
Abstract
Background and Objectives:
WHO defines infertility as the ‘failure to achieve a pregnancy after 12 months or more of regular unprotected sexual intercourse’. Female sexual dysfunction (FSD) includes disorders centered on sexual desire, arousal, orgasm, and pain, which impair quality of life. Sexual Dysfunction impacts infertility as it results in decreased coital frequency, which can worsen infertility, adding to the distress of patients. The current study was a modest attempt to help detect and raise awareness about sexual dysfunction in patients and treating doctors, so that the necessary intervention can be provided, which ultimately improves treatment outcome and quality of life.
Methods:
This is a hospital-based, observational study. A total of 120 women between ages of 18 and 45 years attending the OPD Infertility clinic, at a tertiary care hospital over a period of 6 months from January 2024 to July 2024 were chosen for the study. Patients with current psychiatric illness, chronic debilitating medical illness, not engaging in sexual intercourse in the last 1 month or sexual dysfunction in a partner were excluded from the research.
Results:
The findings reveal that sexual dysfunction is prevalent among women facing infertility, with a slightly higher incidence in secondary infertility cases. Secondary infertile women had statistically significantly lower scores in arousal, orgasm and satisfaction domains than those with primary infertility.
Conclusion:
The high prevalence of sexual dysfunction both in primary and secondary infertility underscore the importance of incorporating sexual health assessments and psychosexual counseling into infertility treatment. Adopting a holistic approach, including psychological and relational dimensions of infertility care can improve both individual and couple outcomes and potentially fostering better sexual health.
Keywords
Introduction
The World Health Organization defines infertility as the ‘failure to achieve a pregnancy after 12 months or more of regular unprotected sexual intercourse’. When a pregnancy has never been achieved, it is termed primary infertility, and the failure to conceive after one prior pregnancy is termed secondary infertility. 1 In India, it is estimated that approximately 8% women suffer from infertility, among which 5.8% were secondary infertile. 2 The ability to reproduce is closely connected with self-image, self-respect, and sexuality. The spontaneity involved in sexual intercourse may be lost, as the main aim becomes conception. This may influence the ability for intimate sexuality and can give rise to sexual dysfunction. 3
Female sexual dysfunction (FSD) is a continuum of psychosexual disorders revolving around sexual desire with interrelated problems of sexual pain, arousal, and orgasm that impair the quality of life for many women. For some, it is a momentary problem, but for others, it is more debilitating. 4
Sexual discomfort is crucial in defining and diagnosing FSD. Distress can manifest as trouble, concern, sadness, irritation, rage, or hopelessness. Distressing behaviors may include decreased or absent initiation of sexual activity, avoidance of sexual circumstances, or involvement in sexual activity without desire. 5
Women’s sexual responses are complicated and incompletely understood. They have been reframed as a cyclical process influenced by societal and physiologic variables. 6 It is influenced by age, adverse effects of medications, sex hormone and psychological status. 7
Infertile women may experience impaired sexual function, which can negatively impact their physical and marital health and drastically decrease their quality of life. Researchers discovered that the number of people seeking medical attention for sexual complaints is far lower than the actual number of people experiencing sexual issues. 8
FSD is as common as male sexual dysfunction, but has received decreased attention in research. 9 It is difficult to determine if sexual dysfunction is the cause or result of infertility. Sexual dysfunction can lead to decreased coital frequency, which can worsen infertility owing to less exposure. Sex on demand can cause psychological stress and reduce the enjoyment of sex, thereby worsening sexual dysfunction. 10
Existing literature indicates that sexual dysfunction is more prevalent among infertile couples than among healthy controls. Despite sexual function being a crucial component of physical and marital well-being, it often receives inadequate attention, and as per our literature review, no research has evaluated the quality of sex in this population. 7
Our study aims to add data in the Indian setting about the impact of FSD on infertility. It will help in the detection and raise awareness about sexual dysfunction in patients and treating doctors, so that necessary and timely intervention can be provided, which ultimately improves the treatment and quality of life.
