
Abstract
Background:
It is generally assumed that erectile dysfunction (ED) under the age of 40 is primarily driven by psychosocial factors.
Aims
This cross-sectional study evaluated ED, depression, anxiety, and quality of life among young Japanese men.
Materials and Methods:
We used an online survey to gather data from a wide range of community samples. ED was assessed by the IIEF-5 questionnaire, while depression, anxiety, and quality of life were assessed by the PHQ-9, GAD-7, and LISAT-8 questionnaires, respectively. Categorical data were evaluated by chi-square test and numerical data were estimated by one-way ANOVA. Post-hoc tests were conducted using the Holm method, which was used to control for type I errors. Cohen’s d index was calculated as effect sizes.
Results:
Valid responses from 329 individuals (age 33.93 ± 6.41 years) were obtained. According to IIEF-5 scores, the distribution of various severities of ED was as follows: non-ED, 37.39%; mild ED, 18.24%; mild to moderate ED, 27.36%; and moderate and severe ED, 17.02%. There were no significant differences in depression and anxiety between non-ED and ED men. In contrast, there were significant differences in quality of life between non-ED and ED men (P < .01).
Conclusions:
We conclude that psychosocial factors may also be the cause of ED in young Japanese men besides depression and anxiety, and ED may reduce quality of life in various aspects. It is necessary to develop a Japanese version scale to measure ED-related psychosocial factors.
Introduction
Erectile dysfunction (ED) is a male sexual disorder characterized by the inability to obtain and/or maintain a penile erection sufficient for satisfactory sexual performance. 1 ED has been a common disease worldwide with high reported morbidity rate.2,3 ED patients were identified in an estimated 34.5% of Japanese men. 4
In Japan, Sugimori et al. surveyed relationships among ED, depression, and anxiety. 5 In their study, the subjects were 1,419 non-institutionalized Japanese men aged 40–64 years. As a result, ED associated significantly with depression and anxiety status only in the late 40s to early 50s (45–55 years). As ED prevalence varies across racial, cultural, religious, and socioeconomic backgrounds, 6 psychological associations (depression and anxiety) with ED in Japanese men may be in a different situation from previous studies. For example, the Massachusetts Male Aging Study 7 demonstrated a strong positive association within a much wider age distribution (40–70 years). It was suggested that inconsistent results in “late” adulthood with previous studies might be partly explained by older Japanese men experiencing less difficulty adjusting to life with ED than younger Japanese men. From this result, there might be three sub-types of ED assessed by IIEF-5 in the Japanese general male population, comprised of EDs in “early” (less than 45 years), “middle” (45–54 years), and “late” (55 years or more) adulthood.
By now, there are several review papers and clinical guidelines available on ED, but many of these papers approach the assessment and treatment of ED from a purely medical perspective and pay only little attention to describing the psychosocial factors of ED. 8 Because the introduction of phosphodiesterase-5 inhibitors (PDE5Is) such as sildenafil, tadalafil, vardenafil, and avanafil has dramatically changed the therapeutic approach to the ED, they have become the first-line treatment for most patients.9,10 However, pharmacological treatment alone does not respond to all the concurrent factors of ED, including anxiety, loss of self-esteem, depressed mood, a couple’s communication problems, relationship problems, or a partner’s sexual dysfunction. 11 A systematic review of the psychosocial outcomes associated with erectile dysfunction suggested the importance of evaluating psychosocial factors associated with ED and its treatment. 12 In fact, ED has shown an influence on psychosocial health with 63.1% of ED patients developing psychiatric symptoms. 13 In particular, depression is known to be associated with ED. 14
It is widely assumed that ED in men under the age of 40 is primarily caused by psychosocial factors, whereas ED in older men is more likely to be caused by biological factors. Moore et al. showed a difference in symptom patterns among ED patients according to age groups. 15 They reported that younger men had comparatively greater depressive symptoms, accompanied by lower relationship satisfaction, more negative reactions from partners, and lower job satisfaction. However, the association of depression, anxiety, and quality of life with ED of different severity ratings in young Japanese men is unknown. Therefore, this cross-sectional study using standardized self-administered assessments aimed to evaluate depression, anxiety, and quality of life in the context of ED severity using the International Index of Erectile Function (IIEF-5) questionnaire 16 in young Japanese men.
