
Abstract
Abstract
Background: Sexual dysfunction is common in females with schizophrenia and is attributed to multiple causes, including individual psychopathology and antipsychotics. Understanding the impact of relationship satisfaction on sexual functioning is not widely studied in schizophrenia. Women caregivers also experience sexual problems and were not studied in the past.
Aim: To assess the nature and occurrence of sexual dysfunction in women with schizophrenia in comparison to caregivers of males without severe mental disorder.
Methods: A cross-sectional study was conducted. A total of 30 women with schizophrenia were recruited as cases and 26 age-matched controls were recruited from female caregivers. All subjects were assessed using standardized tools such as Female Sexual Function Index (FSFI) and Relationship Assessment Scale along with sociodemographic questionnaire.
Results: There was a significant difference in FSFI scores and relationship scores between women with schizophrenia and caregiver control subjects. The relationship quality was better in patients with schizophrenia when compared to caregivers unlike sexual functioning.
Conclusion: Sexual functioning in women is a complex phenomenon. A holistic biopsychosocial approach is necessary to understand women’s sexual function.
Introduction
Sexual well-being is an important determinant of health and has a direct impact on one’s quality of life. Sexual response is a psychophysiological experience influenced by psychosexual development, psychological attitude toward sexuality, and attitudes toward one’s sexual partner. Sexual dysfunction is more common in patients with psychiatric illness as opposed to general population and is related to both the psychopathology and pharmacotherapy. 1 Sexual dysfunctions are frequently associated with mental disorders, such as depressive disorders, anxiety disorders, and schizophrenia. 2 Schizophrenia is an illness that affects interpersonal relationships and sexual function along with many other. The prevalence of sexual dysfunction in women with schizophrenia ranges from 30% to 80%. 3 The sexual dysfunction in people with schizophrenia is associated with poor quality of life and noncompliance to treatment. 4 The rate of female sexual dysfunction has been reported to be 64.3% in general population 5 and that of schizophrenia in women has been reported to be 70% in the Indian context. 6
A sexual disorder can be a symptomatic of biological problems, intrapsychic conflicts, interpersonal difficulties, cultural influences, or a combination of these factors. Sexual function can be affected by stress of any kind, by emotional disorders, and by a lack of sexual knowledge. Adequate sexual functioning is associated with personal well-being and relationship stability. 7 Research has shown significant association of sexual dysfunction with negative symptoms, general psychopathology, and antipsychotic medications in women with psychosis. 8 As illness and drug-related risk factors are specific to women with psychosis and the prevalence of sexual dysfunction is almost same in women with psychosis and general population in Indian setting, there is a need to explore the common risk factors. Most of the studies have concentrated on sexual dysfunction in women with psychosis in relation to individual psychopathology and pharmacology. 9 The role of relationship with spouse in causing sexual dysfunction in women with psychosis has not been studied in the past.
This study aimed to assess the nature, occurrence, and risk factors of sexual dysfunction in women with schizophrenia in comparison with women without mental illness using standardized assessment tools and to explore the association of sexual dysfunction with relationship satisfaction.
Materials and Methods
Setting and Study Design
A cross-sectional study was carried out at Department of Psychiatry in a tertiary care teaching hospital in south India. The psychiatric department caters 200 outpatients a day and has 40 beds in a patient ward.
Sample
The size of the sample was decided with a view to obtain as much of representativeness and precision of information as possible. A total of 30 individuals met the inclusion criteria and compared with 26 age-matched healthy controls.
Inclusion criteria for cases (n = 30) was as follows:
severe mental illness, married women aged 18 to 45 years, stable heterosexual relationship for last 1 year, and willingly gave written informed consent.
The exclusion criteria for cases were as follows:
severe language, hearing, or cognitive impairment, organic disorders including gynecological disease that affect sexuality, pregnant or breast-feeding within the last 1 year, postmenopausal women, and patients unable to participate due to severity of mental illness.
