
Abstract
Background:
Dhat syndrome (DS) is a well-known culture-bound syndrome and is widely prevalent in rural areas and lower socioeconomic strata. Though mentioned widely in the mythology and modern medicine, DS has remained a controversial area in psychiatry with relation to its diagnostic validity and nosological status. With this background, this community-based study aimed to explore the epidemiological and clinical correlates as well as the comorbidities associated with this disorder.
Materials and Methods:
A total of 907 males between 18 and 60 years participated in the study through community-based sampling. Socio-demographics, socioeconomics, and physical parameters were recorded. “Tool to diagnose Dhat Syndrome (DS)” was prepared using the diagnostic criteria of DSM-IV and ICD-10. Those diagnosed with DS were further interviewed in detail for symptoms. All the study subjects with and without DS were studied for psychiatric disorders (MINI Plus) and any disorders related to sexuality, including the International Index of Erectile Function (IIEF) and the Premature Ejaculation Diagnostic Tool (PEDT). Sexual disorder assessment was done only for sexually active males above 18 years. The Statistical Package for the Social Sciences, version 16.0, was used for statistical analysis.
Results:
This is the first study globally to report the epidemiology of DS in the general population. Our study reports the prevalence of DS in the general population to be 12.5%. DS was more common in the 18–30 age group, particularly among individuals with low education, lower socioeconomic status, and job profiles in agriculture and daily wage work. The prevalence of psychiatric and sexual disorders is about threefold higher in those with DS compared to non-DS subjects. Twenty-five percent and 43% of patients with DS had comorbid depressive disorders and sexual dysfunction, respectively. Most of them attributed the loss of semen to the reason for DS. Backache, weakness, and easy fatiguability were the commonly reported physical symptoms, whereas loss of interest, decreased self-esteem, and guilt were the psychological complaints. The majority perceived thinness of semen, decreased sexual capabilities, and size of testes, as well as tilting of genitals, as a part of the DS.
Conclusion:
DS, irrespective of its controversial position in the classificatory systems, is a highly prevalent and distressing disorder with multiple comorbidities. Population-based studies such as this help to understand the attributions, risks, and clinical characteristics of patients with this intriguing disorder that can provide useful insights for management.
Dhat Syndrome (DS) is a common culture-bound syndrome in males with controversial nosology, attributed to ‘loss of semen’ from the body. A community-based study was conducted to assess the epidemiology, comorbidities, and clinical correlates of DS in Southern India. Prevalence was high (12.5%) with poorly educated young males from rural areas and lower socioeconomic status being mainly affected. Comorbid depression and sexual dysfunction were high in those with DS. Individuals with DS attributed their physical and psychological symptoms to the loss of “semen” and perceived a change in the morphology and vitality of their sex organs. The findings are discussed in the Indian sociocultural context and in light of global literature on DS.Key Messages
Introduction
The term “dhat” is mainly derived from the Sanskrit word “dhatu,” which means “metal,” a “medicinal constituent” that is considered to be “the most concentrated, perfect and powerful bodily substance, and its preservation guarantees health and longevity.” 1 The disorder related to this “dhatu” is mentioned in the ancient treatments “Sushruta Samhita” in Sanskrit, also called “Shukrameha” (shukra = sperm; and meha = passage in urine). 2 Traditionally, the loss of “dhatu” has been associated with weakness and vitality in the Charaka Samhita and considered by Aristotle as a “soul substance” that can lead to imbalance of bodily humors.2,3 “Dhat syndrome” (DS), a well-known “culture-bound syndrome” characterized by physical and psychosexual symptoms such as weakness, tiredness, anxiety, appetite loss, and guilt associated with loss of semen through nocturnal emission, in urine, and by masturbation, as mentioned in earlier reports.1,3 The term “culture-bound syndrome” was formally introduced by a Chinese psychiatrist more than five decades ago.4–7 Several past studies have emphasized the prevalence of this culture-bound syndrome worldwide.8–16 Recent research in India reveals that DS comprises a plethora of anxiety, depression, and somatic complaints specifically attributed to semen loss.17–22
In an epidemiological perspective, a greater prevalence of DS has been reported in India, Pakistan, Nepal, and Bangladesh.23,24 Syndromes similar to DS are prevalent worldwide, too. A similar kind of syndrome is observed to be present in other cultures by different names, such as “shen-k-uei” in China, 25 “prameha” in Sri Lanka, 26 “jiryan” in different parts of South East Asia.27,28 The series of events of DS is often traced back to Vedic culture, where it was addressed to maintain Brahmacharya, in which an individual must ration semen, and it is the semen that provides solidarity to a person to succeed into God Brahma. 29 The beliefs regarding the preciousness of semen are not limited to the Hindu religion’s culture; similar cultural beliefs exist in religions such as Islam, Christianity, and Buddhism. 30 This has probably led to a popular “food-blood-semen” association with a culturally sanctioned belief that failure to preserve semen can lead to sexual dysfunction, impotency, and loss of masculinity as well as vigor. 8
