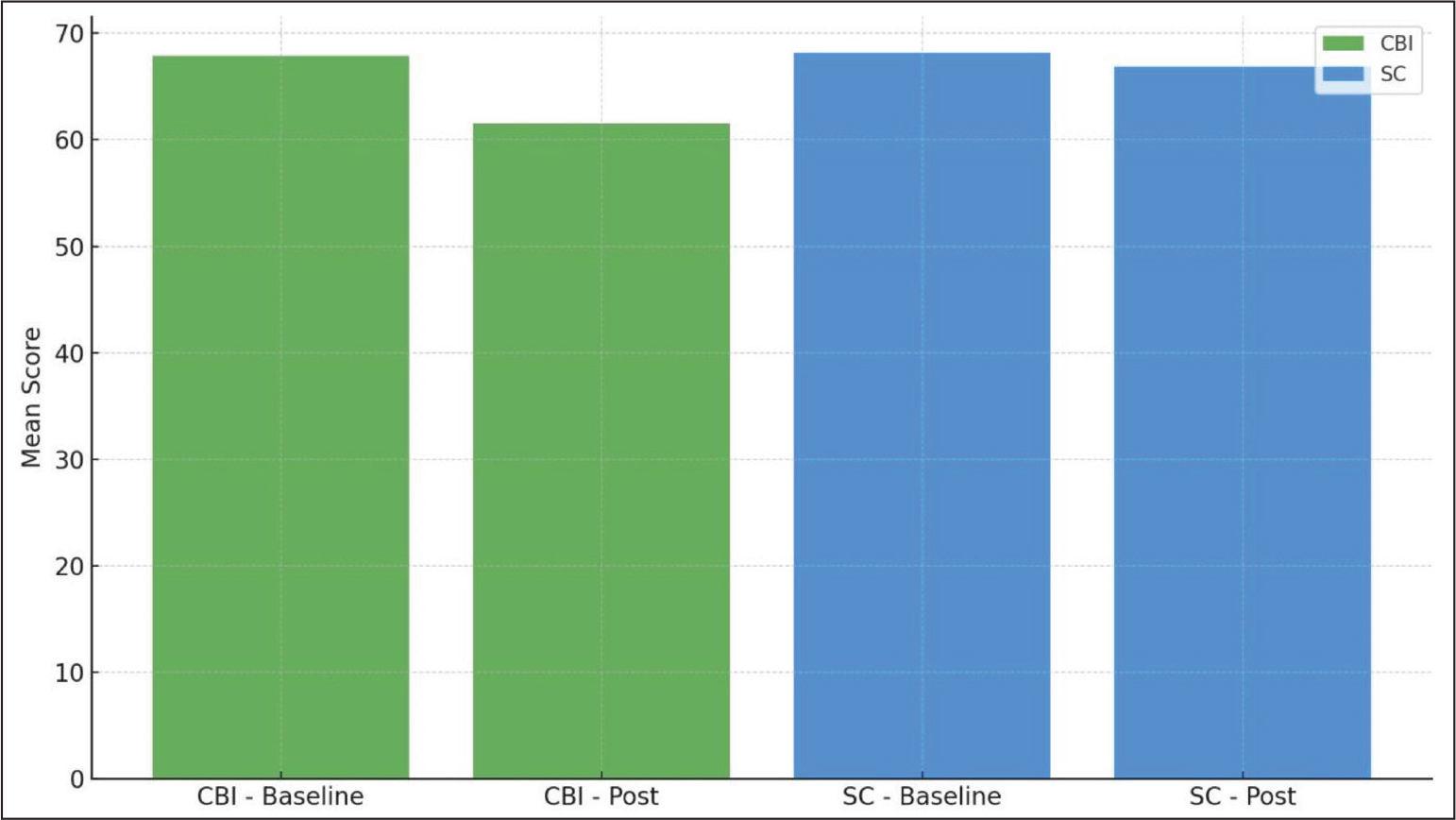
In the present study, the CBI group demonstrated statistically significant improvements across all three domains measured. The improvements in sexual satisfaction, as measured by the ISS, indicate that couple-focused therapy not only reduces sexual avoidance and performance anxiety but also helps partners rebuild emotional and physical intimacy (Figure 1). This finding aligns with studies showing that EFT can effectively address sexual disconnection by restructuring maladaptive emotional patterns and enhancing secure attachment bonds (Yazdani et al). 5
Sexual Satisfaction (ISS): Showing Pre-post Comparison for CBI and SC.
