
Abstract
Objective:
This study aimed to explore the epidemiology and characteristics of primary versus secondary infertility cases referred to infertility clinics at a major Saudi Arabian referral hospital, as well as potential correlations between patients’ characteristics and infertility types.
Methods:
All female patients who visited the infertility clinics between January 2020 and December 2022 were included in this retrospective chart review study. Data were collected on medical histories, medications, diagnostic tests, reproductive characteristics, and the type and cause of infertility.
Results:
During the study period, a total of 667 female patients attended the infertility clinic. The mean age was 33.64 ± 6.56 years. The mean marriage duration was 79.92 ± 57.17 months, and the mean duration of infertility was 59.80 ± 49.71 months. Of the total patients, 56.07% had secondary infertility, whereas 43.93% had primary infertility. The most frequently defined causes were unexplained, followed by combined factors. Temporal patterns show a gradual, but significant decrease in cases during the COVID-19 pandemic peak months (25.82% reduction between January and April). Results from diagnostic tests were generally normal for most patients. Females with secondary infertility tended to be older (Mean age = 34.64 vs 32.37 years) and had been married for longer (Mean duration 96.18 vs 68.86 months; p-value < 0.001). The duration of infertility was longer for patients with primary infertility. An irregular menstrual cycle was more common in females with the primary type of infertility. Individuals with secondary infertility were significantly more likely to have had previous surgery.
Conclusion:
Crucial information in the epidemiology of infertility has been found. The older age among secondary infertility, as well as the high proportion of unknown causes warrants further research. Women’s health consultants and family physicians should initiate investigations and manage underlying causes during the waiting period for specialized clinic appointments.
Introduction
Infertility is a medical condition of the female and/or male reproductive system and is defined by the World Health Organization (WHO) as “the inability to conceive after more than a year of consistent, unprotected sexual activity.” 1 It can negatively impact people’s mental and psychosocial well-being by causing severe psychological distress, social stigma, depression, anxiety, violence, divorce, low self-esteem, and financial difficulty.1–5 According to a report released by the WHO, infertility is estimated to affect one in six individuals of reproductive age globally at some point in their lives. 2 The lifetime prevalence varied between countries; in middle-income and low-income countries, it was 16.5%, whereas in countries with high incomes, it was 17.8%. 2 Infertility services have been provided to 12.2% of females aged 15–49 in the United States. 6 Reports from Middle Eastern countries are as follows: Qatar showed that the prevalence of infertility was 16%. 3 Nearly one in six couples in the United Arab Emirates (UAE) had infertility, and the country’s general fertility rate has decreased from 2.7 births per female in 2000 to 1.5 births per female in 2020. 7 In Saudi Arabia, the General Authority for Statistics has reported that the fertility rate had decreased from 3.8 in 2011 to 2.7 in 2024 among Saudi females. 8
Infertility could be categorized as primary or secondary. Secondary infertility occurs when a person has at least one previous pregnancy, whereas primary infertility occurs when a person has never conceived. 1 Infertility can result from a variety of issues with the reproductive systems of either the male or female. Ovulatory dysfunction, obesity, ovarian reserve, uterine and tubal factors, and hormone-related illnesses are among the causes of infertility in females. Hormonal disorders, genetic abnormalities, and abnormal semen are common male factor infertility problems. The causes of infertility, however, are occasionally unclear. 6
The distribution of various reasons for infertility may vary from one country to the other due to differences in the characteristics of populations in different studies, for example, baseline incidence of sexually transmitted infections (STDs) or the ages of the populations under study. 1 At the primary level of healthcare, many of these reasons are manageable and preventable. 9 Particularly considering that access to infertility-related interventions is a challenging issue globally due to the deficiency in experts and the high cost of these interventions. 1
The WHO identifies high-quality family planning services, including fertility care, as fundamental to reproductive health. Given the significance of infertility and its effect on an individual’s well-being and quality of life, the WHO is dedicated to addressing infertility and fertility treatment by carrying out worldwide studies on the epidemiology of infertility. 1 Available studies from Middle Eastern countries, including Saudi Arabia, are limited. Therefore, the purpose of this study was to determine the epidemiology of infertility in terms of temporal trends as well as characteristics of primary versus secondary infertility cases referred to infertility clinics at a large referral hospital in Saudi Arabia, and to identify the possible associations between patients’ characteristics and types of infertility.