To understand the genesis of DS, it is important to appreciate the impact of culture, demographic profiles, and the socioeconomic variables of the affected individuals. Culture comprises values and different behavior patterns as well as ideas, which are considered in the context of historical backgrounds. It also consists of beliefs, values, norms, and myths, which are the components of specific geographic areas and are also shared and discussed by people in those particular areas. 24 According to Tiwari et al. 25 “culture is a ground substance, in which psychological, sociological, and biological forces operate, and influence the mental processes as well.” Cultural influences affect the mode of communication in individuals, and these interactional patterns are considered important in diagnosing mental illness, particularly when and where objective tools are not available. 26 Cultural context has been emphasized by the mental health professionals who have attempted to differentiate between the essential pathogenic determinants of a mental disorder from the individual and cultural variations.27–29 Beside these, the patients of DS usually believe that semen loss is harmful, and that it leads to multiple problems. Nocturnal emission and masturbation are considered to be the commonest forms of semen loss. Perceived causes of nocturnal emissions were bad company, increased interest in sex, sexual thoughts, and exposure to pornographic material, based on demographic and socioeconomic profiles.13,17,31 These attributional patterns and culturally sanctioned belief systems related to DS have been fundamental to the genesis of its symptoms and the reason for help-seeking. High prevalence was found in young men, unmarried or newly married men of rural areas with low or medium socioeconomic status and lower literacy status compared to urban areas.21,31–33 Few studies revealed that DS was also observed in urban areas with a high prevalence among young men, but with lower rates of education and employment.34,35 DS is also a common disorder in clinical practice, often presenting to psychiatrists later in the course. Mostly treated by traditional healers and alternative systems of medicine, the multi-dimensional presentations of DS can shadow a lot of other conditions, such as depression, anxiety, delusional disorders, sexual dysfunction, impotency, and infections such as urinary-tract infections and sexually transmitted diseases.17,36 It has also been reported in a recent study by Shahi et.al, that the quality of life (QoL) in DS patients is lower and it is mostly attributed to the comorbidities associated with DS. 16 Hence, understanding this common mental health problem that can be chronic, having a significant effect on the QoL, becomes important in its treatment.
Keeping this in the background, the present community-based study attempted to explore the prevalence rates, symptom profile, comorbidity, and management of DS in rural men of Suttur village in Karnataka. This study was conducted as part of the PhD. thesis submitted by the first author to the JSS University, Mysore. 37
Materials and Methods
Study Design
The study was conducted in Suttur village in Karnataka. There is a primary health center run by the Government of Karnataka in collaboration with the JSS Medical College and Hospital. The study was designed to interview males above 18 years in the entire community area to know the prevalence of DS. The research work was carried out within a mixed population of rural and semi-urban areas through community-based, door-to-door sampling from January 2012 to January 2015. Appropriate written informed consent was obtained from the participants. The study was approved by the Institutional Ethics Board of JSS Medical College, JSS Academy of Higher Education and Research, Mysuru, Karnataka.
Type of Study
A descriptive and exploratory study and a door-to-door epidemiological study were carried out.
Hospital-based population presenting with DS.
Inclusion Criteria
All males age of >18 and <60 years.
Those who gave informed consent.
Exclusion Criteria
All males <18 and >60 years.
Individuals with psychotic symptoms, intellectual disability or dementia, other organic disorders, or those who refused to provide informed consent were excluded.
Data Collection
Out of 1,100 male subjects who had fulfilled the inclusion and exclusion criteria, 907 subjects gave informed consent to participate in the study. The visits to the study area were done twice for interviewing the subjects. For clinical data, weight, height, pallor, and blood pressure were measured to inform basic health tips regarding obesity, the importance of diet, and to refer to a physician if blood pressure was above normal. Privacy and anonymity were ensured during the study. “Tool to diagnose DS” was prepared for the study to diagnose the presence of DS. This tool was based on the diagnostic criteria given in ICD-10 and DSM-IV TR.38,39 Those subjects who were found to have DS were further interviewed. The symptoms subjects attribute to semen loss were noted using the “Tool to assess Symptoms of DS.” All the subjects with DS and without DS were assessed for psychiatric and sexual disorders to understand the variation in the prevalence of psychiatric and sexual disorders among those subjects with a diagnosis of DS and those without. Sociodemographic data were collected as per the prepared standard questionnaire. No psychiatric disorder screening questionnaires were used to avoid false positive and false negative findings, and each patient was interviewed in detail using MINI- Plus for diagnosing psychiatric disorders. 40 Male sexual disorder assessment was done using the International Index of Erectile Function (IIEF) 41 and Premature Ejaculation Diagnostic Tool (PEDT). 42 Structured questionnaires were prepared for the study to assess hypoactive sexual desire disorder, sexual aversion disorder, post coital dysphoria, anorgasmia, dyspareunia, paraphilia, and gender identity disorders based on ICD-10 and DSM-IV TR diagnostic criteria. All the parameters of assessment were the same except for the socioeconomic scale. 35 The socioeconomic variables, such as age, marital status, education, occupation, family structure, religion, chronic medical condition, alcohol, and nicotine consumption assessment, were studied based on Modified B. G. Prasad’s classification. 43
Statistical Analysis
All the statistical analyses were performed using the Statistical Package for the Social Sciences software (version 16.0). The descriptive analyses were done using mean and standard deviation for continuous variables and percentage frequency for nominal variables. Pearson’s chi-square test was performed to compare categorical variables. Contingency coefficient, or crosstabs or two-way variables test, was done to determine the relationship between several categorical variables. The combined studies were done among the rural and urban subjects for prevalence rate, common symptoms, and comorbid psychiatric and sexual disorders of DS.