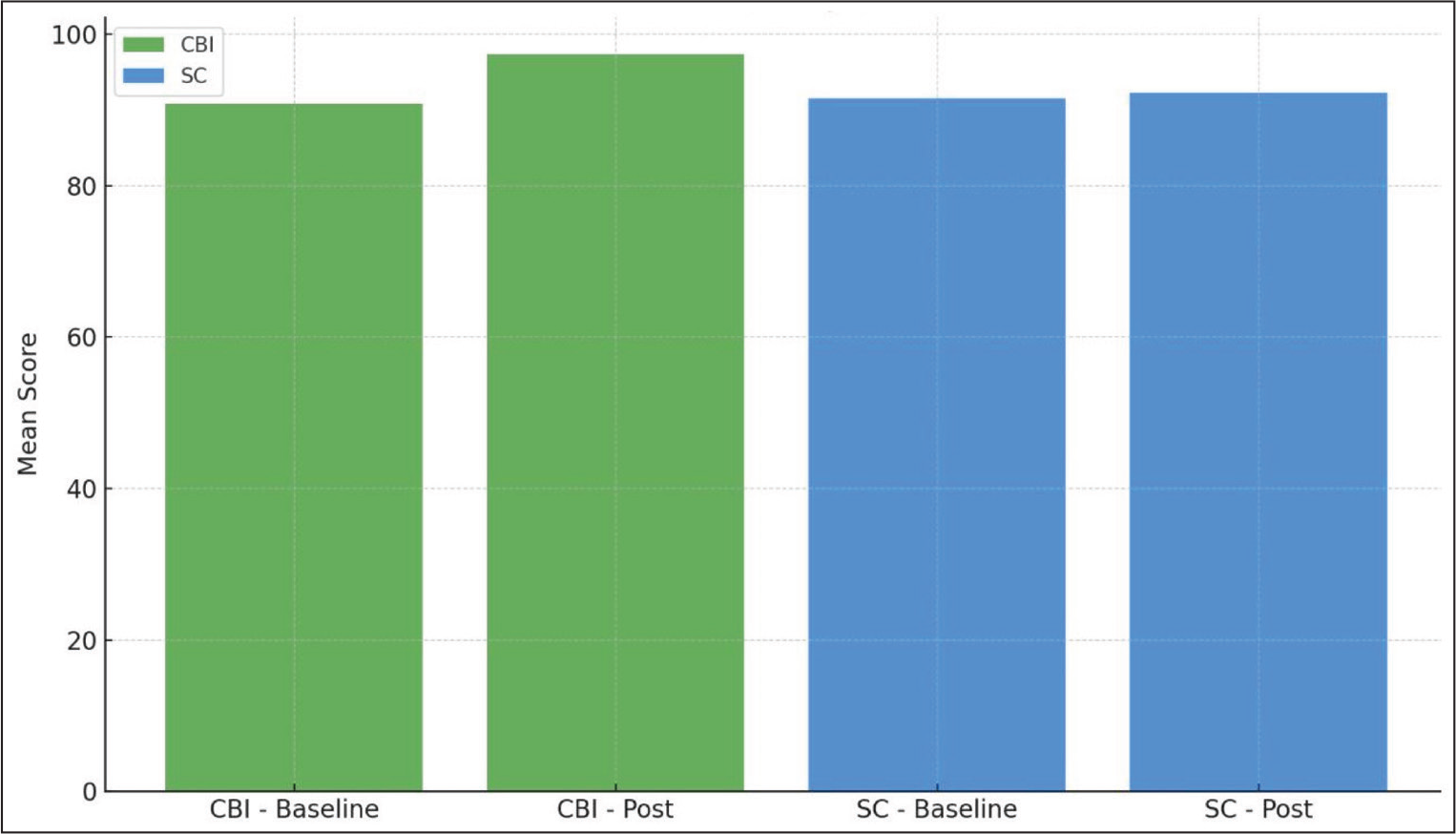
Similarly, the improvement in marital adjustment (DAS scores) (Figure 2), suggests that involving both partners in structured therapeutic sessions fosters open communication, mutual empathy, and collaborative coping. SC, which often targets individual distress, lacks the dyadic tools needed to address shared relational strain. The CBI model’s incorporation of CBCT and communication training provides couples with practical strategies to navigate stress and disappointment together. These results are consistent with prior work indicating that CBIs improve both relational satisfaction and treatment adherence in infertile couples (Peterson et al., 2003). 6
Marital Quality (DAS): Depicting the Shift in Scores.