Materials and Methods
A cross-sectional hospital-based study enrolled 120 women with primary and secondary infertility, aged 18 to 45 years. Women engaging in a sexual relationship in the last 1 month, who could speak Kannada/English, and those willing to participate in the study were included. Women on treatment for any known psychiatric illness, sexual dysfunction in the partner, alcohol or other psychoactive substance abuse, or chronic debilitating medical illness, and those who had not had sexual intercourse in the last 01 month were excluded from the research.
Female Sexual Functioning Index (FSFI)
FSFI is a self-reported scale used for evaluating the elements of sexual function in females. It comprises 19 items assessing six domains of sexual function: desire, arousal, lubrication, orgasm, satisfaction, and pain. A score of 26.55 is used as an optimal cutoff for differentiating women with and without sexual dysfunction. The scale has been used in several earlier similar Indian studies, indicating its transcultural validity for use. The scale has an acceptable reliability coefficient (from 0.89 [satisfaction] to 0.96 [lubrication]). The test-retest reliability coefficients ranged from 0.75 (for pain) to 0.86 (for desire).
Sample Size Analysis
The sample size was calculated considering the prevalence of FSD in an earlier Indian study. 11 A sample size considering 12.6% expected prevalence, a precision of 6% and a confidence level of 95%, the minimum sample size required was 117, which was approximated to 120.
Data Analysis
