
Abstract
Background:
Sexual dysfunction is one of the many health outcomes linked to professional life stress and burnout, which are becoming more widely acknowledged in the medical field. However, quantitative evidence on these relationships in the Indian health care context remains limited and warrants a systematic inquiry.
Objective:
To assess the relationship between sexual dysfunction, burnout, and work-related stress in married doctors and nurses working in a tertiary institution in India.
Methods:
This cross-sectional observational study included 202 married participants aged 21–53 years, comprising 153 doctors (75.7%) and 49 nurses (24.3%). The Professional Life Stress Scale (PLSS), Copenhagen Burnout Inventory (CBI), and Changes in Sexual Functioning Questionnaire (CSFQ) were completed by participants along with demographic and occupational data. Descriptive statistics, multivariable logistic regression, and Pearson correlations were performed.
Results:
Sexual dysfunction was present in 22.3% of the participants, and prevalence increased significantly with age. Participants with sexual dysfunction showed significantly higher levels of work-related stress and personal burnout than those without dysfunction. Strong negative correlations were found between professional life stress and sexual functioning (r = −0.85, P < .001) and between personal burnout and sexual functioning (r = −0.76, P < .001). Multivariable regression identified professional life stress and client burnout as independent predictors of sexual dysfunction.
Conclusions:
Professional life stress and burnout are strongly and independently associated with sexual dysfunction among doctors and nurses. These findings highlight the need for comprehensive occupational health programs that routinely assess burnout and sexual health, implement strategies to reduce professional stress and provide access to psychological support services, especially for vulnerable groups such as female healthcare workers (HCWs), nurses, and emergency workers.
Keywords
Introduction
Burnout and professional life stress are common sources of complaint for healthcare workers (HCWs) worldwide, affecting their mental and emotional well-being. 1 They are also vulnerable to burnout because of exhaustion, long hours, high patient volume, and daily exposure to serious, even tragic conditions. 2 Emotional exhaustion, depersonalization, and a lack of personal accomplishment are common characteristics of burnout, which can lower productivity at work and lower overall life satisfaction.3,4
Professional life stress is also an issue in healthcare. Such pressure can result from the burden of patient load, work overload, interpersonal tensions, and organizational demands. 5 Research has shown that doctors and nurses experience more work-related stress than most other workers. 6 Long-term exposure to this kind of stress has been linked to health problems, such as heart disease, musculoskeletal pain, and decreased immune function. 7
Tertiary care hospitals in India are the highest level of health care, providing advanced tertiary care services, complex diagnostic procedures, and multidisciplinary treatment of serious conditions, including trauma and critical care. Healthcare professionals in these settings face various challenges in their work, such as high numbers of patients, long hours, often more than 12 to 14 hours, frequent night shifts, and emergency shifts, exposure to critically ill and dying patients, a limited staff-to-patient ratio, and inadequate infrastructure and security measures. These tertiary institutions serve as referral centers for both secondary and primary health care institutions, which means that health professionals face an excessive burden of complex cases with limited resources. The demanding nature of the work in Indian tertiary care hospitals, marked by high emotional workloads, insufficient rest periods, and organizational pressures, creates a unique working environment that can have a significant impact on the professional and personal well-being of doctors and nurses. 8
Stress and burnout are not limited to work but can affect personal lives as well. Sexual dysfunctions, which include problems with sexual desire, arousal, or satisfaction, can be mentioned among the various sequels. It can also affect the quality of life and sexual relationships. The literature suggests that psychological stress, including burnout, could play a role in the development of sexual dysfunction. Burnout is a risk factor for erectile dysfunction in men and decreased sexual satisfaction in both sexes.9,10
Little is known about the influence of work-related stress and burnout on sexual function, and what we do know comes from general population studies. Although the relationship of psychological distress and sexual dysfunction has been observed in various other groups, such work in HCWs, especially doctors and nurses, has not been documented to a greater extent, particularly in India, and its setup, where the workplace settings and expected roles of an individual may modulate these associations.11,12
The current research aims to explore the relationship between work-related stress, burnout, and sexual dysfunction in healthcare professionals employed in a tertiary care hospital in India. This research seeks to better understand how these connections materialize and affect the personal lives of doctors and nurses. The results are expected to be used to improve our understanding of the general impact of work-related stress and burnout and to develop initiatives to support the sexual health of doctors and nurses.
Methods
Study Design, Setting, and Ethical Considerations
This cross-sectional observational study was conducted at a tertiary care hospital in India between March 2021 and January 2022. The primary objective was to assess the association between professional life stress, burnout, and sexual dysfunction among doctors and nurses. The Institutional Ethics Committee approved the study protocol, and all procedures were consistent with the Helsinki Declaration. 13 Written informed consent was taken from all participants. The participants were provided with assurances of anonymity and privacy in relation to their identity and the right to withdraw at any time without consequence.
Sample Size Calculation
Sample size was determined using the formula for finite population prevalence studies: n = NZ2 P(1 – P)/d2 (N – 1) + Z2 P(1 – P) where Z is the Z statistic for a 95% confidence level (1.96), N = 600 (population size), P = .15 (expected proportion of participants showing the characteristic of interest), and d is the absolute precision 0.05 (5%). Allowing for non-response, the minimum required sample was 200 participants.
Participants
A total of 202 married doctors and nurses, aged 21–53 years, were recruited using convenience sampling. The sample included 153 doctors (75.7%) and 49 nurses (24.3%) from both clinical and non-clinical departments. Current marriage, age 21–53 years, and employment at the study hospital were included. A history of major psychiatric illness or other comorbidities such as hypertension, diabetes mellitus, addictions, current use of medications known to affect sexual function, and refusal to participate were excluded.
Data Collection
Data were collected using a structured, self-administered questionnaire that asked about demographics, professional life stress, burnout, and sexual functioning. Questionnaires were completed in a private, confidential setting to ensure participant anonymity. Demographic and occupational profile information was recorded, which included age, gender, occupation (doctor or nurse), specialty, emergency on-call status, and marital status.