Participants and Methods
Participants
To gather data from a wide range of community samples, we used an online survey conducted with the assistance of a marketing research service provider, Rakuten Insight, Inc., in Japan. Based on the IIEF-5 cutoff point, all severities were recruited to include a certain percentage of patients. All enrolled participants followed these criteria: (a) male; (b) 20–44 years old; and (c) married or living with a fixed sexual partner for more than 6 months. Besides, the exclusive criteria were as follows: (a) sexual dysfunction caused by Peyronie’s disease or other organic lesions of the external genitalia; (b) organic diseases such as diabetes, chronic kidney disease, and cardiac disease; and (c) a history of sertraline or other medicines that may influence their erection and psychological symptoms.
Participants first read an explanation that this survey would be conducted anonymously, and that they would not be forced to respond. Subsequently, only those who agreed to participate in this study responded to the questionnaires. As a reward, respondents received points that they could redeem for goods within the system of the survey company.
Measurements
International Index of Erectile Function-5
The Japanese version of IIEF-5 is a 5-item self-report questionnaire designed to measure erectile function. 17 Items are rated on a 5-point Likert-type scale, ranging from 1 to 5. The total score can range from 5 to 25, with high scores meaning high erectile function. Based on the original validation studies, the total score can then be interpreted as suggesting “no ED” (22–25); “mild ED” (17–21); “mild-to-moderate ED” (12–16); “moderate ED” (8–11); and “severe ED” (1–7).
Patient Health Questionnaire-9
The Japanese version of PHQ-9 is a 9-item self-report questionnaire designed to measure depression. 18 This scale evaluates each of the 9 DSM-IV (the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition) criteria for major depressive disorder. Items are rated on a 4-point Likert-type scale, ranging from 0 to 3. The total score can range from 0 to 27, with high scores meaning high depression. Based on the original validation studies, the total score can then be interpreted as suggesting no depression (0–4), mild depression (5–9), moderate depression (10–14), moderately severe depression (15–19), or severe (20–27). A cut-off score of 10 is suggested as indicating a possible diagnosis of depressive disorder.
Generalized Anxiety Disorder-7
The Japanese version of GAD-7 is a 7-item self-report questionnaire designed to measure generalized anxiety disorder. 19 This scale evaluates each of the seven DSM-IV criteria for generalized anxiety disorder. Items are rated on a 4-point Likert-type scale, ranging from 0 to 3. The total score can range from 0 to 21, with high scores meaning high anxiety. Based on the original validation studies, the total score can then be interpreted as suggesting no anxiety (0–4), mild (5–9), moderate (10–14), or severe (14–21). A cutoff score of 10 is suggested as indicating a possible diagnosis of generalized anxiety disorder.
Life Satisfaction Checklist-8
The Japanese version of Life-11 is an 11-item self-report questionnaire (LISAT-11) designed to measure life satisfaction. 20 In this study, we used an 8-item version based on the original version. 21 This scale evaluates satisfaction with eight different aspects of the patient’s life; life in general, sexual life, relationship with a partner, family life, relationship with friends, leisure, professional, and financial situation. Items are rated on a 6-point Likert-type scale, ranging from 1 to 6. The total score can range from 8 to 48, with high scores meaning high satisfaction. All items can be grouped in three dimensions: satisfaction with social life (items 1 and 4–6), satisfaction with affective life (items 2 and 3), and satisfaction with financial life (items 7 and 8).
Statistical Analysis
We used mean ± standard deviation (SD) to describe numerical data and used counts and percentages to describe categorical data. Categorical data were evaluated by the chi-square test and numerical data were estimated by a one-way ANOVA. Post-hoc tests were conducted using the Holm method, which was used to control for type I errors. Cohen’s d index was calculated as effect sizes, serving as standardized indicators unaffected by sample sizes. All tests were two-tailed, and a statistical difference was assumed when the p-value was <0.05. All statistical analyses were carried out through IBM SPSS Statistics 25.0.