Methods
Ethical approval
The study was approved by Imam Abdulrahman Bin Faisal University’s Institutional Review Board Committee (IRB number: IRB-2022-01-444). Anonymity and confidentiality were ensured, and data was only utilized for the study. Written informed consent was waived as the data used did not contain any personally identifiable information.
Study design, setting, and population
This retrospective chart review study involved all females who visited the infertility clinics at King Fahd Hospital of the University (KFHU). KFHU is a large medical referral center in Khobar City that serves patients from the Eastern region of Saudi Arabia and is a teaching hospital of Imam Abdulrahman Bin Faisal University. An electronic record system is used to report hospital patient records. Laboratory, pharmacy, radiology, and doctor’s notes were all covered.
Medical record numbers of female patients referred to the specialized infertility clinics were obtained after approval. The sample consisted of a full coverage of all patients who presented to the clinic between January 2020 and December 2022. Records without a documented type of infertility were excluded.
Data collection tools and processes
Data on sociodemographic and reproductive factors, medical histories, prior surgeries, medication use, diagnostic test results, and the type and reason of infertility were collected using a checklist created by the investigators after evaluating related studies (Tables 1–4).7,10,11 Content validity was ensured by seeking the expertise of three experienced consultants in infertility, obstetrics and gynecology, and women’s health. Between January and October 2023, the patient’s electronic data system was used to collect data.
Sociodemographic and reproductive characteristics of females with infertility between 2020 and 2022.

Past medical and surgical history of females with infertility.

The five most reported medical histories.
The five most reported previous surgeries. The total ≠ 100% due to multiple responses.
The five most reported previous medications used. The total ≠ 100% due to multiple responses.
Clinical and laboratory-related characteristics of female patients with infertility.

Diagnostic interventions of female patients with infertility.

Statistical analysis
Patients with no documented type of infertility were excluded. All the remaining patients’ variables were managed and coded for analysis. Continuous variables were described as means ± standard deviation if normally distributed, and by median and interquartile range if skewed. Normality was assessed by the Shapiro–Wilk and Kolmogorov–Smirnov tests. Categorical variables were described as frequencies and percentages. The type of infertility was the comparative variable. p-values of associations were computed by t-tests for continuous variables and Chi-squares for categorical variables. For the skewed continuous variable, the Mann–Whitney nonparametric test was used for bivariate analysis. The missingness in data was challenging, and a decision was made to opt for complete case analysis for the separate bivariate associations to maximize the use of the available data. Levels of significance were set at p < 0.05. The Stata Statistical Software version 15.1 was used for data analysis.
Results
Temporal trend of patients with infertility
During the period from January 2020 to December 2022, a total of 667 records of females who visited the infertility clinic were reviewed (Figure 1). In 2020, a marked decline was observed between April and August, with visit proportions approaching zero. In contrast, 2021 and 2022 demonstrated more consistent distributions throughout the year, with peaks in June and December 2021, and October to December 2022. The highest percentage of visits occurred in January 2020, while the lowest was recorded during mid-2020 (25.82% reduction between January and April). A gradual increase in visit proportions was noted in the latter months of each year, particularly in 2022.