Assessment Tools
Professional Life Stress Scale (PLSS) (David, 1989): The PLSS is a 24-item validated instrument for assessing work-related stress. Scores range from mild to moderate, with higher scores indicating greater stress levels. 14
Copenhagen Burnout Inventory (CBI) (Kristensen et al., 2005): The CBI is a 19-item scale measuring three burnout areas: Personal, work-related, and client-related burnout. Higher mean scores reflect more burnout. 15
Changes in Sexual Functioning Questionnaire (CSFQ) (Clayton et al., 1997): The CSFQ is a 14-item measure that assesses current versus previous sexual functioning. Scores of ≤41 for females and ≤47 for males indicate sexual dysfunction.16,17
Statistical Analysis
Data were analyzed using IBM SPSS Statistics for Windows, version 28.0 (IBM Corp; 2021; Armonk, NY). Before assessment normality of distribution for the primary variables (PLSS, CBI, CSFQ scores) was formally assessed using the Shapiro-Wilk test. Frequent and percentage data were summarized as frequencies and percentages; continuous data as mean ± standard deviation (SD) or median (interquartile range), as appropriate. Group comparisons were performed using independent t tests or one-way analysis of variance (ANOVA) for continuous variables and chi-square tests for categorical variables.
Correlations between professional life stress, burnout, and sexual functioning were evaluated using Pearson correlation coefficients. Multivariate linear and logistic regression analyses were performed to identify independent predictors of sexual dysfunction, controlling for potential confounders (age, sex, occupation, specialty, emergency duty status). Sexual dysfunction was the dependent variable; professional life stress, burnout domains, and demographic variables were independent predictors. Statistical significance was set at P < .05 (two-tailed). Model fit was assessed using pseudo R2 (McFadden), sensitivity, specificity, and classification accuracy.
Results
The study participants were 202 doctors and nurses who had an average age of 34.42 years. Of the participants, 110 (54.46%) were male, and 92 (45.54%) were female. All 202 participants (100%) were married. Of these, 153 (75.74%) were doctors, while 49 (24.26%) were nurses. Additionally, 185 (91.58%) of the HCWs were from clinical specialties, and 17 (8.42%) were from non-clinical specialties. In addition, 121 (59.90%) of the participants were in specialties where attendance at emergencies was part of their routine work, while 81 (40.10%) were from non-emergency departments.
Based on the sexual history of the participants, 128 (63.40%) initiated sexual intercourse verbally, while 74 (36.60%) initiated sexual intercourse physically. During intercourse, verbalization during intercourse, and afterplay, all participants (100%) participated in foreplay, verbalization during intercourse, and afterplay. Among the feelings reported after engaging in sexual activities, 126 (62.40%) felt relaxed, 70 (34.70%) felt loved, and 6 (3.00%) felt tense. Considering marital disagreements, the participants reported that 200 (99.00%) participants reported no conflict, and 2 (1.00%) participants reported some relationship conflict. With respect to the first sexual intercourse with a spouse, 201 participants (99.50%) reported it as satisfying, while only 1 (0.50%) reported it as disappointing. Regarding the effects of having children on marriage, regarding sexual activity, 120 (59.40%) indicated a reduction in sexual activity. Furthermore, no participants reported extramarital relations. Sexual functioning within this population is currently being studied.
The specialty-wise distribution of physicians showed that the largest groups were general surgery (28, 18.30%) and general medicine (23, 15.03%). Orthopedics (12, 7.84%), pediatrics (8, 5.23%), and radiology (9, 5.88%). The least represented specialties were biochemistry, cardiology, and cardiovascular surgery, each contributing one participant (0.65%). In nursing, the most common workplace settings for general specialties were general surgery (10, 20.41%) and obstetrics and gynecology (6, 12.24%). Other workplaces were pediatrics (2, 4.08%) and ophthalmology (2, 4.08%), with one nurse each from emergency medicine and psychiatry, and urology (2.04%).
Most of the participants, specifically 160, showed mild stress with an average PLSS score of 7.21 ± 3.563. A total of 41 participants (20.29%) were recorded with an average score of 21.71 ± 3.614. Only one participant (0.49%) fell under the major stress category, reporting an average score of 31.00 ± 0.000. No participant claimed severe stress. It can be inferred that most HCWs experienced mild to moderate stress levels during their work.
Burnout was measured using the CBI, which examines personal, work-related, and client-related burnout. For personal burnout, the average score was 26.75 ± 16.65, indicating moderate exhaustion. Work burnout averaged 34.78 ± 15.51, indicating a moderately high level of fatigue due to work-related stress. Client burnout, which assesses the emotional and mental exhaustion associated with professional interactions with patients and clients, had the greatest average of the three components at 35.91 ± 16.10, suggesting that emotional exhaustion is associated with client interactions. These outcomes reveal differentiation in HCWs professional dimensions of experience relative to the degree of burnout.
Table 1 shows the correlation between burnout, professional life stress, and demographic factors. There were clear disparities between males and females. Females had higher levels of stress in professional life (t = −3.98, P = .002), personal burnout (t = −4.60, P = .004), and work burnout (t = −1.01, P < .001). Males had a greater prevalence of client burnout (t = 0.32, P = .003). Nurses had higher levels of professional life stress (t = −2.86, P = .003), personal burnout (t = −3.88, P < .001), work burnout (t = −3.88, P = .001), and client burnout (t = −3.88, P = .001) when compared to doctors. Those working in a clinical setup had significantly more professional life stress compared to those in a non-clinical setup. Similarly, those who had emergency duties also had greater professional life stress and personal burnout compared to their non-emergency counterparts. These findings demonstrate the significant effect of gender, occupation, specialty, workplace, and environment on the degree of stress and burnout experienced by HCWs.
Correlation of Demographic and Sexual History Variables with Professional Life Stress and Burnout.