Data was entered into a Microsoft Excel data sheet and was analyzed using the Statistical Package for the Social Sciences version 22 (SPSS 22) software. Categorical data was represented in the form of frequencies and proportions. Median values with interquartile ranges were used to describe continuous variables. Normality testing was conducted using the Shapiro-Wilk method. Group comparisons of Female Sexual Function Index (FSFI) scores between primary and secondary infertility was carried out using the Mann-Whitney U test, with Statistical significance is defined as P < .05.
Results
Table 1 describes the socio-demographic characteristics of 120 women with infertility. The majority of participants (54.2%) were aged 18–25 years, with a significant portion (30%) holding an intermediate or post-high school diploma. Employment status revealed that 40% were unemployed, while 16.7% held professional positions. Regarding socio-economic status, 48.3% were categorized as lower middle class. All participants were married, with 70.8% residing in urban areas. The study population was almost evenly split between primary (54.2%) and secondary (45.8%) infertility types.
Socio-demographic Characteristics of Women with Infertility (N = 120).
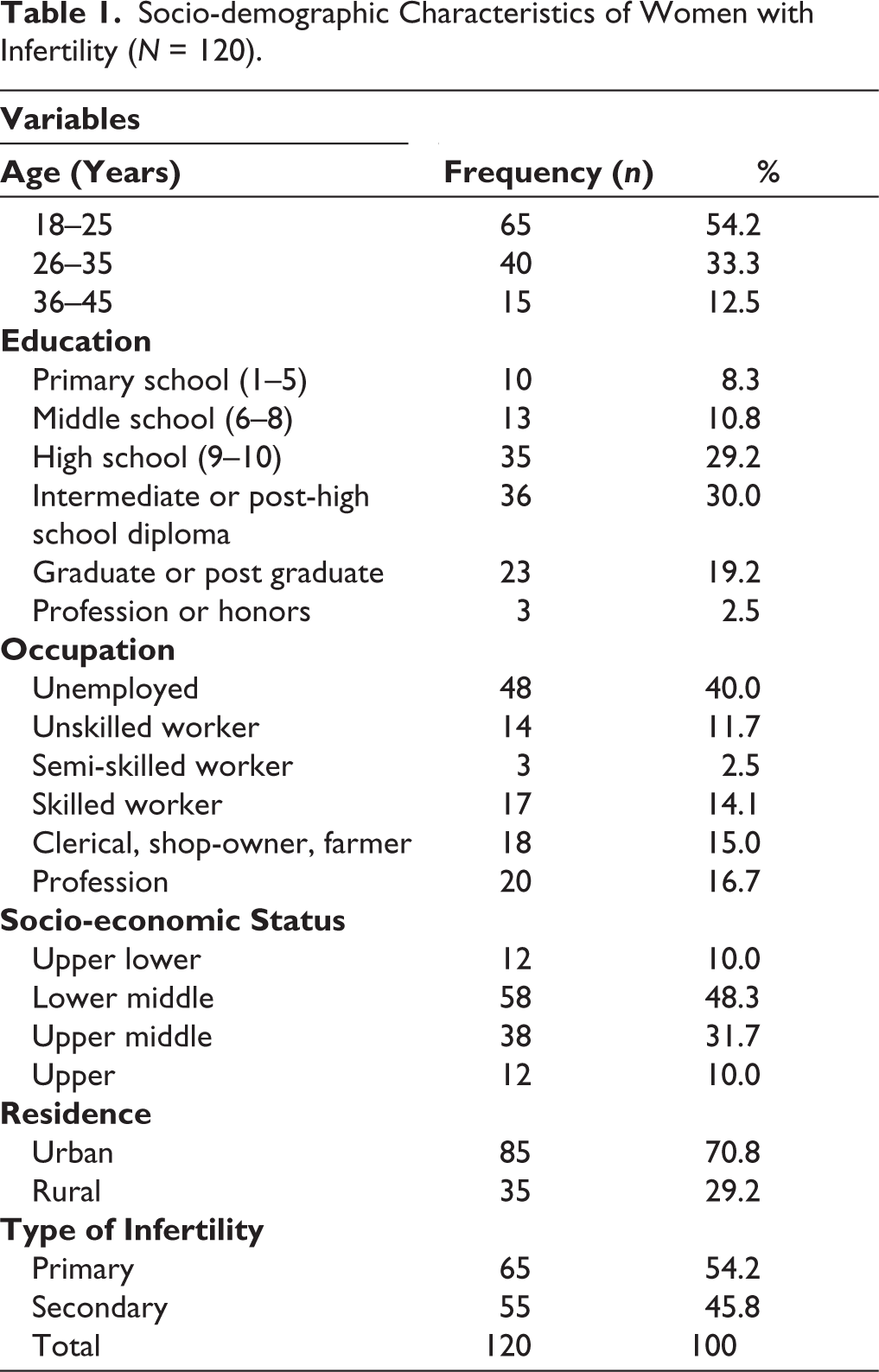
Table 2 presents the incidence of sexual dysfunction among women with primary and secondary infertility, involving a total of 120 participants. Among women with primary infertility, 40 out of 65 (61.5%) reported experiencing sexual dysfunction, while 25 (38.5%) did not. In contrast, 38 out of 55 women with secondary infertility (69.1%) reported sexual dysfunction, with 17 (30.9%) indicating no issues. These results suggest a relatively high prevalence of sexual dysfunction in both groups, with a slightly greater incidence among those with secondary infertility.