Results
Demographic Characteristics
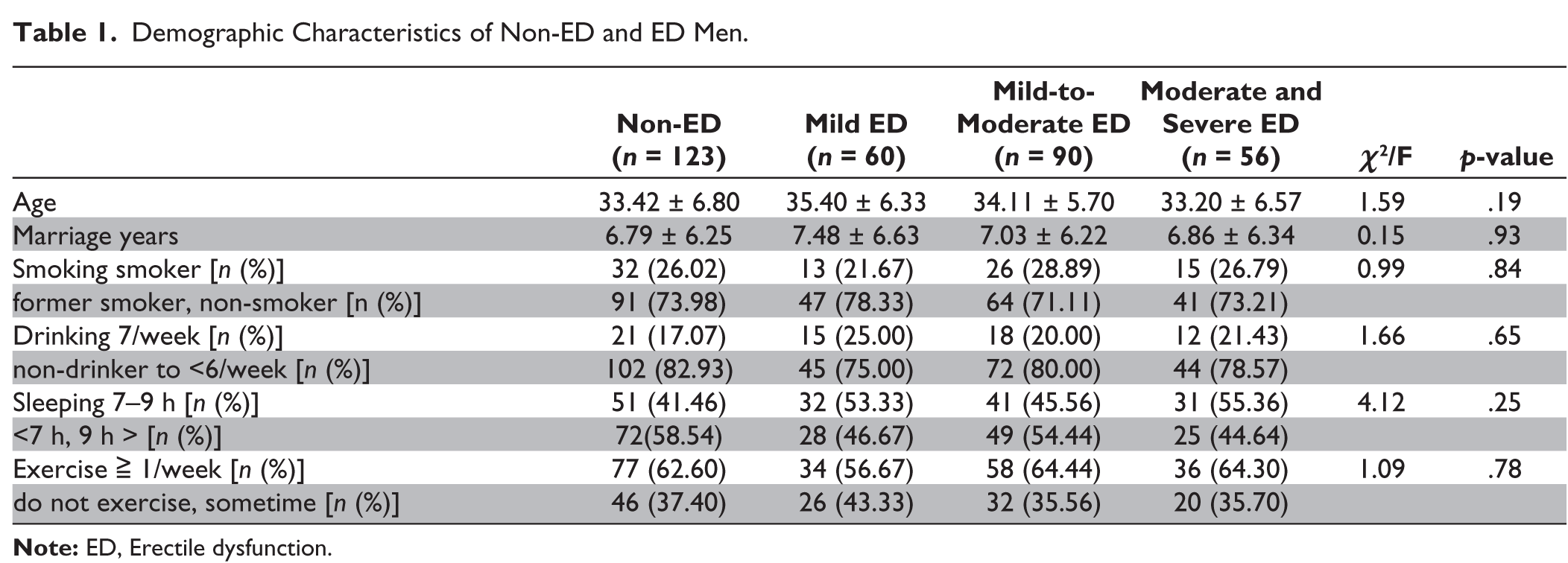
We obtained valid responses from 329 individuals (aged 33.93 ± 6.41 years). According to IIEF-5 scores, the distribution of severities of ED in men was as follows: non-ED, 37.39% (123/329); mild ED, 18.24% (60/329); mild to moderate ED, 27.36% (90/329); and moderate and severe ED, 17.02% (56/329). Table 1 shows the demographic characteristics of participants by erectile function groups. No statistical difference was found between non-ED and ED men in age, marriage years, or lifestyles.
Demographic Characteristics of Non-ED and ED Men.