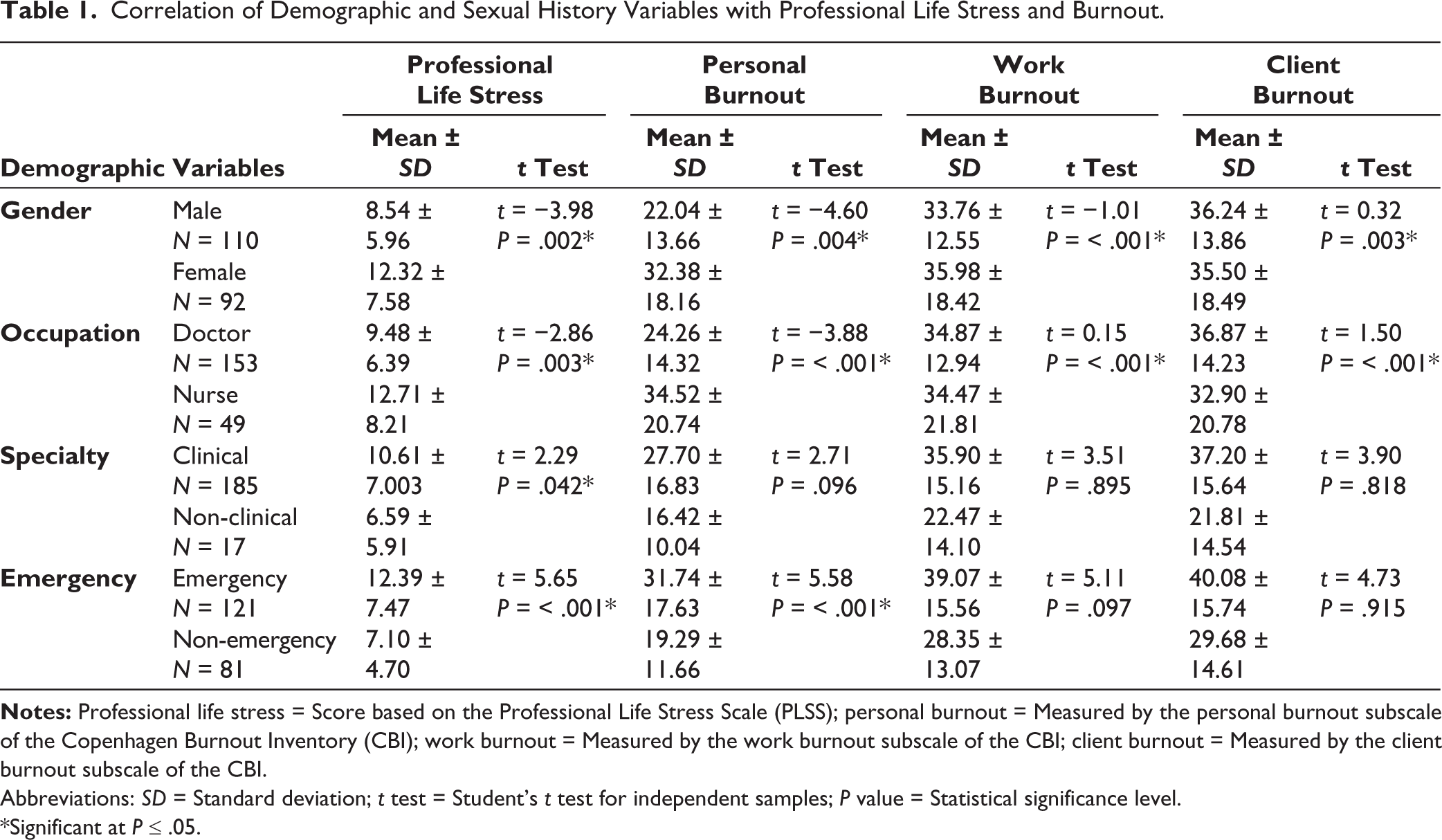
Abbreviations: SD = Standard deviation; t test = Student’s t test for independent samples; P value = Statistical significance level.
*Significant at P ≤ .05.
Table 2 presents the professional life stress and burnout correlation using Pearson’s method. A strong positive correlation was identified between professional life stress and all three burnout types. There was the strongest correlation between professional life stress and personal burnout (r = 0.816, P < .001), followed by work burnout (r = 0.741, P < .001) and client burnout (r = 0.669, P < .001). These results imply that burnout in all its manifestations, personal, professional, and client, increases in tandem with greater professional life stress. This emphasizes how professional life stress has a major role in making burnout among HCWs worse.
Pearson Correlation of Professional Life Stress with Burnout.
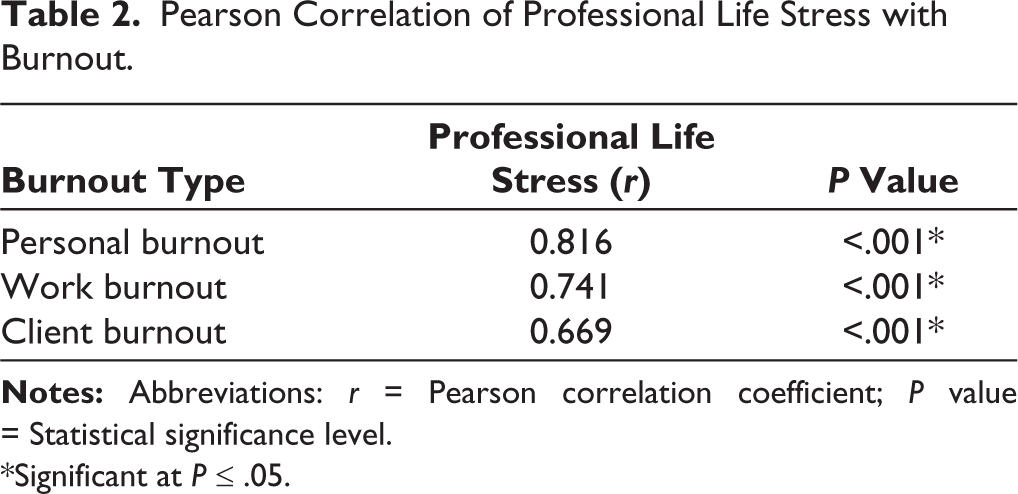
*Significant at P ≤ .05.