Results
In this door-to-door epidemiological study, a total of 907 subjects who had given informed consent were assessed and interviewed. The study results of demographic and socioeconomic status are described. Among 907 subjects, only 113 individuals were diagnosed with DS. The comorbid psychiatric and sexual disorders in patients of DS and their clinical presentations are described below under physical, psychological, and sexual symptomatology.
Demographic and Socioeconomic Status of the Study Subjects
A total of 907 subjects were included in the study who fulfilled the inclusion and exclusion criteria. The study population consisted majority of subjects from 18 to 30 years (44.5%), followed by those aged 31 to 40 years (24.3%), 41 to 50 years (18.70%), and 51 to 60 years (12.5%) (Figure 1c). Among the study subjects, 45.80% were illiterate, followed by 25.20% of those with a high school education, 19.70% who had completed an undergraduate or graduation, and the least number of subjects were postgraduates (0.60%). The majority of the subjects were married and were in agriculture (63.30%), while 36.70% were unmarried. Most subjects (61.30%) were residing in a nuclear family, followed by 38.40% in a joint family, and only 0.30% of the study population were residing alone. In case of addictive behaviors, subjects without smoking and non-alcoholic groups (84%) as well as smoking and alcoholic groups (16%) were found to have almost similar prevalence of DS. The occupational distribution revealed that the majority of subjects were engaged in agriculture (43.40%), followed by daily wage labor (28.00%), salaried or business (20.00%), and students (7.90%), but only a few were unemployed (0.70%). In terms of socioeconomic status, upper and lower classes each represented only 3.3% of the study population, and the majority of the study subjects were from the lower middle class and upper lower class based on the Prasad classificatory system (mentioned before). It was observed from the study that most of the subjects had no medical comorbidities (93.70%), while a few of them had diabetes mellitus (2.50%), hypertension (2.40%), chronic obstructive pulmonary disease (0.90%), asthma (0.30%), and migraine (0.10%).
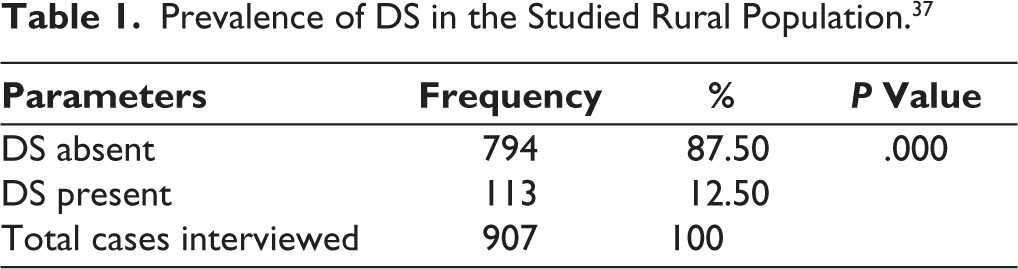
Of the 907 subjects, 113 were found to have DS. The prevalence of DS was found to be 12.5% in the study population (125 per 1000 population). P value was observed as highly significant (P = .000) for the distribution of DS in the study subjects (Table 1).
Prevalence of DS in the Studied Rural Population. 37
Subjects with DS Across Various Demographic and Socioeconomic Variables
Table 2 describes the age distribution among subjects with DS at a significant level of P = .000, and it was observed to be highly prevalent among those between 18 and 30 years and was found to decline with increasing age, with the least prevalence among those between 51 and 60 years. DS was found to be prevalent in both educated and non-educated population groups without significant changes (P = .103). Subjects with a high school education level formed most cases (31%), and they were closely followed by the subjects with no education (29.2%). DS was also found to be prevalent in subjects educated beyond the level of undergraduate or graduate studies. The population consisted of almost two-thirds of married and one-third of the unmarried population. After assessment for DS, 31.5% cases of DS were found among married individuals and 68.10% among unmarried individuals. So even though the initial study population had a higher number of married people, diagnosed DS cases were found in more than two-thirds of the study population with a statistically significant difference (P = .000). This reflects that DS is highly prevalent among people who are not yet married. About 60% of the DS cases were found in those residing in a nuclear family, with a significant change (P = .030). Forty percent of the cases were in those from joint families. DS was not found in those living alone, but it must be considered that the study participants who were living alone were quite few.