IIEF-5, PHQ-9, and GAD-7 Results
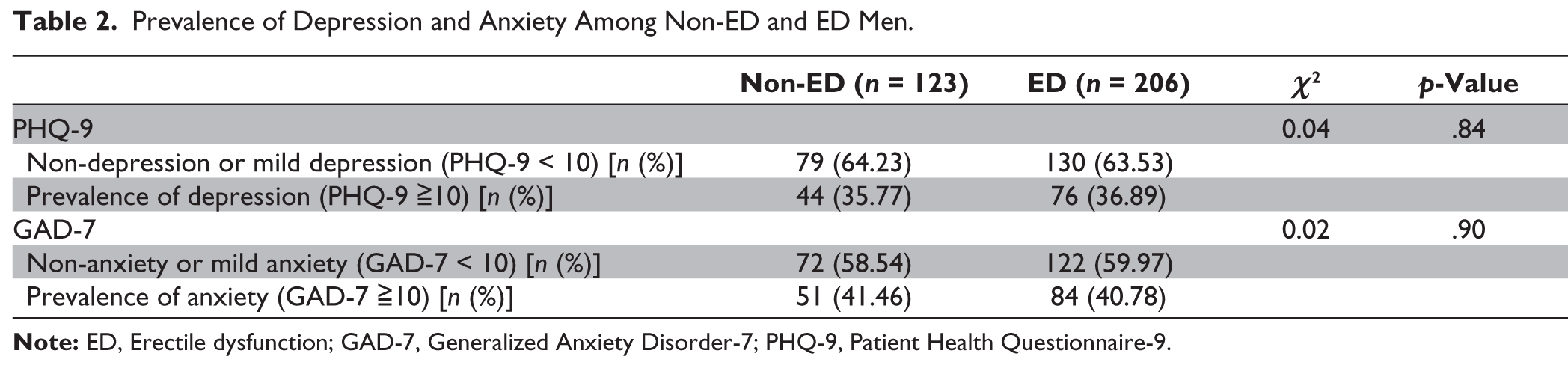
Table 2 shows the prevalence of depression using PHQ-9 ≥ 10 cut-off score among non-ED men was 35.77% (44/123) and among ED men was 36.90% (76/206). Also, the prevalence of anxiety using GAD-7 ≥ 10 cut-off score among non-ED men was 41.46% (51/123) and among ED men was 40.77% (84/206). There was no difference in the prevalence of depression and anxiety between non-ED and ED men (p = n.s.).
Prevalence of Depression and Anxiety Among Non-ED and ED Men.
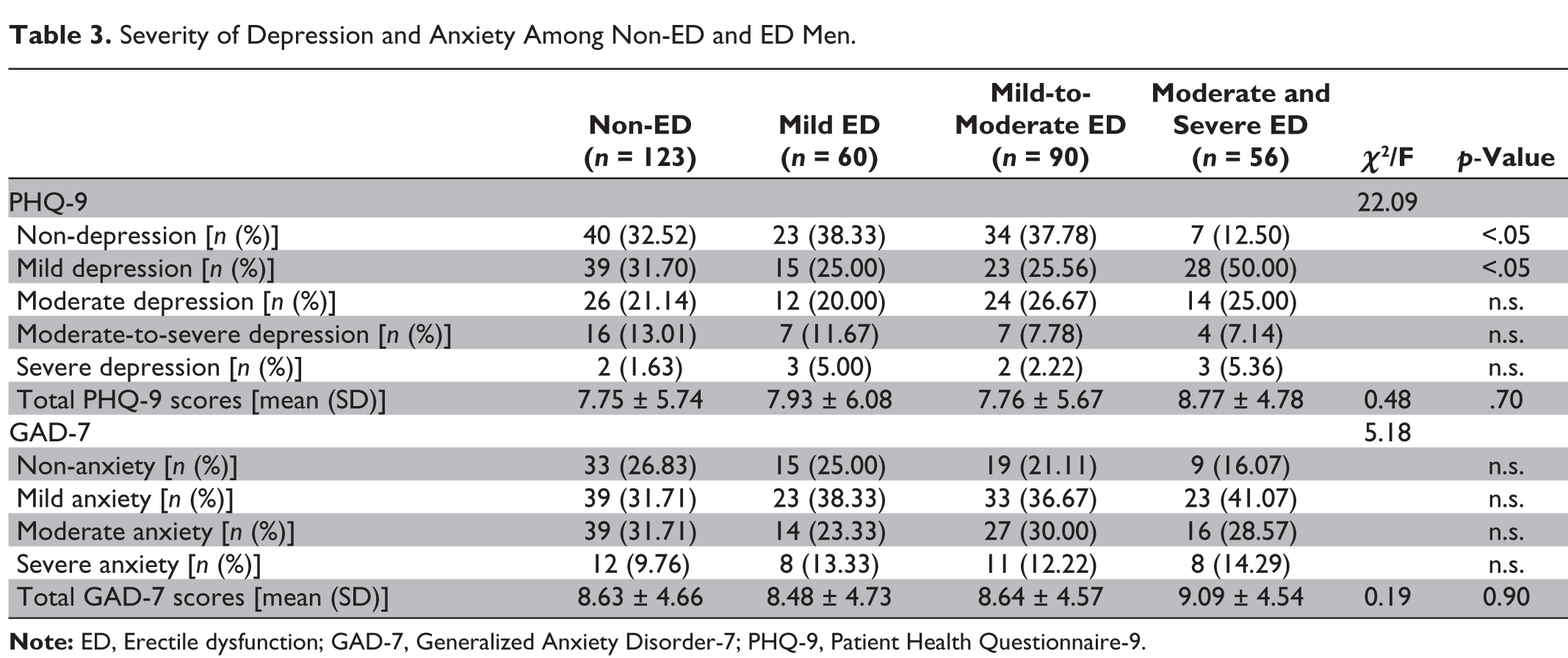
The mean scores of PHQ-9 by ED severity were as follows (Table 3): non-ED, 7.75 ± 5.74; mild ED, 7.93 ± 6.08; mild to moderate ED, 7.76 ± 5.67; and moderate and severe ED, 8.77 ± 4.78. Also, the mean scores of GAD-7 by ED severity were as follows: non-ED, 8.63 ± 4.66; mild ED, 8.48 ± 4.73; mild to moderate ED, 8.64 ± 4.57; and moderate and severe ED, 9.09 ± 4.54. There was no difference in mean scores of PHQ-9 and GAD-7 between non-ED and ED men (p = n.s.).