Sexual dysfunction was found in 45 participants (22.27%), whose mean score was 40.38 ± 4.57. The other 157 participants (77.72%) who did not have sexual dysfunction had a higher mean score of 53.38 (SD = 5.36). These findings suggest that approximately one-fifth of HCWs in this investigation exhibited sexual dysfunction, as evidenced by a lower total CSFQ score. The types of sexual dysfunction experienced by participants were assessed in different areas of the CSFQ. Out of 45 participants reporting sexual dysfunction, 38 (84.44%) had low sexual desire, 30 (66.67%) had low arousal, and 28 (62.22%) had difficulty with orgasm. The least common variant was the pain or discomfort variant, which affected 10 (22.22%) participants.
The relationship between demographic factors, sexual history, and total CSFQ scores in the affected group is described in Table 3. Considering sex as a demographic variable, males performed better than females in total CSFQ scoring (CSFQ 43.16 ± 3.23; VS 36.90 ± 3.52; t = 6.19, P < .001). This showed that females had more impaired compared to males. Occupational differences were also noteworthy; doctors scored better compared to nurses (CSFQ 41.51 ± 4.16; VS 36.40 ± 3.77; t = 3.48, P = .001). This study shows that dysfunction was greater in nurses compared to doctors. There was no significant difference observed based on specialty (clinical vs. non-clinical) or on the way sexual intercourse began (verbal vs. physical). No significant differences were noted in relation to the influence of pregnancies and children on marital sex as well as feelings of relaxed, tense, or loving post-coital states. Overall, gender and occupation have been shown to have a significant effect on sexual dysfunction, whereas factors related to sexual history have not shown any remarkable relationships.
Correlation of Demographic and Sexual History Variables with Total CSFQ Scores of Participants with Sexual Dysfunction (n = 45).
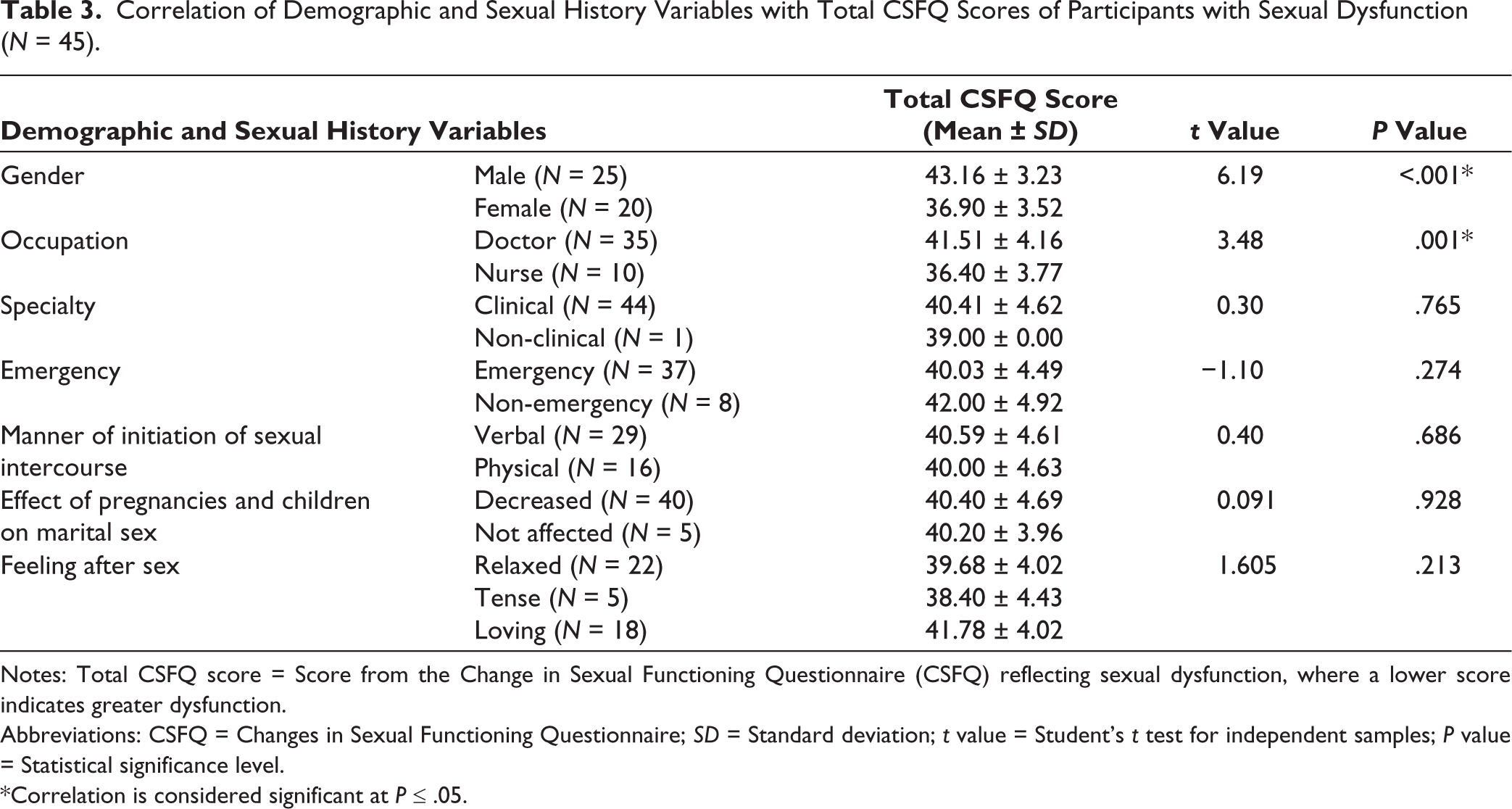
Abbreviations: CSFQ = Changes in Sexual Functioning Questionnaire; SD = Standard deviation; t value = Student’s t test for independent samples; P value = Statistical significance level.