Demographic Variables of the Study Population. 37
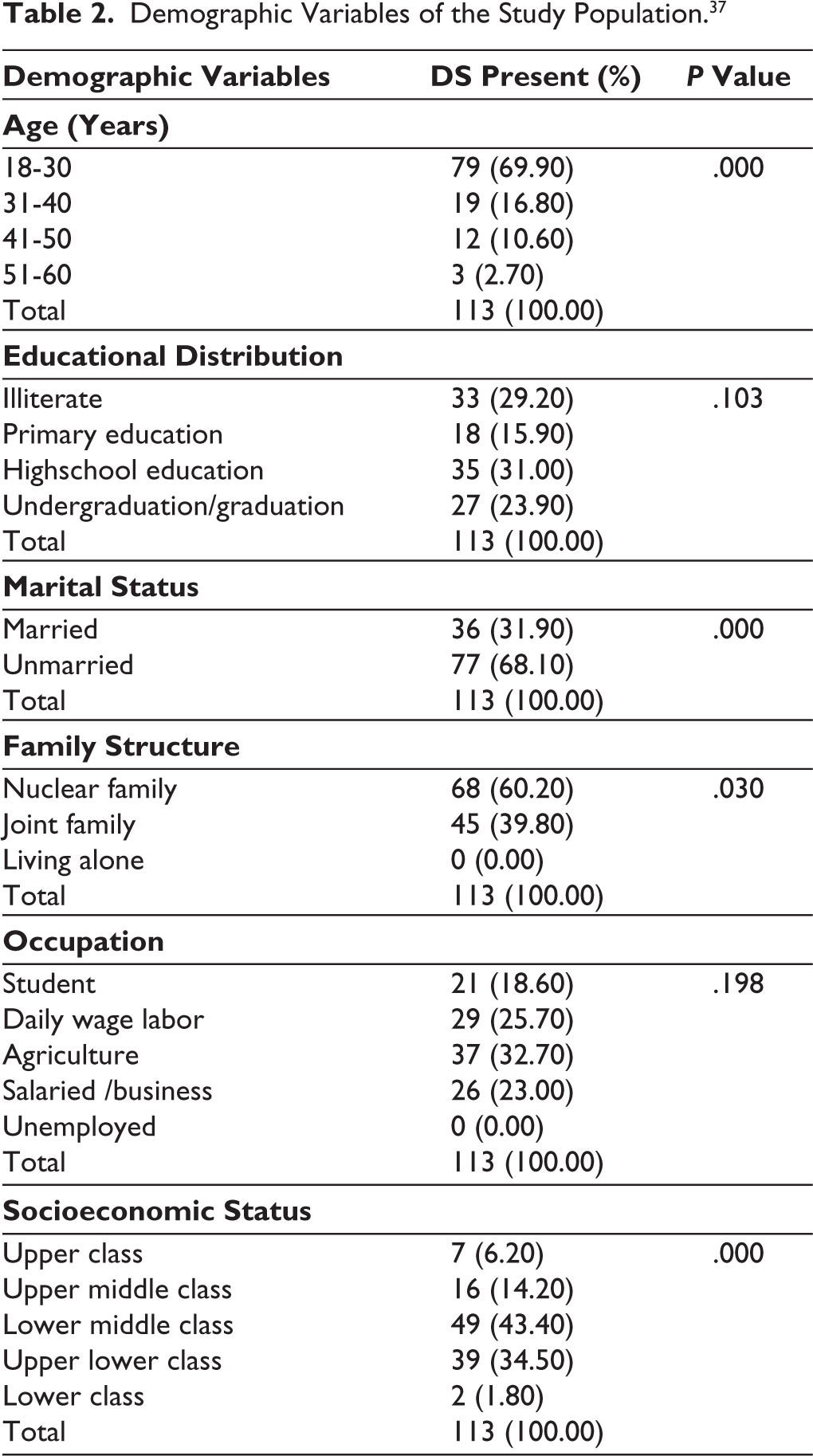
Furthermore, in Table 2, DS did not show any statistically significant (P = .198) prevalence across all occupational groups. DS was observed in 32.7% of agriculturists, 25.7% among daily-wage laborers, and 23% of the salaried and business population. Eighteen point six percent of the DS cases were found among students. DS was least prevalent in subjects from extreme poles of socioeconomic status, and the differences were statistically significant (P = .000). Forty-three point four percent of the subjects were from the lower middle class, and 14.2% of the cases were from the upper middle class; thus, almost 60% of the DS cases were found in the middle socioeconomic group.