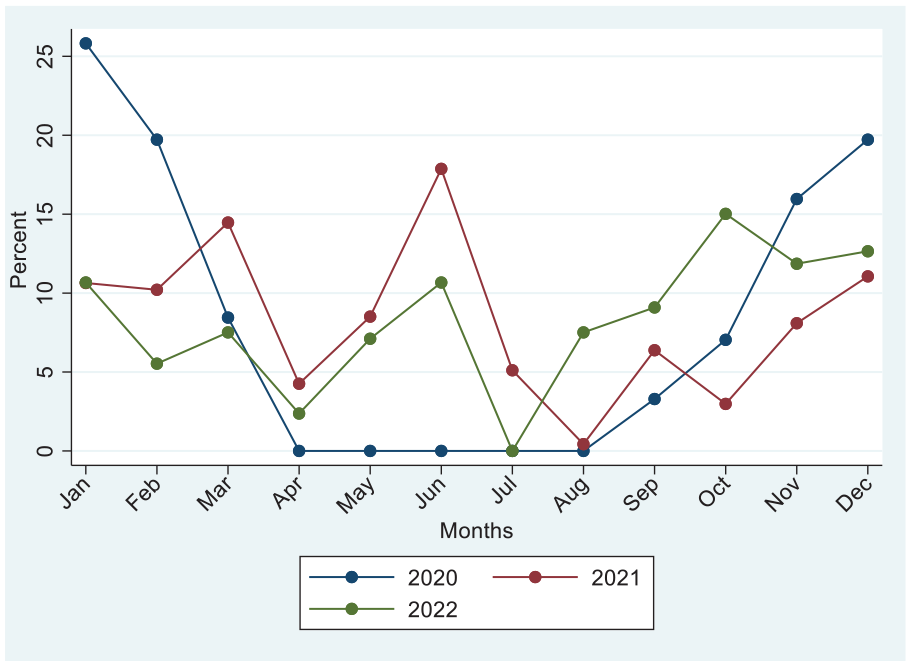
Epidemiological trend of infertility during 2020–2022.
Social and reproductive characteristics of females with infertility
Table 1 shows the available social and reproductive characteristics of these females. The mean age of females was 33.64 ± 6.56 years. The majority of patients were Saudi nationals.
With regard to reproductive characteristics, the mean length of marriage was 79.92 months, while the mean duration of infertility was 59.80 months. The pattern of the menstrual cycle was irregular in 26.91% of the total 524 females with a documented pattern. Most females were nulliparous (52.45%), and only 21.15% were multiparous. As for miscarriages, 56.44% reported no previous miscarriages, while 15.34% reported one previous miscarriage and 28.22% reported two or more miscarriages.
Past medical and surgical history of females with infertility
Table 2 presents the past medical and surgical history of females with infertility. Of the 667 females, 46.33% had a past medical history. Of those with a past medical history, the five most common conditions reported were polycystic ovary syndrome (PCOS; 19.20%), hypothyroidism (16%), Leiomyomas (10.67%), diabetes mellitus (9.60%), and hyperprolactinemia (8.27%). Almost 36% of females in the study reported previous surgeries and caesarean section was the most frequently reported surgery. One-third of patients reported medication consumption, the most common of which was folic acid in 54.38% of the 217 females who had reported use of medications.
Clinical and laboratory-related characteristics of infertility
Of the total 667 females in the study, 43.93% were documented to have primary infertility, whereas 56.07% had secondary infertility. About 60% of females did not have a documented cause for infertility. Unexplained causes were documented in 9.45% of cases, followed by combined factors (9.00%). The least documented causes of infertility are tubal factors (2.40%) and cervical factors in 0.15% of cases.
With regards to laboratory investigations, only 31 females have had a karyotype analysis (4.65%), 5 of whom have been found to have sex chromosome abnormalities. The medians of the follicle-stimulating hormone (FSH), the luteinizing hormone (LH), prolactin, and anti-Müllerian hormone (AMH) were 5.71, 4.36, 16.33, and 1.63, respectively (Table 3).