*Correlation is considered significant at P ≤ .05.
There were notable variations in sexual functioning between the sexes, as shown in Table 4. Males demonstrated superior sexual functioning compared to females, as evidenced by significantly lower dysfunction in sexual desire or frequency (P = .008), sexual desire or interest (P < .001), sexual arousal or erection (P < .001), and sexual orgasm or ejaculation (P = .014). Compared to nurses, doctors showed significantly less dysfunction in sexual desire or interest (P = .026) and sexual arousal or erection (P < .001), indicating better sexual functioning. However, no significant differences were found according to specialty, how sexual activity was initiated, the impact of pregnancies on marital sex, or feelings after sex (P > .05), indicating that these factors did not significantly affect sexual functioning in the study sample.
Correlation of Demographic and Sexual History Variables with Sexual Dysfunctions (as per CSFQ Subscale Components Scores).
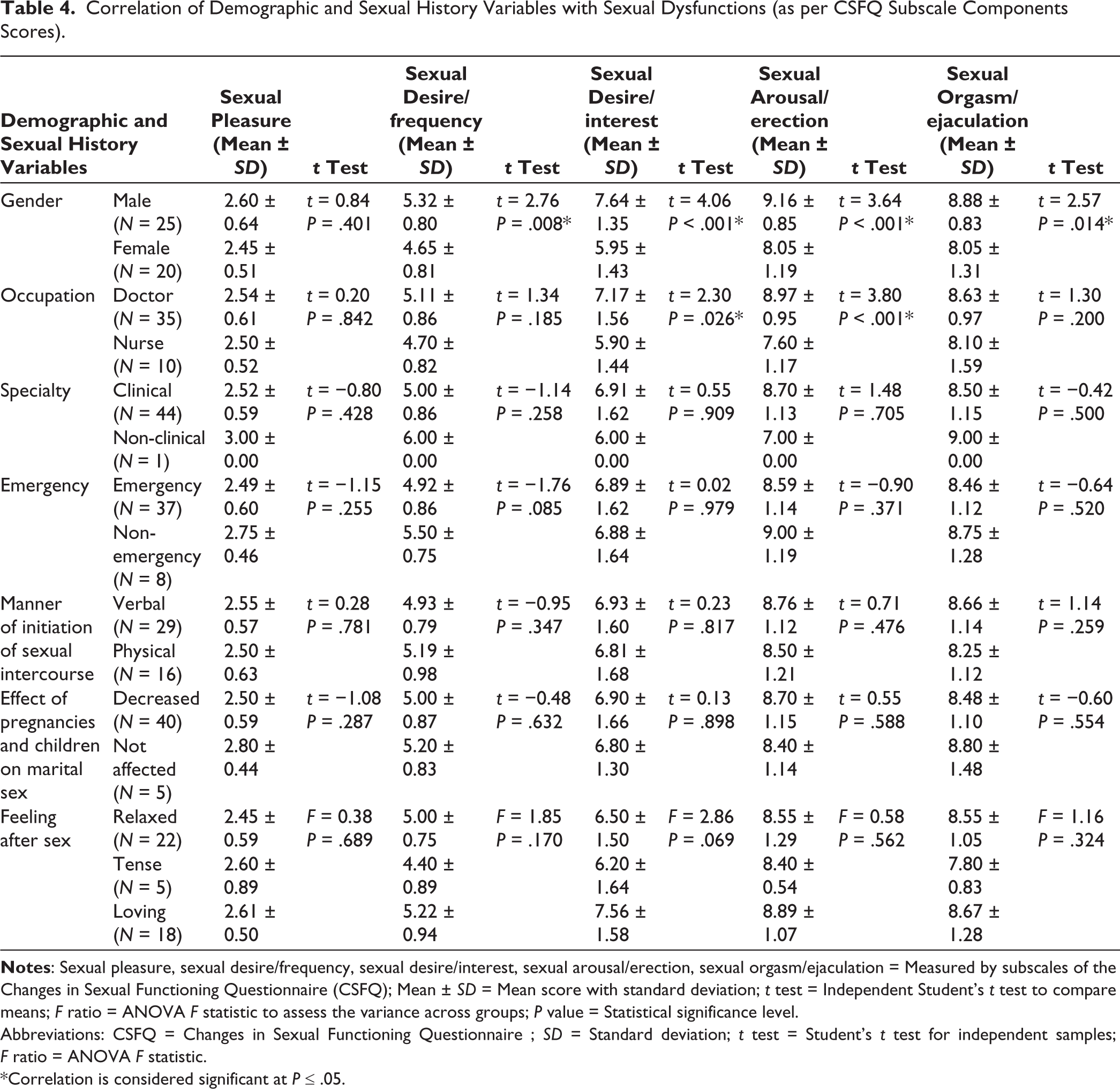
Abbreviations: CSFQ = Changes in Sexual Functioning Questionnaire; SD = Standard deviation; t test = Student’s t test for independent samples; F ratio = ANOVA F statistic.
*Correlation is considered significant at P ≤ .05.
Sexual dysfunction participants’ professional life stress scores (10.22 ± 7.58) and those without (10.28 ± 6.84; t = −0.049, P = .961) do not differ significantly, according to Table 5. However, burnout significantly increased in individuals with sexual dysfunction. Sexual dysfunction was significantly correlated negatively with all three types of burnouts: personal (r = −0.755, P < .001), work-related (r = −0.710, P < .001), and client (r = −0.650, P < .001).
Correlation of Sexual Dysfunction Based on Total CSFQ Score with Professional Life Stress and Burnout Scores.