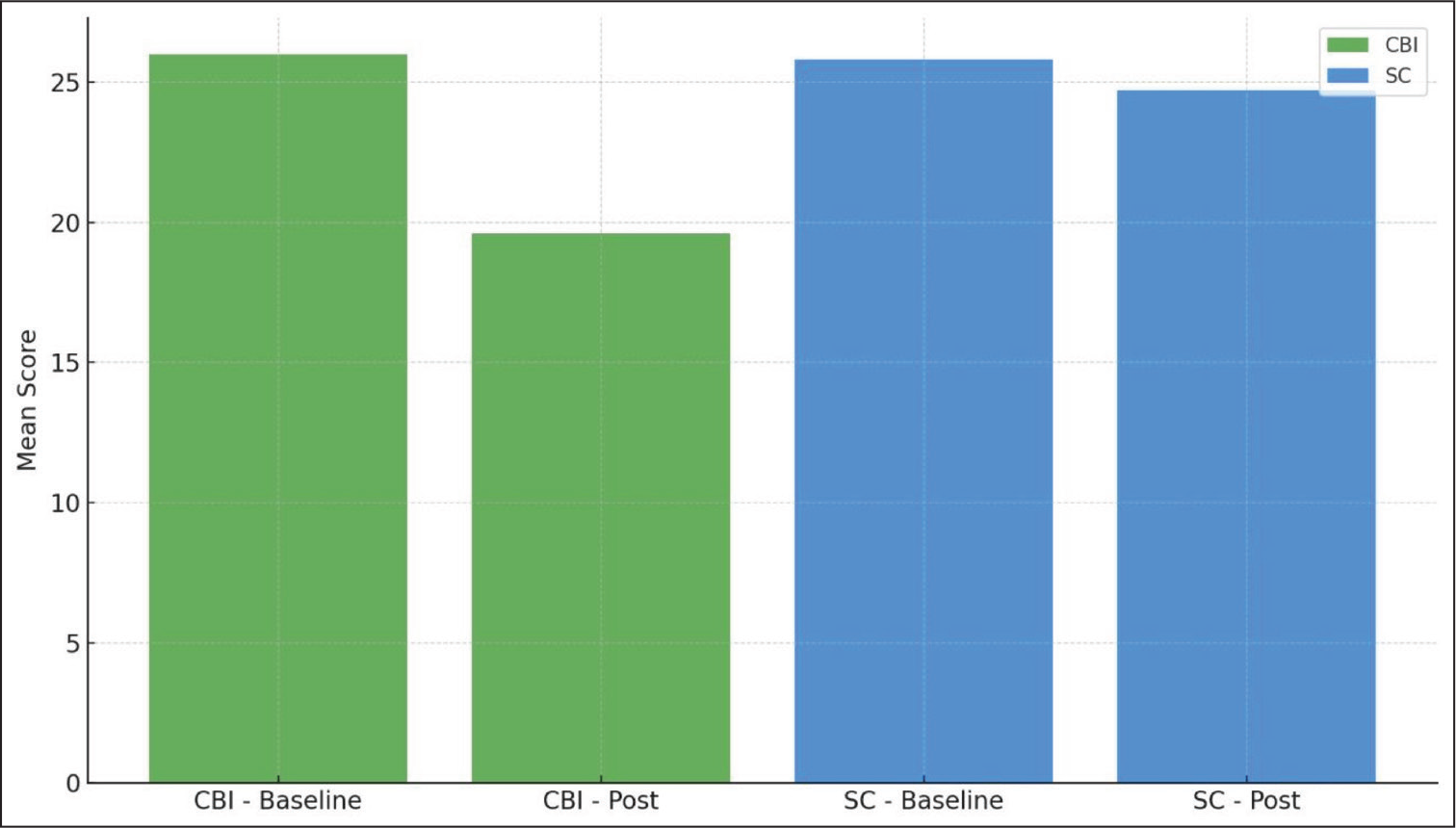
Most notably, the significant reduction in psychological distress (GHQ-28 scores) (Figure 3) among couples receiving CBI highlights the mental health benefits of collaborative support. Infertility-related distress is often internalized, particularly by women, and can involve feelings of guilt, inadequacy, and abandonment fears. By processing emotions together, couples can externalize the problem, reduce self-blame, and build emotional resilience. This finding is supported by prior evidence showing that psychosocial interventions delivered at the dyadic level result in greater reductions in anxiety and depression (Faramarzi et al., 2008). 7
Psychological Well-being (GHQ-28): Illustrating Reduced Distress Post-intervention in the CBI Group.