Incidence of Sexual Dysfunction Among Women with Primary and Secondary Infertility (N = 120).
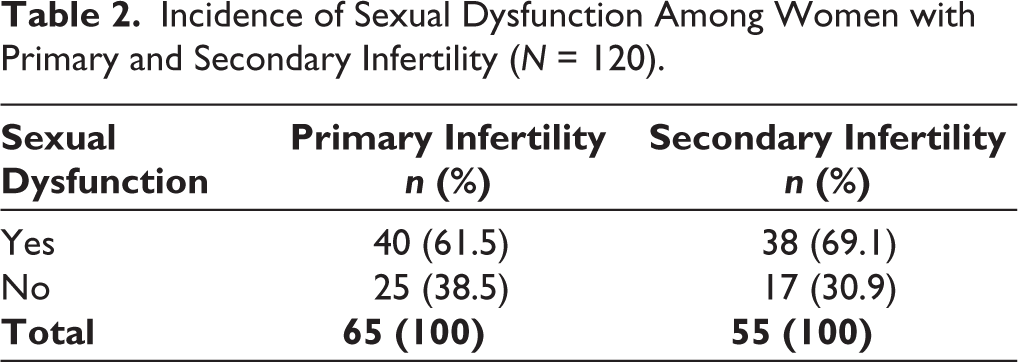
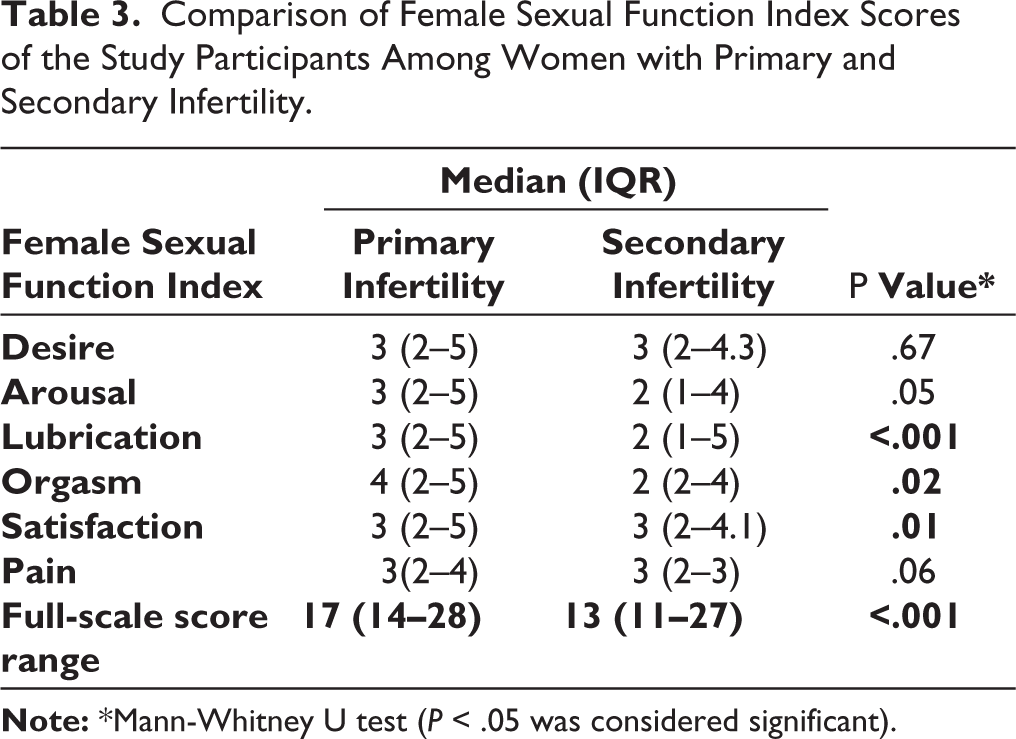
Table 3 compares the FSFI scores between women with primary and secondary infertility. For desire, the median (IQR) score was similar at 3 (2–5) for primary and 3 (2–4.3) for secondary (P = .67). However, significant differences emerged in arousal [(3 (2–5) for primary vs. 2 (1–4) for secondary, P = .05], lubrication [3 (2–5) vs. 2 (1–5), P < .001], and orgasm [4 (2–5) vs. 2 (2–4), P = .02], indicating better function in women with primary infertility. Satisfaction scores also showed a significant difference, with a median score of 3 (2–5) for primary and 3 (2–4.1) for secondary infertility (P = .01). Pain scores did not differ significantly [3 (2–4) vs. 3 (2–3), P = .06]. Overall, the full-scale median (IQR) FSFI score was significantly higher for women with primary infertility [17 (14–28)] compared to those with secondary infertility [13 (11–27), P < .001], suggesting a notable impact of infertility type on sexual function.
Comparison of Female Sexual Function Index Scores of the Study Participants Among Women with Primary and Secondary Infertility.
Discussion
This study compares sexual dysfunction prevalence and sexual function scores between women experiencing primary and secondary infertility. The findings reveal that it is prevalent among women facing infertility, with a slightly higher incidence in secondary infertility cases. Women with primary infertility scored higher across various domains of the FSFI.