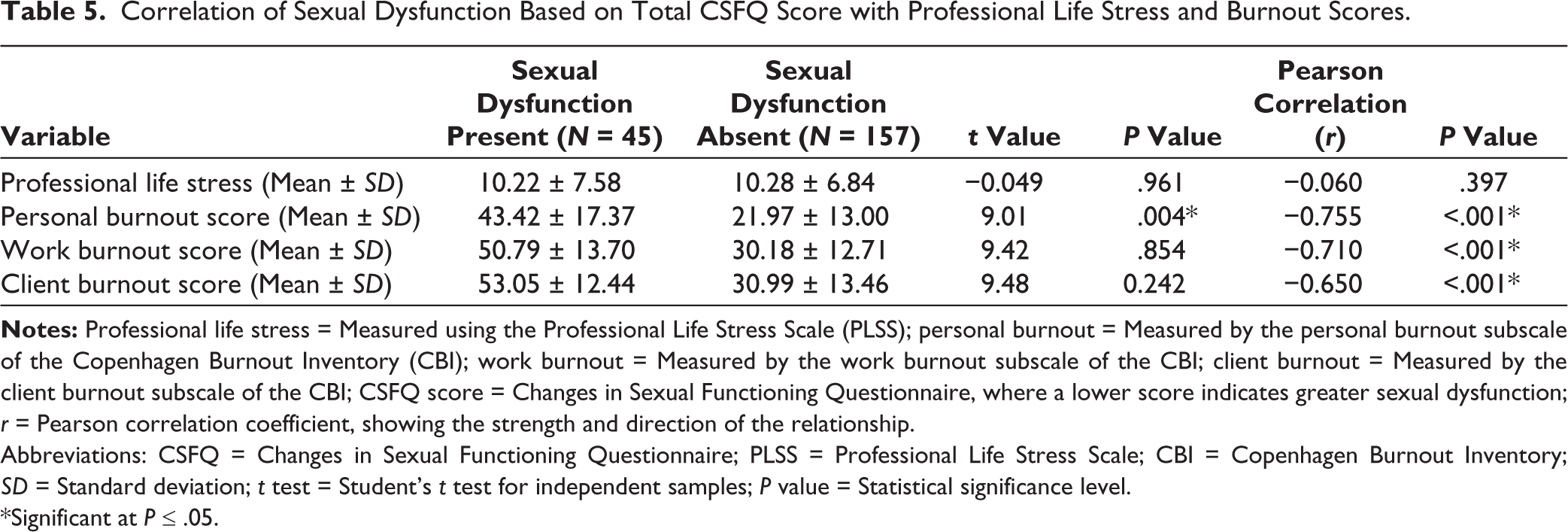
Abbreviations: CSFQ = Changes in Sexual Functioning Questionnaire; PLSS = Professional Life Stress Scale; CBI = Copenhagen Burnout Inventory; SD = Standard deviation; t test = Student’s t test for independent samples; P value = Statistical significance level.
*Significant at P ≤ .05.
Table 6 shows a significant correlation between sexual dysfunction and professional life stress severity, as measured by cumulative CSFQ scores. The ANOVA results show that participants with mild professional life stress had higher CSFQ scores compared to those with moderate stress (40.20 ± 4.320) and major stress (32.00 ± 0.000), with a significant F ratio of 107.95 and P < .001. These findings suggest that increased professional life stress is associated with greater sexual dysfunction, with the severity of sexual dysfunction worsening as stress levels increase.
Correlation of Professional Life Stress with Sexual Dysfunction Based on Total CSFQ Score.
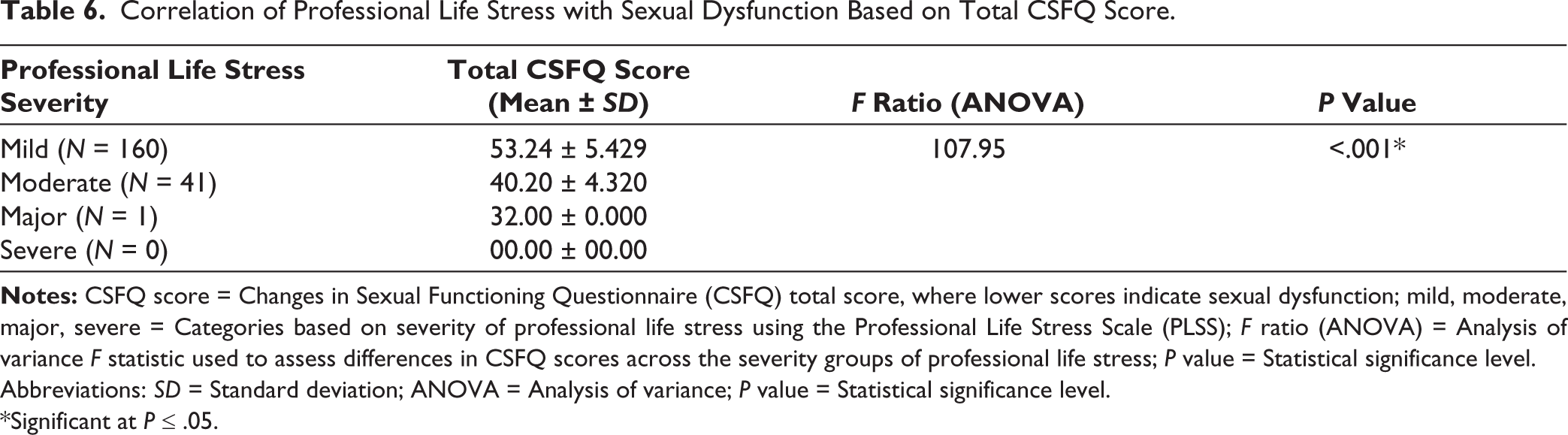
Abbreviations: SD = Standard deviation; ANOVA = Analysis of variance; P value = Statistical significance level.
*Significant at P ≤ .05.
In Table 7, doctors and nurses are documented with their sexual dysfunction and related predictors in a logistic regression analysis. Age, professional life stress, and client burnout were relevant predictors, which showed that older age, work-related stress, and emotional exhaustion contributed to sexual dysfunction. Personal burnout and work burnout showed no significance. The model fit the data well and showed a pseudo R2 of 0.567 along with high sensitivity and specificity, which indicates a 56.7% of the variance is contributed by the predictor variables on the criterion variable sexual dysfunction.