Diagnostic interventions for female patients with infertility
Table 4 presents the diagnostic investigations for patients with infertility. Out of the 667 patients, 253 (37.93%) have undergone a pelvic ultrasound. Of those, 53.36% had normal findings. PCOS features were found in 23.32%, compared to only 0.40% with cervical changes. Also, 286 patients (42.87%) had hysterosalpingography, of which 75.52% had normal findings in the fallopian tube, whereas a unilateral block of the left side was found in 9.09% compared to only 4.90% on the right side. Also, 87.76% had a normal uterine cavity appearance, whereas the most common finding was leiomyoma or polyps in the uterine cavity (5.94%).
Bivariate associations between patients’ clinical characteristics and type of infertility
Table 5 shows the bivariate associations between patients’ clinical characteristics and their type of infertility. The most frequently documented causes of secondary infertility were unexplained, followed by uterine abnormalities and combined factors. On the other hand, females with primary infertility were mostly due to combined factors, followed by ovulatory dysfunction and male factors (p < 0.001).
Bivariate associations between clinical characteristics of patients and their type of infertility.
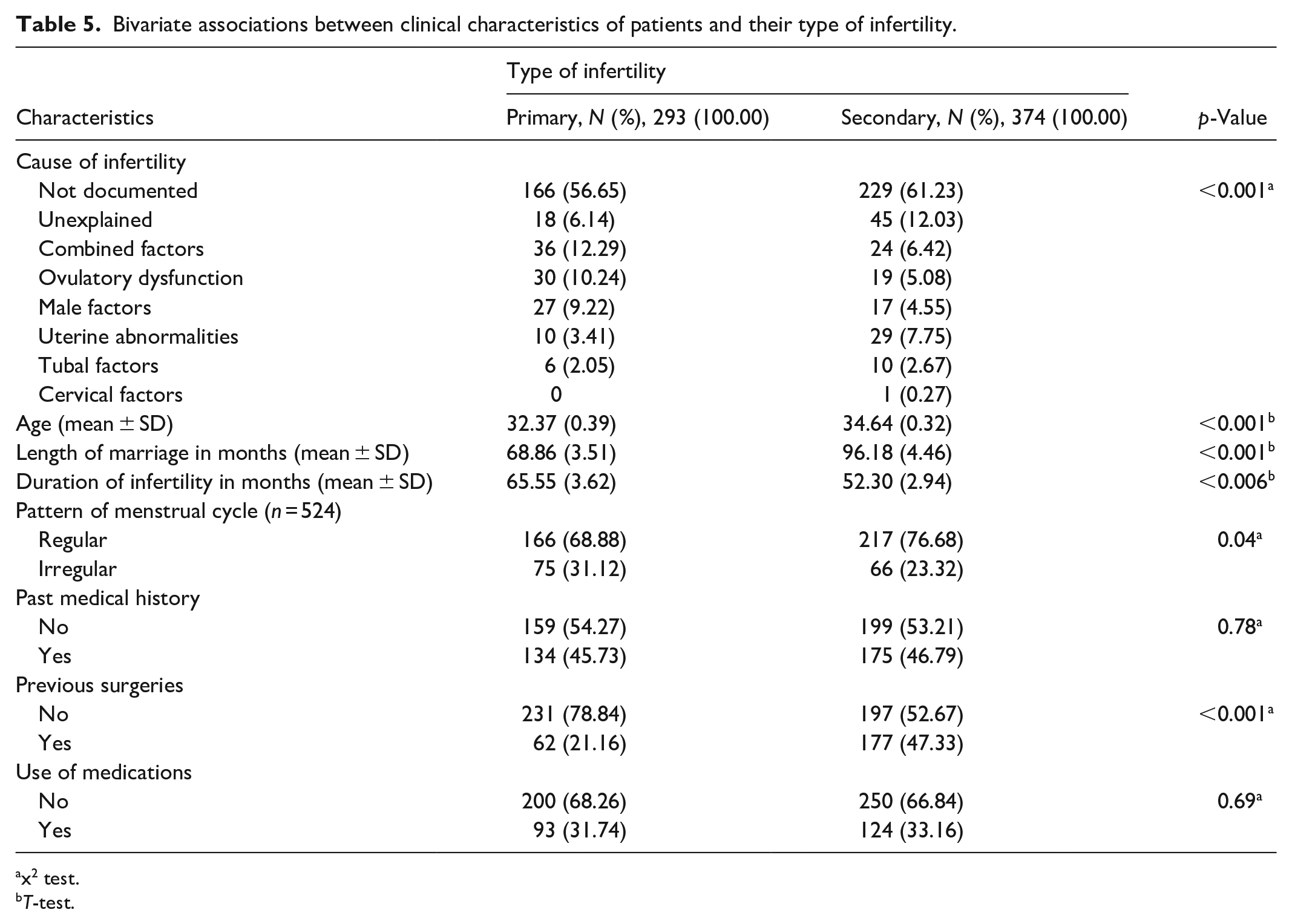
x2 test.