Severity of Depression and Anxiety Among Non-ED and ED Men.
IIEF-5 and LISAT-8 Results
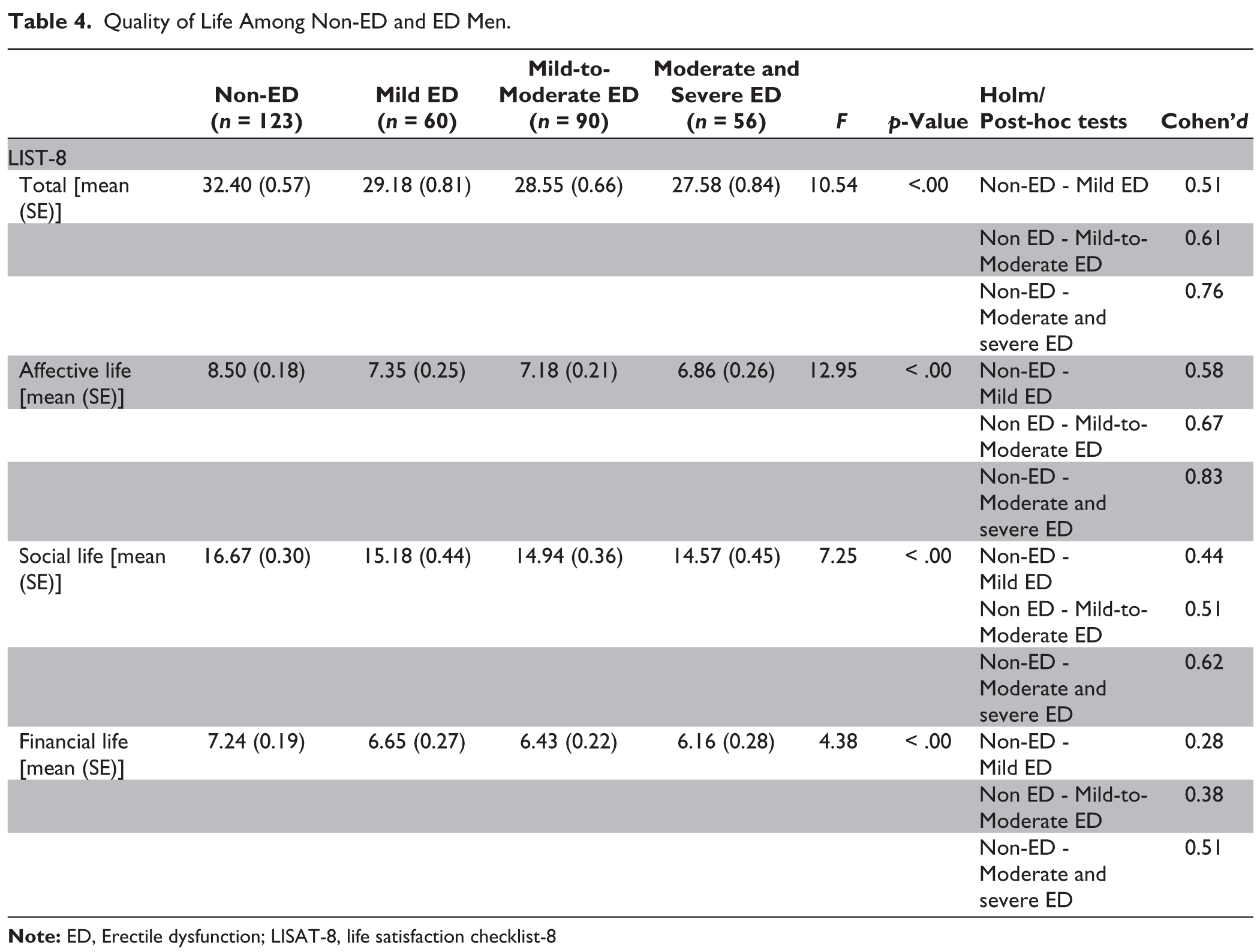
The mean total scores of LISAT-8 by ED severity were as follows: non-ED, 32.40 ± 6.79; mild ED, 29.18 ± 5.77; mild to moderate ED, 28.55 ± 6.75; and moderate and severe ED, 27.58 ± 4.97 (Table 4). ED men showed significantly lower total mean scores in LISAT-8 than non-ED men (p < .01). Also, ED men showed significantly less mean score of social life (items 1, 4–6), affective life (items 2 and 3), and satisfaction with financial life (items 7 and 8) than non-ED men, respectively (p < .01). However, there was no difference in the mean score of satisfaction with financial life (items 7 and 8) between non-ED and mild ED men (p = n.s., d = 0.28).
Quality of Life Among Non-ED and ED Men.
Discussion
This cross-sectional study aimed to evaluate depression, anxiety, and quality of life among young Japanese men. No statistical difference was found between non-ED and ED men with respect to demographic characteristics. Since organic diseases were excluded and the average age of the participants was 33.93 years, the population was assumed to have psychogenic ED. Contrary to expectations, however, there were no significant differences in depression and anxiety between non-ED and ED men. The mean PHQ-9 and GAD-7 scores among both non-ED and ED men were below the cut-off limit of §[ 10, corresponding to mild depression and mild anxiety), respectively. However, a significant difference was observed in LISAT-8 scores for life satisfaction between non-ED and ED men. Furthermore, significant differences were found not only in affective life but also in social life and financial life.