Logistic Regression Analysis Predicting Sexual Dysfunction.
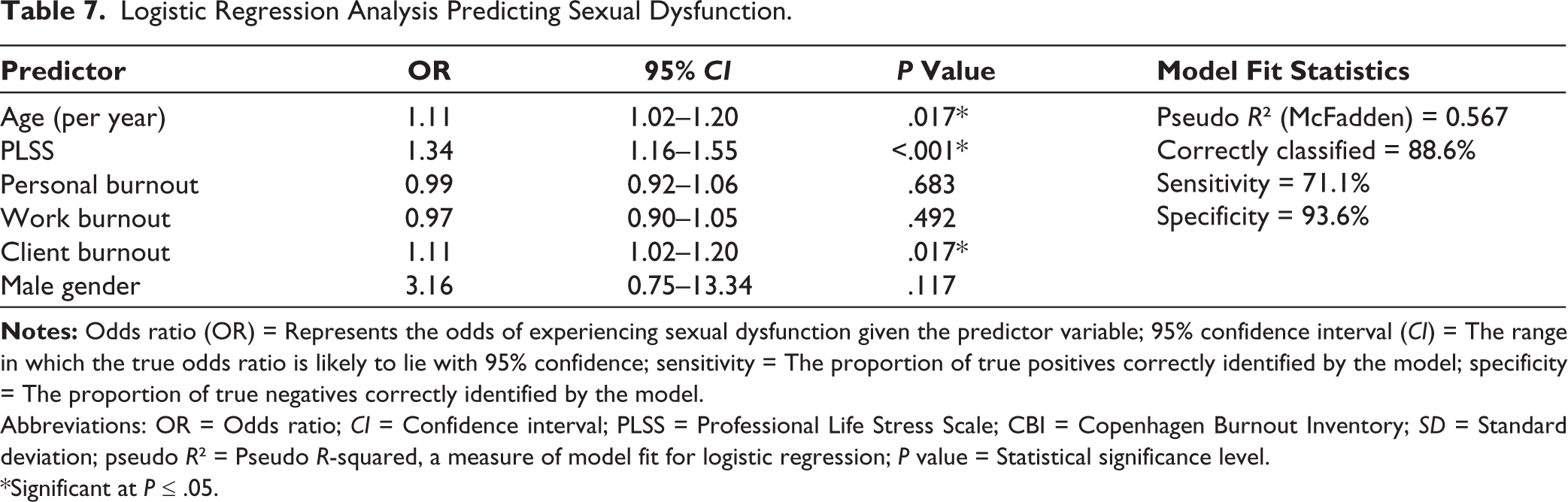
Abbreviations: OR = Odds ratio; CI = Confidence interval; PLSS = Professional Life Stress Scale; CBI = Copenhagen Burnout Inventory; SD = Standard deviation; pseudo R² = Pseudo R-squared, a measure of model fit for logistic regression; P value = Statistical significance level.
*Significant at P ≤ .05.
Discussion
This study provides a detailed analysis of the relationship between professional life stress, burnout, and sexual dysfunction among doctors and nurses in a tertiary care hospital in India. It provides evidence of associations between these factors and their implications for individual health and healthcare system performance.
In this study, the prevalence of sexual dysfunction was 22.3%, with rates for men and women being almost equal. Although higher than estimates for the general population, this number is consistent, or lower than earlier research among HCWs, which found rates ranging from 15% to 50%.18–22 The multifactorial nature of sexual health disorders in high-stress occupational settings is reflected in the prevalence of erectile and ejaculatory disorders in men and desire, arousal, and orgasmic disorders in women.23,24 Sexual dysfunction was notably more prevalent in older age groups, with 53.1% in those aged 41–53 years compared to 13.5% in the 21–30 year group. This age-related increase is consistent with literature linking hormonal changes, comorbidities, and cumulative professional life stress to declines in sexual function.19,25,26 The compounding effect of chronic stress and aging may further exacerbate vulnerability to sexual dysfunction in HCWs.25,27,28
Most participants reported mild or moderate professional life stress, with only a small fraction experiencing major stress. Client-related burnout was the most common cause of burnout, followed by work and personal burnout. Indian and international research document high rates of burnout, especially emotional exhaustion and depersonalization, among HCWs, particularly those in patient-facing and emergency roles.9,11 The emotional toll of patient care, long hours, night shifts, lack of organizational support, exposure to traumatic events, and heavy workloads are all significant contributing factors. The COVID-19 pandemic exacerbated these stresses, leading to increased burnout in the health care sector. Two meta-analyses have shown that COVID-19 has a significant effect on burnout, emotional exhaustion, and traumatic stress in HCWs.29,30 Our research data collection was also carried out during the pandemic, which may have amplified the effects. Risks of this problem are increased by organizational problems such as limited autonomy, performance-based compensation, and insufficient staffing.31,32
Female HCWs and those working in emergency departments had a higher rate of workplace stress and personal burnout. Female HCWs are at higher risk for professional life stress and burnout due to gendered expectations, emotional labor, and work-life conflict.33,34 The unpredictability, crowding, and need for quick decisions make emergency situations especially stressful, which exacerbates emotional exhaustion and depersonalization.35,36 A strong positive correlation was observed between professional life stress and all three domains of burnout (personal, work, and client-related). These findings support the theory of “demand-control” and “effort-reward imbalance” models, which posit that high job strain and low control precipitate chronic stress and burnout.37,38
The strong association between professional life stress, burnout, and sexual dysfunction is a central finding in this study. The burnout domains and CSFQ scores were significantly higher in participants with sexual dysfunction. This means that as burnout increases, sexual functioning deteriorates. This relationship is supported by recent meta-analyses and cross-sectional studies.9,10,22
The linkage between chronic stress, burnout, and sexual dysfunction is complex and is mediated by both psychological and biological pathways.9,15 Long-term stress and burnout can interfere with the function of the body’s neuroendocrine system, resulting in certain hormone imbalances, including high levels of cortisol that can blunt the libido, cause mood swings, and depress sexual response and fulfillment.9,10,39 Emotional exhaustion, burnout’s central component, correlates most with sexual problems, in that it reduces emotional resources or emotional stores of energy and intimacy, which in turn makes it more difficult to feel desire and to experience fulfillment.9,10 Neurobiologically, chronic stress can lead to alterations in brain areas associated with sexual function (e.g., prefrontal cortex, amygdala), induce neuroinflammation, oxidative stress, and synaptic disturbances, which are predisposed to compromised sexual functions.40–42 High-stress in women was associated with increased cognitive distraction and cortisol, which in turn were negatively associated with genital arousal. 40 Onset of erectile dysfunction is associated with burnout and personal stress in men.9,43 Internalizing stress can exacerbate the detrimental effects on sexual health by causing emotional disengagement and intimacy issues.9,10,40 Taken together, these results demonstrate that emotional exhaustion and neuroendocrine impairment are involved in the link between chronic stress, burnout, and sexual dysfunctions.9,10,40,42 There was also a significant correlation between sexual dysfunction and client burnout or fatigue from patient care. This suggests that healthcare professionals’ personal lives may be impacted by the emotional toll of providing care. Employees who work in emotionally charged fields such as emergency departments or oncology are especially susceptible to client burnout, which can result in depersonalization and withdrawal from interpersonal relationships, including sexual ones.10,44,45