T-test.
The mean age was over 2 years higher among those with secondary infertility, and the mean length of marriage was similarly higher by over 27 months among patients with secondary infertility. These differences were also statistically significant (p < 0.001). The duration of infertility was statistically significantly higher in the primary infertility type.
An irregular pattern of menstrual cycle was reported in 31.12% of females with primary type of infertility and in 23.32% of females with secondary infertility (p < 0.04).
History of previous surgery was significantly more frequent among patients with secondary infertility than those with primary infertility (47.33% and 21.16%, respectively, p < 0.001).
Discussion
Worldwide, infertility is a significant health concern. The prevalence is rising globally, and it is imperative that more people have access to high-quality reproductive care. 2 Unfortunately, in the majority of countries, access to fertility care is still challenging, especially in countries with low or middle incomes. 1 Significant obstacles include a shortage of skilled workers, the required infrastructure and technology, and the very high costs of treatment medications. 1
Results from the present study showed that the average duration of infertility among female patients was about 5 years. Moreover, the duration of infertility was significantly higher among patients with the primary infertility type. Research showed that self-withdrawal from fertility care is common and that about one-fifth of individuals with infertility will wait 2 years or longer to be referred to an infertility specialist. 9 This highlighted the need for well-trained family physicians and staff at the primary care level to provide timely access to investigations, initial management, treat preventable causes, and address the emotional and social burdens of patients with infertility. 9
A notable decline in clinic attendance is observed during 2020, particularly between March and August, with near-zero visits from April to August. This sharp drop coincides with the peak months of the COVID-19 pandemic in Saudi Arabia, reflecting potential disruptions in healthcare access or patient avoidance of hospital visits as well as prioritization of urgent cases over non-urgent ones during this period. 12 In contrast, 2021 and 2022 show more fluctuant but sustained visit patterns throughout the year. Peaks in clinic attendance are observed in June and December 2021, and October–December 2022, suggesting a post-pandemic recovery in healthcare utilization. Notably, the seasonal variation in clinic attendance appears more pronounced in 2021 and 2022, while 2020 demonstrates a pandemic-induced flattening of typical visit patterns.