The inclusion criteria for controls (n = 26) were as follows:
no prior diagnosis of severe mental illness, married women aged 18 to 45 years, stable heterosexual relationship for last 1 year, and willingly gave written informed consent.
The exclusion criteria for controls were as follows:
severe language, hearing, or cognitive impairment, organic disorders including gynecological disease that affect sexuality, and pregnant or breast-feeding within the last 1 year, postmenopausal women.
Procedure
The study was conducted between June 2018 and September 2018. The study was approved by the Institutional Ethics Committee. All subjects who had met the inclusion criteria were included in the study. Controls were sourced from among the relatives of patients receiving treatment, that is, from the same socioeconomic and cultural population as the cases. The control subjects did not have a prior diagnosis of severe mental illness. The subjects were interviewed and assessed for sexual dysfunction and their relationship satisfaction.
Study Assessments
In sociodemographic questionnaire, all participants were asked to fill in semi-structured forms that had been prepared by the investigators. These forms included questions on age, literacy, residence, marital status, education level, occupation, income, and so on.
Sexual functioning was assessed using the Female Sexual Function Index 10 (FSFI), which is a 19-item, a self-rate instrument that assesses six key domains of sexual functioning in women. Each item is scored on a scale of 0 (or 1) to 5; a total score is also obtained, and higher scores indicate better sexual functioning. The FSFI domains are desire, arousal, lubrication, orgasm, satisfaction, and pain. Participants completed the FSFI alone, in a private room. Women who were not sufficiently literate to complete the FSFI on their own were assisted by multilingual female health professional. A total score below 26.55 denotes sexual dysfunction.
The Relationship Assessment Scale 11 (RAS) is a brief measure of global relationship satisfaction. It consists of seven items, each rated on a 5-point Likert scale. It is suitable for use with any individuals who are in an intimate relationship, such as married couples, cohabiting couples, engaged couples, or dating couples. The brevity of the scale increases its utility in clinical settings and for online administration. Research has shown the scale to be correlated with other measures of love, sexual attitudes, self-disclosure, commitment, and investment in a relationship.
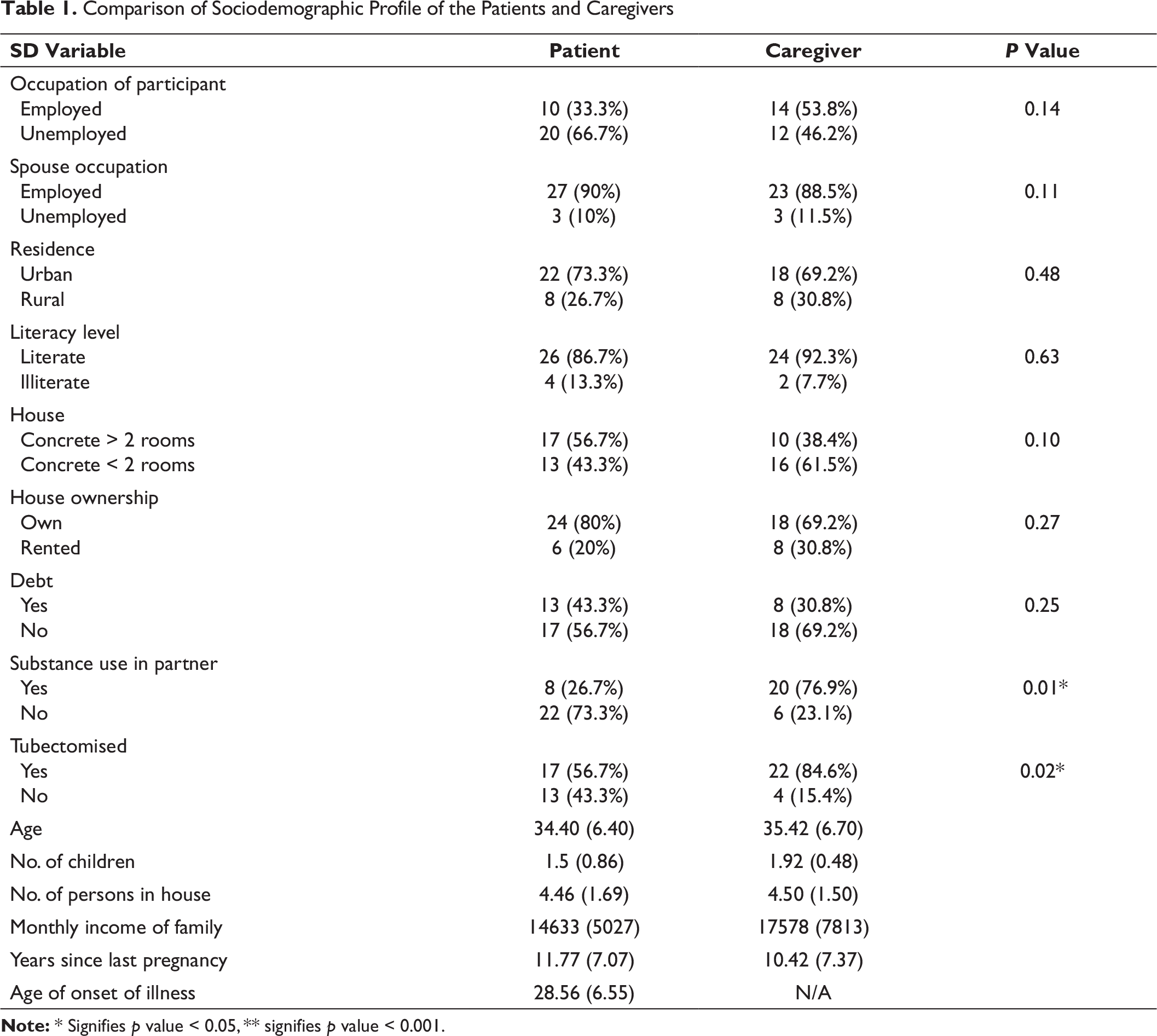
Comparison of Sociodemographic Profile of the Patients and Caregivers