In a previous study, Yang et al. showed that in Chinese young men, the PHQ-9 and GAD-7 scores among non-ED men indicated no depression and no anxiety, respectively, while in the mild and mild-to-moderate ED subjects, the PHQ-9 and GAD-7 scores corresponded to mild depression and mild anxiety, respectively. 22 In addition, in moderate and severe ED subjects, the PHQ-9 and GAD-7 scores indicated moderate depression and moderate anxiety, respectively. The results of our study were not consistent with the previous study, which had found that depression and anxiety rose according to the severity of ED. This discrepancy, however, may be due to the online survey feature and self-assessment of symptoms employed in our study. Interestingly, while there was no difference in PHQ-9 and GAD-7 scores, there was a significant difference in LISAT-8 scores between non-ED and ED men. This included significant differences not only in affective life, but also in social life and financial life. A previous study had also found similar results. 21 We found no significant differences by severity of ED, although there was a tendency toward higher mean PHQ-9 score for depression in moderate and severe ED among the young Japanese men. This suggests that ED reduces the quality of life in various aspects.
Taken together, these results demonstrate that in addition to depression, it is necessary to focus on other psychosocial factors as well. For example, MaCabe suggest that treatment of sexual dysfunction should take into account the attitudes towards sex, their extent of performance anxiety, and the dynamics inherent in their personal relationships. 23 Men who experience erectile difficulties enter a sexual situation with high negative affect and low positive affect, along with negative expectations about their sexual performance.24,25 This mindset induces an attentional shift towards cues that signal failure and a strong evaluative focus on their own bodily signals, which distracts them from erotic cues. They react with spectating, self-monitoring, performance demands, and failure anxiety, which are frequently associated with an increase in sympathetic nervous system activity, leading to genital arousal inhibition. Eventually, some men will avoid sexual activity, thereby maintaining or worsening the initial negative affect associated with sex. Avoiding sexual activity exacerbates ED, and ED may have an obvious impact on the quality of life of the ED patient and his sex mate. 26 McCabe recommends the use of validated multidimensional measures that are designed specifically for men with ED (e.g., the SEAR questionnaire) when assessing psychosocial outcomes. 11 The SEAR questionnaire possesses strong psychometric properties that support its validity and reliability for measuring sexual relationship, confidence, and, particularly, self-esteem. 27 Various scales have been developed to measure psychosocial factors related to ED, but few are available in Japan. In the future, it will be necessary to develop a Japanese version of the scale to measure psychosocial factors related to ED.
The limitations of this study are as follows. As this study used a cross-sectional design, it has shown only “associations” and not “causality” between the quality of life and the ED. However, more experimentally controlled and prospective studies are needed to better understand how psychosocial factors are implicated in ED. Furthermore, factors such as the online survey nature of the study, self-report of ED symptoms, purposive sampling, the lack of a diagnostic interview, and sample size calculation may have affected the findings. Finally, the racial/ethnic and socioeconomic particularities of the subjects could limit the generalizability of the results. The study was also conducted during the COVID-19 epidemic, which may have influenced the results. In comparison to the previous studies, the present study showed higher levels of depression and anxiety among the non-ED men. Psychological distress indices have been significantly correlated with several measures relating to COVID-19 in Japan. 28
Conclusions
This cross-sectional study aimed to evaluate depression, anxiety, and quality of life among the young Japanese men. There were no significant differences in depression and anxiety between non-ED and ED men. On the other hand, there were significant differences in quality of life between non-ED and ED men. These results suggest that psychosocial factors other than depression and anxiety may also be the cause of ED in young Japanese men and that ED may reduce quality of life in various aspects. Partner relationships and performance anxiety are considered as important psychosocial factors. It is necessary to develop a Japanese version of the scale to measure psychosocial factors related to ED.
Footnotes
Declaration of Conflicting Interests
MG, CS, and HT are members of Logos Science Corp., Ltd.
Ethical Approval
This study was approved by the Waseda University Academic Research Ethical Review Committee (2019-363). The study protocol followed the guidelines for epidemiological studies in accordance with the Declaration of Helsinki.
Funding
This research was funded by Logos Science Corp., Ltd, Tokyo, Japan.
Informed Consent
The participant has consented to the submission of the article to the journal.