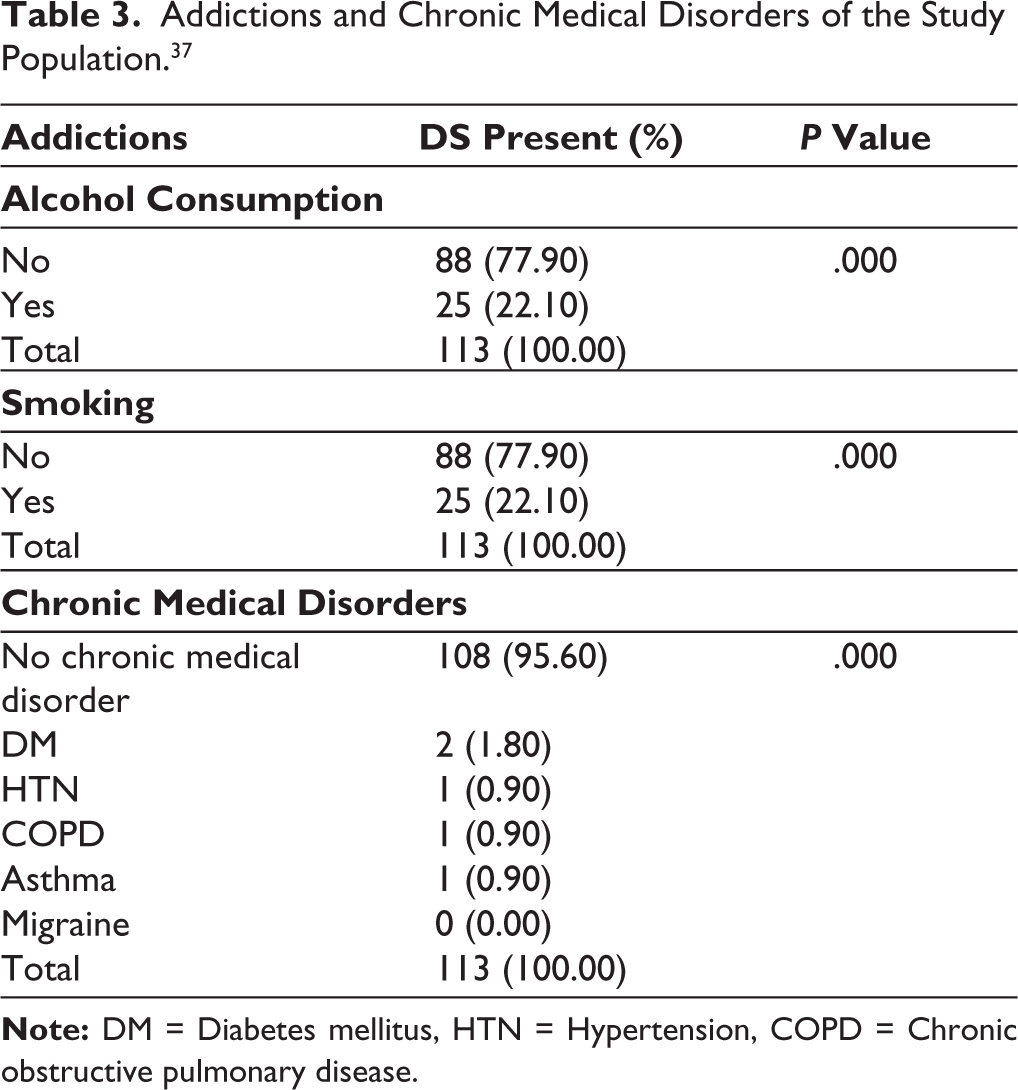
Table 3 summarizes that about 22.1% of the subjects with DS consumed alcohol, and a similar percentage of the subjects reported smoking, with statistically significant differences (P = .000). DS was not significantly higher in subjects with chronic medical disorders. Only 1.8% of the cases were found to have associated diabetes mellitus. Subjects with hypertension, chronic obstructive pulmonary disease (COPD), and asthma in total contributed only 2.7% of the cases.