As per the multivariable regression analysis, sexual dysfunction was significantly predicted by age, client burnout, and PLSS score. Any increase in professional life stress was associated with an increase in the odds of sexual dysfunction, highlighting the significant impact of professional life stress on sexual health. Client burnout as a significant predictor highlights the importance of addressing burnout due to patient care.10,46,47 Age independently predicted sexual dysfunction, with increased prevalence among older doctors and nurses, which is consistent with prior studies that have attributed greater prevalence of sexual dysfunction among older adults to biological and psychological factors, as well as professional life stress.12,15,19,48 On the other hand, systematic reviews by Kiratipaisarl et al. (2024) and Ong et al. (2024) propose that interventions based on organizational support and mindful practice reduce the effectiveness of burnout, which could indirectly reduce sexual dysfunction by improving well-being.49,50
Implications for Policy and Practice
Routine assessment for burnout and sexual dysfunction ought to be integrated into occupational health programs, along with pathways for referrals to psychological and sexual health services.
Organizational strategies such as managing workloads, providing peer and supervisory support, offering mental health resources, and implementing stress reduction initiatives are essential, particularly for vulnerable groups (such as female HCWs, nurses, and emergency personnel).
To address the difficulties faced by female HCWs, gender-sensitive tactics such as mentorship programs, gender-equitable policies, and specialized mental health resources may be helpful.
Multicenter and longitudinal studies should be a part of future research to assess the efficacy of interventions and gain a better understanding of causal relationships.
Strengths and Limitations
This research has certain advantages, including a decent sample size, the application of validated assessment tools (PLSS, CBI, and CSFQ), and a comprehensive analysis of demographic, occupational, and psychological factors. The inclusion of doctors and nurses from diverse specialties enhances its generalizability. Among the limitations, the inability to infer causality due to the cross-sectional design, small single-center setting, and reliance on self-report data, which is prone to social desirability and recall bias, are notable. Also, the applicability to the greater population may be limited due to the focus on HCWs who are not married and those who do not have important mental health issues or do not take certain medications. There’s a need for longitudinal studies to evaluate the effectiveness of proposed interventions and clarify the causal pathways.
Conclusion
This study shows a strong and direct correlation between burnout, sexual dysfunction, and professional life stress among doctors and nurses. Reducing sexual functioning is closely associated with burnout on both a personal and professional level, as well as client-related fatigue among female HCWs, nurses, and those in emergency and clinical specialties. The results above show the need for comprehensive occupational health approaches that address the psychological and sexual health of healthcare professionals.
Footnotes
Acknowledgements
The authors express their sincere gratitude to all the doctors and nursing staff for their support in making this study possible by providing their valuable time and information.
Authors’ Contribution
Conceptualization: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Lakhan Kataria, Dr. Jahnavi Bhatt Data curation: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Dhruv Raval, Dr. Prajesh Kalathiya Formal analysis: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Lakhan Kataria, Dr. Prajesh Kalathiya Funding acquisition: Not applicable. Investigation: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Jahnavi Bhatt Methodology: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Lakhan Kataria Project administration: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Lakhan Kataria Resources: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Dhruv Raval Software: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Dhruv Raval, Dr. Prajesh Kalathiya Supervision: Dr. Lakhan Kataria Validation: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Jahnavi Bhatt Visualization: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Dhruv Raval, Dr. Prajesh Kalathiya Writing, original draft: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Lakhan Kataria, Dr. Jahnavi Bhatt, Dr. Dhruv Raval, Dr. Prajesh Kalathiya Writing, review, and editing: Dr. Nisheet Patel, Dr. Dharmin Shah, Dr. Lakhan Kataria, Dr. Jahnavi Bhatt, Dr. Dhruv Raval, Dr. Prajesh Kalathiya
Data Sharing Statements
Data can be made available upon request by the authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimers
The views expressed in this manuscript are solely those of the authors and do not necessarily represent the views of their affiliated institutions.
Ethical Approval
The Sumandeep Vidyapeeth Institutional Ethics Committee approved the study protocol (approval number SVIEC/ON/Medi/BNPG20/D21026 dated January 25, 2021), and all procedures were consistent with the Helsinki Declaration. Written informed consent was taken from all participants. The participants were provided with assurances of anonymity and privacy in relation to their identity and the right to withdraw at any time without consequence.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was taken from all participants. The participants were provided with assurances of anonymity and privacy in relation to their identity and the right to withdraw at any time without consequence.
Patient Consent
Not applicable.
Prior Presentations
Not done.
Simultaneous Submission to Another Journal or Resource
None.