The results of this study showed that 56.07% of females had secondary infertility and 43.93% had primary infertility. A study from Oman demonstrated that secondary infertility was significantly more common than primary infertility (71.5% and 28.5%, respectively). 13 Similarly, in the UAE, the prevalence of secondary infertility was higher than that of primary infertility (62.5% and 37.5%, respectively). 7 The percentage of primary and secondary infertility in Africa is roughly equal. 14 A study among 178 infertile females undergoing assisted reproductive technology treatment in Namibia showed that 53.9% had primary infertility and 46.1% had secondary infertility. 15
Studies demonstrated that male and female factors, as well as unidentified or unexplained factors, are the causes of infertility. Up to 30% of infertility causes may be due to unexplained causes, whereas 35%–50% are caused by female factors, and 40%–50% are caused by male factors. 6 In the current study, about 60% of females with infertility had no documented etiology for their condition. Poor documentation or the fact that the patient is still being investigated, and no reason has been found, could be one explanation. Unknown causes were the most common among the causes of infertility that were documented, followed by a combination of factors. Further associations between types and causes of infertility in the current study demonstrated that the most commonly reported reasons for primary infertility were as follows: combined factors, ovulatory dysfunction, and male factors. On the other hand, females with secondary infertility mostly had unexplained causes, followed by uterine abnormalities and combined factors. A study among 928 patients in 2 fertility clinics in Abu Dhabi, UAE, showed that the most frequent cause of infertility in females was infertility of unknown etiology. Furthermore, the odds of primary infertility were higher in patients with uterine, ovulatory, or tubal factors than in those who had infertility for unexplained reasons. 7 A study conducted on 207 infertile couples aged 40 years or more who visited the infertility clinic in Oman revealed that the majority of infertility cases (54.1%) were caused by female factors, with male factors coming in second (22.7%). The frequency of infertility that could not be explained was 19.3%, and only 3.9% had combined factors. 13 Infertility in Africa is primarily caused by female-related factors, such as abortion, fallopian tube issues, and pelvic inflammatory diseases, followed by male-related factors. 14
According to research, the proportion of females with infertility rises with age and is lower among those aged 15–29. 6 In line with this finding, the average age of females presented to the infertility clinic in the current study was in the mid-30s. Furthermore, compared to individuals with primary infertility, those with secondary infertility were older. The ovulation function and reproductive span are significantly affected by increasing age. A delay in marriage is a rising trend in the Gulf Cooperation Council (GCC) countries; this may have an impact on childbearing and shorten the reproductive lifespan. Consequently, infertility in the GCC countries may be exacerbated by advanced maternal age. The mean age of infertile patients reported in the UAE is comparable to the observed mean age of the examined females. 7
Females with secondary infertility in the current study had a longer duration of marriage than those with primary infertility. Deshpande and Gupta concluded that infertility causes can be linked to the length of marriage. They found that male factors and unexplained infertility were more prevalent in couples who had been married for more than 5 years. One possible explanation for this is because as both couples age, the amount and quality of sperm and ova decrease. On the other hand, PCOS and tubal causes linked to STDs were more prevalent in couples who had been married for less than 5 years. 10
When evaluating a patient with infertility, the menstrual history is a crucial component of the history. 6 Infertility in females is significantly associated with irregular patterns of the menstrual cycle. 16 In the current study, one-quarter of the female participants had abnormal menstrual cycle patterns. In addition, females with primary infertility were more likely than those with secondary infertility to have an irregular menstrual cycle. In line with these results, an Indian study by Katole and Saoji 17 found a statistically significant correlation between primary infertility and irregular menstruation patterns.
According to the current study, the patients’ median levels of FSH, LH, prolactin, and AMH were 5.71, 4.36, 16.33, and 1.63, respectively. The residual ovarian reserve is reflected in AMH. Even when compared to FSH, which varies more from cycle to cycle, it is the best biochemical indicator of ovarian activity. Because AMH levels typically decrease with age, test results are age-specific. 9 The median AMH in a retrospective large-scale study involving 2495 Arabian Peninsula females, aged 19–50, with a median age of 34.81 years, was 1.76 ng/mL. 18
Most of the participants in this study who underwent radiological testing had normal findings. About one-quarter of patients who underwent ultrasonography reported findings related to PCOS. This can be explained by the current study’s finding that the most often reported medical condition was PCOS. A study among 100 females with infertility in Najran, Saudi Arabia, revealed that 56% of patients had PCOS features in the ultrasonography. 19 According to studies, 10% of females in the world who are of reproductive age have PCOS, making it a common reproductive endocrine disorder among females. 3 According to a recently published meta-analysis that included 2033 infertile females from studies across Saudi Arabia, Kuwait, Oman, and Qatar, 3 out of 10 of them had PCOS. Obesity and older age were associated with a higher frequency of PCOS. Compared to secondary infertility, primary infertility was correlated with a higher prevalence of PCOS. 20