Addictions and Chronic Medical Disorders of the Study Population. 37
Comorbid Psychiatric and Sexual Disorders with DS
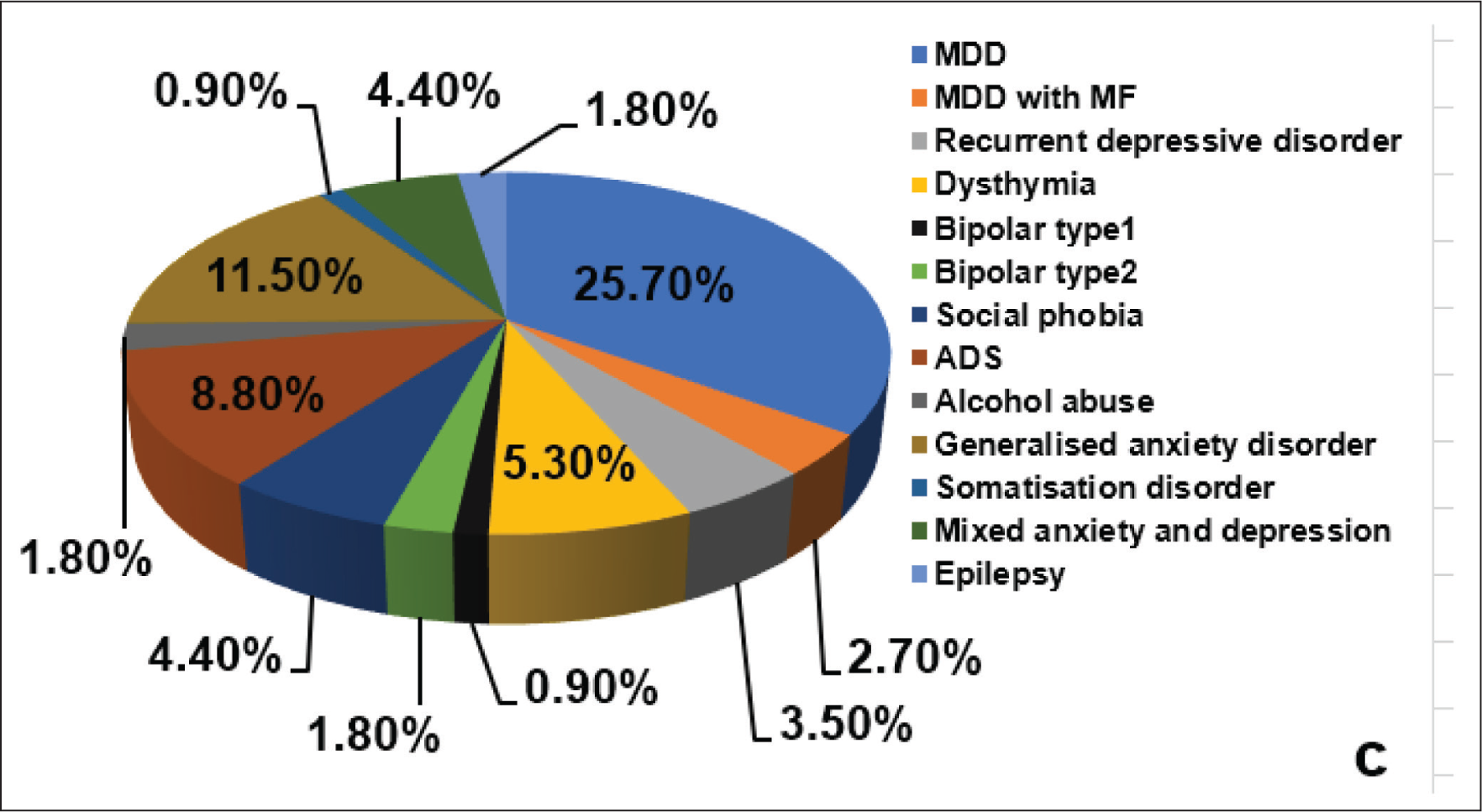
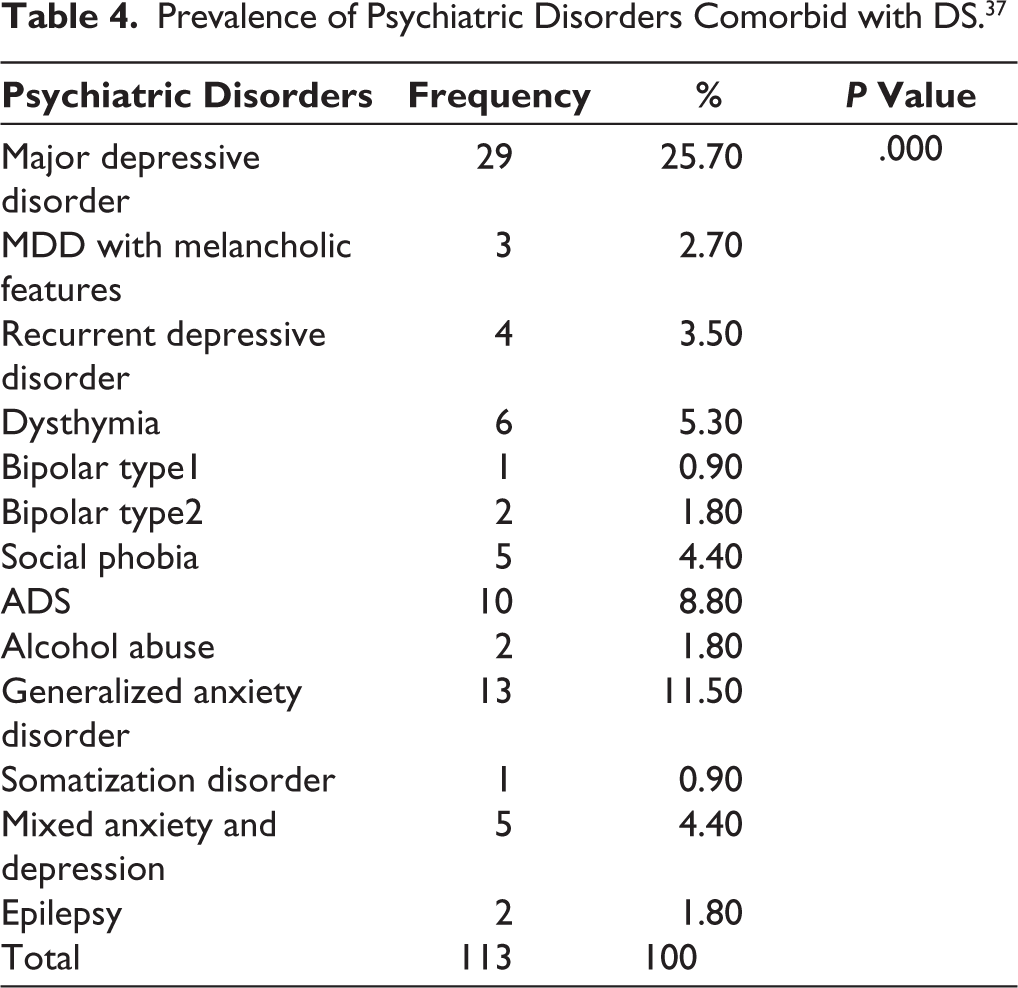
Cross-tabulation for the prevalence of psychiatric and sexual disorders was done across both the subjects with and without DS. Through this tabulation, the difference in these prevalence rates among both the subjects with and without DS was analyzed. Also, the contingency coefficient was obtained at a significance (P value) of .000. About 25.7% of the subjects with DS were found to have comorbid major depressive disorder. If all the depression spectrum disorders were diagnosed in these study subjects, such as major depressive disorder, major depressive disorder with melancholic features, recurrent depressive disorder, and dysthymia, all summed up together, 37.2% of the subjects with DS were found to be suffering from depressive disorders. Alcohol dependence syndrome (ADS) was diagnosed in 8.8% of the cases of DS. Including