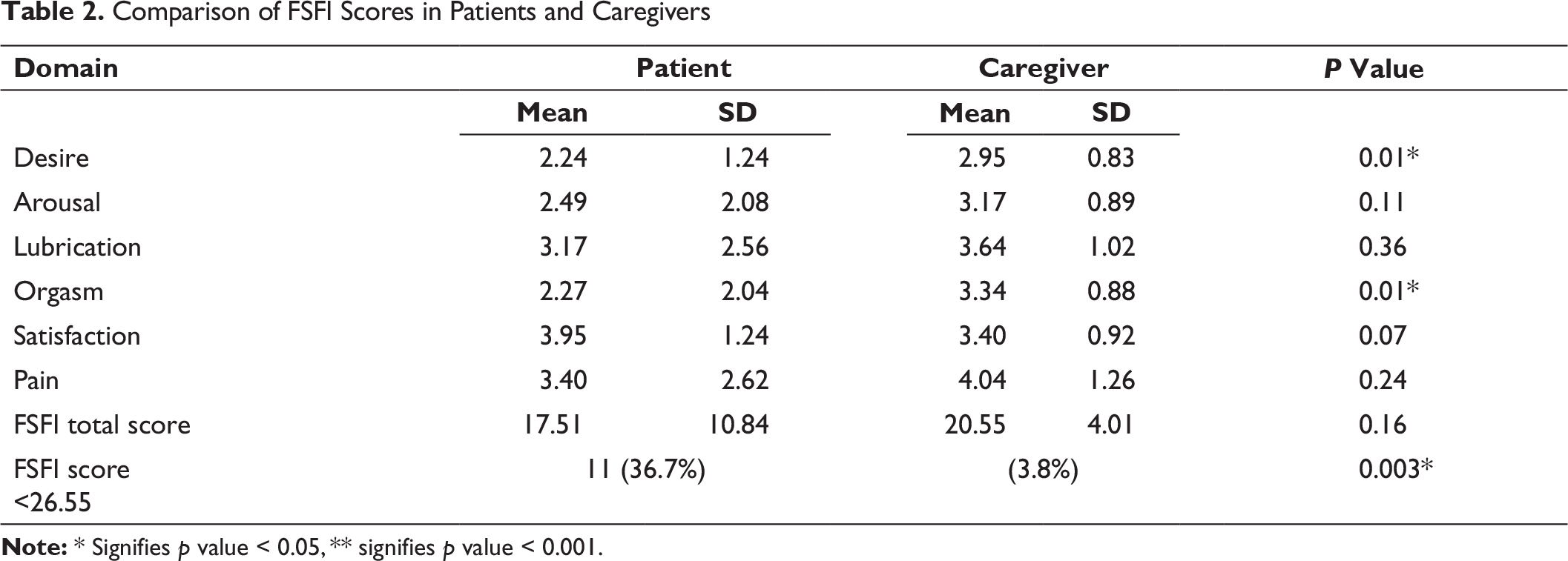
Comparison of FSFI Scores in Patients and Caregivers
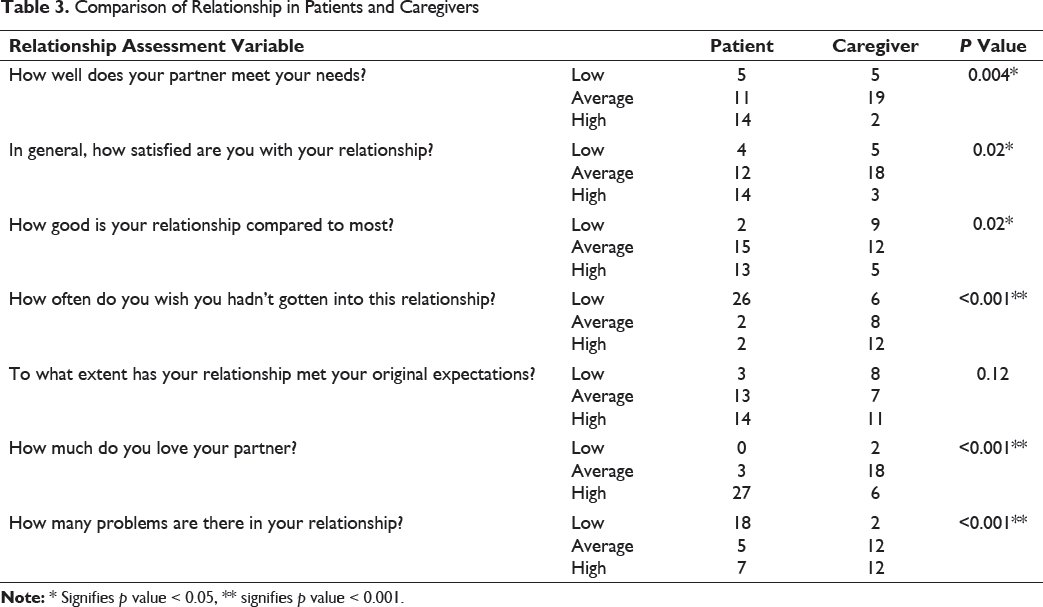
Comparison of Relationship in Patients and Caregivers
Results
Statistical analysis was done using computer software IBM SPSS (Statistical Package for Social Sciences) statistics for windows version 20 (IBM Corp., Armonk, NY, USA). The demographic and clinical data are presented in frequencies, mean, and standard deviation. An independent t-test was conducted to compare assessment scores of cases, and controls value was considered significant if values are less than or equal to 0.05.
Table 1 shows sociodemographic details of the subjects. There is no significant difference between sociodemographic details of patients and caregivers except that significantly more caregivers had been tubectomized. Table 2 shows the comparison of the FSFI domain and total scores of patients and caregivers. The patient group had lower mean scores on desire and orgasm compared to the caregiver group. Table 3 shows the comparison of relationship in subjects. Significantly greater number of patients compared to the caregivers, scored better on multiple domains of the relationship assessment scale, except to “what extent has your relationship met your original expectations.”