Polyps or leiomyoma were the most often reported positive uterine cavity findings by hysterosalpingography investigation. This is in agreement with the fact that leiomyoma is the most frequent benign tumor in females. It can result in a number of symptoms, such as infertility, iron-deficiency anemia, menorrhagia, and persistent pelvic pain.21,22 In terms of fallopian tube results, hysterosalpingography revealed a unilateral block of the left side in 9.09% of patients who performed the tests and a unilateral block of the right side in 4.90%. This aligns with the current study’s findings, which show that tubal factors are recognized causes of infertility in a minority of patients. On the other hand, studies showed that one of the main causes of female infertility (between 25% and 35%) is occlusion of the fallopian tubes. According to analyses of hysterosalpingography reports of 266 infertile female patients in Lagos, Nigeria, tubal pathology was the most often found abnormality, occurring in 54.9% of cases. 23 The ability to pick up and transfer the egg or embryo may be impaired by tubal blockage or decreased tubal motility, which might result from certain disorders such as pelvic inflammatory diseases, endometriosis, STDs, and prior abdominal or pelvic surgeries. 6 The discrepancy in the frequency of tubal factors between the current study and others may be explained by the different epidemiology of these conditions around the world. 24
In the present study, patients with secondary infertility were significantly more likely to report a history of prior surgery, with cesarean section being the most frequently noted procedure. This finding may be explained by the role of cesarean delivery in the formation of postoperative pelvic adhesions, which can compromise fertility by disrupting the normal anatomy and function of reproductive organs. A recent Asia-Pacific expert panel consensus emphasized that adhesions resulting from gynecologic surgeries, including cesarean sections, represent a major clinical concern and may contribute to infertility, highlighting the need for effective adhesion prevention strategies in surgical practice. 25
The nature of the data in terms of the large amount of undocumented or missing observations presented a unique challenge during the analysis and is considered a major limitation. However, considering that the objective of the study was to draw patterns and assess associations and was not aimed at creating prediction models, this limitation has been alleviated within the context of this research. Every effort was made to account to minimize missing data, but this is an important issue that needs improvement. Moreover, no sample size calculation was done, as the sample consisted of full coverage of all patients who presented to the clinic during 2022. Additionally, certain characteristics, such as the number of marriages, sexual history, smoking, substance use, and the patient’s lifestyle, could not be evaluated from patient data. Also, due to the fact that the study only accessed female files, further research on the male partners’ side is suggested to draw a complete etiological classification. Furthermore, the results of this study may not be as generalizable because it was conducted in a single institution, which may have introduced selection bias. Despite all this, the uniqueness of the study spanning over 3 years using clinical data, especially in this region, gave strength to the study and provided baseline information in the field of epidemiology of infertility and women’s health.
Conclusion
This study highlights significant epidemiological patterns of infertility in Saudi Arabia and provides a foundation for targeted policy interventions. The predominance of secondary infertility, the high proportion of cases with unknown causes, and the extended duration before seeking care underscore the need for earlier engagement at the primary care level. To optimize the referral process, establishing standardized referral pathways and equipping family physicians, especially those who specialize in women’s health, with infertility assessment protocols and basic diagnostic tools—such as hormonal profiling and pelvic ultrasound—would enhance triaging efficiency. This could help initiate timely interventions and reduce the burden on tertiary infertility services.
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
The study was approved by Imam Abdulrahman Bin Faisal University’s Institutional Review Board Committee (IRB number: IRB-2022-01-444). Anonymity and confidentiality were ensured, and data will only be utilized for the study.
Consent to participate
Written informed consent was waived as the data used did not contain any personally identifiable information.
Consent for publication
Not applicable.
Author contributions
NAS and RSAlO contributed to the study’s conception. NAS, RSAlO, and NAT carried out the study design. RSAlO performed data analysis. NAS, RSAlO, and ASA contributed to material preparation and analysis interpretations. AHA, ARA, RSA, AAA, MGA, HRA, and AEA collected the data. All authors participated in the writing process and approved the final version of this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.