all the anxiety spectrum disorders, such as social phobia, generalized anxiety disorder, mixed anxiety and depression added together, it was found that 20.3% of the subjects with DS had anxiety disorders. The results revealed that a total of 57.5% of the subjects with DS either had depression or anxiety disorders (Table 4, Figure 1).
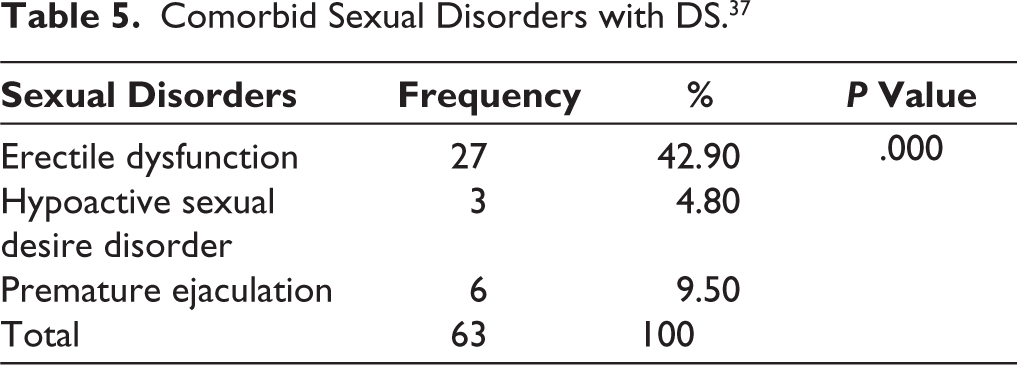
Sexual disorders were assessed only in subjects above 18 years of age and who were sexually active. So, the 50 subjects who had DS but were sexually inactive were excluded from assessment. It can be observed that 50 out of 113 subjects with DS were sexually inactive, while 246 subjects were sexually inactive among those who did not have DS. Analysis of comorbid sexual disorders showed that 42.9% of the cases with DS were suffering from erectile dysfunction. About 4.8% of the cases had comorbid hypoactive sexual desire disorder, and 9.5% of the cases with DS had premature ejaculation, which were statistically significant (P = .000) (Table 5).