Our findings of a substantial burden of sexual dysfunction in both primary and secondary infertility mirror existing literature. Rohina et al. demonstrated that nearly two-thirds of infertile women (63.67%; n = 170/267) had FSD, in contrast to less than half of fertile women (46.35%; n = 108/233). 12 Consistent with this, Keskin et al. reported a greater frequency of sexual dysfunction in secondary infertility (76.5%) relative to primary infertility (64.8%). 13
This pattern suggests that secondary infertility introduces additional psychological and social challenges, such as frustration and increased pressure stemming from prior successful pregnancies, which can impact physical aspects of sexual function.14,15 These experiences may contribute to feelings of inadequacy or guilt, potentially explaining the higher dysfunction rates in this group. 16
The differences in FSFI scores, particularly in domains like arousal and lubrication, provide further insights into the unique challenges faced by women with secondary infertility. The present findings align with Keskin et al., who reported significantly poorer arousal, orgasm, and sexual satisfaction among women with secondary infertility compared with primary infertility. 13
Rohina et al. similarly identified desire and orgasm as the most common sexual dysfunctions, each affecting 40% of participants. 12 In contrast, Onidi et al. found that desire and arousal were the most prevalent dysfunctions in both subfertile and fertile groups, while satisfaction was least affected. 17 Lower arousal and lubrication scores among women with secondary infertility may reflect stress linked to the expectation of difficulty conceiving again, creating a psychological strain that disrupts the physical responses necessary for satisfying sexual activity. 18 While women with primary infertility often experience stress related to the uncertainty of conception, secondary infertility brings a different kind of frustration due to repeated unsuccessful attempts despite previous success in conception. This frustration, combined with past pregnancy experiences, likely influences arousal and lubrication responses more profoundly than in those experiencing primary infertility. 19
Keskin et al. reported that depression and socio-economic status were key determinants of sexual dysfunction, with secondary infertility showing a substantially higher adjusted risk compared with primary infertility. 13 Sater et al. in a sample size of 157 found the depression rate to be 12.7%. Patients with depression had significantly lower FSFI scores. A total of 27.4% of patients experienced both depression and sexual dysfunction, showing a strong association. Poorer mental health was also linked to an increased risk of sexual dysfunction. 20 Olarinoye et al. found secondary infertility is linked with increased anxiety and depression, with studies showing rates of 39.6% for depression and 48.6% for anxiety among infertile women. 21 Addressing mental health needs among infertile women, particularly those with secondary infertility, is crucial, as unresolved psychological distress can greatly impair intimacy and satisfaction in sexual relationships. 22
Heidari et al. found that relationship dynamics play an integral role in sexual health, with mutual support, communication, and shared expectations acting as foundations for healthy intimacy. Infertility, however, often places considerable strain on relationships, leading to decreased intimacy and lower sexual satisfaction.23,24 Keskin et al. observed lower satisfaction scores among secondary infertile women, potentially reflecting additional relational stress within these partnerships. 13 Among women with secondary infertility, high dysfunction prevalence may also be linked to increased expectations or pressures to conceive, which can exacerbate relationship strain and lead to a cycle where stress further diminishes sexual interest.25,26
The cultural context of infertility must also be considered, as childbearing remains a primary expectation for women in many societies.27,28 These cultural and societal stressors can uniquely affect secondary infertile women, who may experience added judgment for not expanding their families. Culturally sensitive interventions that recognize and address these societal norms can enable healthcare providers to offer effective support, helping women navigate the cultural dimensions of infertility and its effects on sexual health.29,30
The results underscore the importance of incorporating sexual health assessments and psychosexual counseling into infertility treatment. Interventions focusing on stress reduction, relationship counseling, and sexual health education could play an important role in improving sexual function for infertile women. Adopting a holistic approach that includes psychological and relational dimensions of infertility care can improve both individual and couple outcomes, potentially strengthening relationships and fostering better sexual health. Targeted support for women with secondary infertility could address unique pressures, providing strategies to manage stress and enhance sexual well-being.
Conclusion
These results suggest a relatively high prevalence of sexual dysfunction in both groups, with a slightly greater incidence among those with secondary infertility, which underscores the importance of incorporating sexual health assessments and psychosexual counseling into infertility treatment.
Adopting a holistic approach that includes psychological and relational dimensions of infertility care can improve both individual and couple outcomes, potentially strengthening relationships and fostering better sexual health.
In some cases, proper management of FSD may help avoid costly and unnecessary infertility treatments, as it is important to determine whether sexual dysfunction is a cause or a consequence of infertility before initiating treatment. The findings of this study emphasize the need for comprehensive policies to assess and address sexual dysfunction across different causes of infertility, with the aim of improving sexual health and overall quality of life.
Limitations
Despite the relevance of the findings, this study has certain limitations. The relatively small sample size limits how widely the results can be applied. In addition, FSD has many contributing factors, and since the study was conducted in a hospital setting, the findings may not represent the general population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Ethics Committee approved the project (BGSGIMS/IEC/App/Jan/2024/007).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Consent was taken from participants.