Discussion
The study was carried out in a tertiary care hospital in an urban area. The primary aim of the study is to assess the nature and occurrence of sexual dysfunction in women with schizophrenia and to find its relation with relationship satisfaction. It was a cross-sectional study with a control arm of women who were caregivers of males with diagnosis other than severe mental disorder. Our caregiver sample was chosen from spouses of males getting treatment for disorder other than severe mental disorder.
The occurrence of sexual dysfunction in women with schizophrenia is high when compared to healthy controls, similar to studies done in the past. However, the occurrence of sexual dysfunction in much higher than previous studies.12, 13 The mean age of the participants, both patients and caregivers, was about 34 to 35 years like previous studies done in Indian context. 6 More number of caregivers were employed as compared to patients. There was a high occurrence of substance use among the spouses of caregivers; however, this was because most of the caregivers were wives of individuals undergoing treatment for alcohol dependence. Among economic variables, most of the participants lived in their own house. The average monthly income was around Rs 14,600 among patients’ families and Rs 17,500 among the caregivers’ families. There was a higher occurrence of debt among the patients’ families. The average number of children was around 1 to 2 in both groups and the average time since last pregnancy was also more or less same in both groups, being around 10 to 11 years. However, it was observed that more number of caregivers had undergone sterilization procedure when compared to the patients.
The comparison of the FSFI domain and total scores shows that overall patients had greater sexual dysfunction compared to the caregivers. The disease burden experienced by the patients may be considered as one of the factors to which we can attribute the higher sexual dysfunction. Psychiatric disorders as well as the treatment involved may be associated with factors such as stigma, relationship difficulties, economic burden, disease-related morbidity, and treatment-related side effects. The lower FSFI in patient group could be attributed to psychopathology or antipsychotic agents. While lower than patients, the caregivers also, however, scored higher total scores on the FSFI scale and were not far better off. One of the factors attributable might be that most were spouses of alcohol-dependent patients undergoing detoxification/deaddiction and sexual problems are known to be prevalent in alcohol dependence syndrome. The other factor could be that caregivers could participate in sexual activity without the fear of becoming pregnant as majority of them had been tubectomized. Among individual domains, participants scored the lowest in desire and orgasm, revealing these to be the most impacted. Coincidentally, these were also the two domains in which the patients were significantly more affected as compared to the caregivers. Treatment with psychotropic medications many of which have sexual side effects can be considered as a possible contributing factor. The disease by itself may also predispose a person to experiencing lower sexual desire. At this juncture, however, gender-based differences in the sexual response cycle also need to be considered, where previous research has indicated that in women sexual desire sometimes or oftentimes may occur subsequent to arousal rather than antecedent.
The RAS measures revealed that more number of caregivers were unhappy or dissatisfied in their marital relationships as compared to the participants. The difference between the two groups was statistically significant for most items of the scale. More number of caregivers felt their needs were not met, were not satisfied in the relationship, had regrets about their relationship, and admitted to increased number of problems and experiencing less love for their partners. This could be possibly explained by lower expectations from their spouses because of lower self-esteem in patient group. 77% of spouses of caregiver group had alcohol dependence and probably, caregivers had higher expectations and were let down by spouses, so reported poor relationship scores. Despite this, the overall FSFI scores are better in caregivers. Whether this stands to implicate that the quality of the relationship has less bearing on the overall sexual functioning of the individual is food for thought.
This study has several limitations. The small sample size and hospital-based evaluation limit generalizability of the study. Choosing caregivers for comparison is strength in terms of understanding needs of caregiver and limitation as part of their marital dyad is not healthy thus effecting the results. We have not studied the effects of antipsychotic medication on sexual functioning, which could be potential confounder in our study.
Conclusion
The rates of sexual dysfunction are high in women with schizophrenia when compared to female caregivers. Multiple factors influence sexual functioning in women, including relationship satisfaction.