An additional insight from the demographic comparison was that urban residence was significantly associated with better outcomes in the CBI group. This may be due to higher health literacy, better access to mental health services, and greater familiarity with structured therapy among urban couples. Although not statistically significant, trends suggested that higher education levels were associated with better intervention uptake, potentially due to improved comprehension and engagement with therapeutic material.
Overall, these findings support the growing international consensus that dyadic models are best suited to address the psychosocial complexities of infertility. CBI appears to bridge the gap between medical treatment and relational healing, a crucial but often overlooked dimension in standard infertility care (Chan et al., 2020). 8
Conclusion
This study provides strong evidence that CBI is more effective than SC in improving sexual, relational, and psychological outcomes among couples facing infertility. The statistically significant changes observed in the CBI group across ISS, DAS, and GHQ-28 scores affirm the therapeutic value of addressing infertility as a shared emotional experience rather than an individual burden.
The use of EFT, cognitive behavioral couple strategies, sexual communication training, and joint mindfulness exercises within CBI offered couples a comprehensive toolkit to navigate infertility, not just as patients, but as partners. These techniques promoted emotional safety, intimacy, and psychological resilience, factors crucial not only for coping with infertility but also for enhancing relationship satisfaction and mental well-being. This is supported by Cousineau and Domar, who emphasized that couple-focused psychological interventions result in better coping and adjustment than individual-focused approaches. 9
Given the rising prevalence of infertility and its profound emotional toll, this study advocates for a paradigm shift in psychosocial infertility care, from individual-centered counseling to couple-centered therapeutic approaches. CBI should be integrated as a standard adjunct to infertility treatment, particularly in tertiary care centers and fertility clinics, where couples are navigating complex medical and emotional pathways. Additionally, Hjelmstedt et al. demonstrated that emotional adaptation improves significantly when psychosocial interventions are delivered jointly to couples, rather than individually. 10
Furthermore, clinicians must consider the role of sociodemographic facilitators, such as urban background and education, in influencing therapy outcomes. Tailoring CBI to suit diverse cultural and literacy contexts will be essential for ensuring broader accessibility and equity in care.
In conclusion, CBIs not only reduce the psychological burden of infertility but also strengthen the relationship, making couples more resilient, whether in continuing fertility treatments, exploring alternative parenting, or choosing to live childfree. Future research should explore the long-term effects of CBI and its adaptability across different socio-cultural settings.
Footnotes
Acknowledgements
We extend our sincere gratitude to the Department of Obstetrics and Gynecology, Saveetha Medical College and Hospital, and to all the couples who participated in this study. No third-party writing or editorial assistance was involved in the preparation or submission of this manuscript.
Authors’ Contribution
Dr Gayathri J: Data collection, analysis, and manuscript drafting
Dr Nithya Ragavi Rajendran: Conceptualization, study supervision, methodology design, and critical revision
Dr Raman K: Guidance on clinical framework, manuscript review, and final approval.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Scientific Review board at Saveetha Medical College and Hospital. Approval number: 438/06/2025/PG/SRB/SMCH.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from all participants prior to inclusion in the study, including consent for the publication of anonymized data.