Prevalence of Psychiatric Disorders Comorbid with DS. 37
Comorbid Sexual Disorders with DS. 37
Analyzing the crosstabs in Table 6 showed that the prevalence of psychiatric disorders was about three times higher in subjects with DS (73.50%) compared to subjects without DS (22.50%). ADS showed slightly higher prevalence among subjects without DS (9.10%) compared to subjects with DS (8.80%). The rest of all other psychiatric disorders were found to be significantly more prevalent in subjects with DS.
Psychiatric Disorders with and Without DS. 37
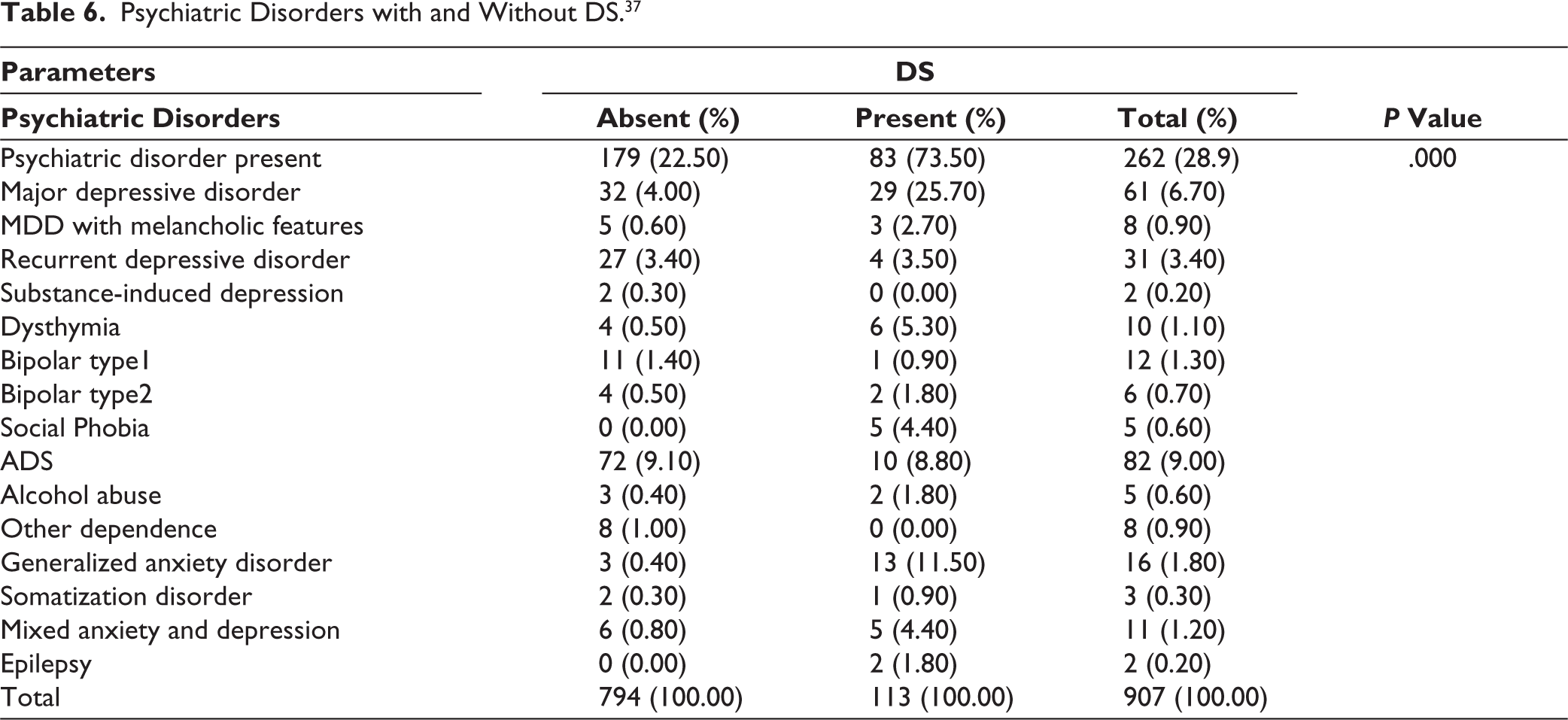
Table 7 revealed that comorbid sexual disorders were more than three times higher in subjects with DS compared to subjects without DS. About 42.9% of the subjects with DS had erectile dysfunction compared to 12% among those subjects without DS. Even hypoactive sexual desire disorder and premature ejaculation were found to be highly prevalent in the individuals affected with DS compared with those who were not. All the findings were statistically significant.
Sexual Disorders vs. Subjects with and Without DS. 37

Symptom Presentation of DS Described Under Physical, Psychological, and Sexual Categories
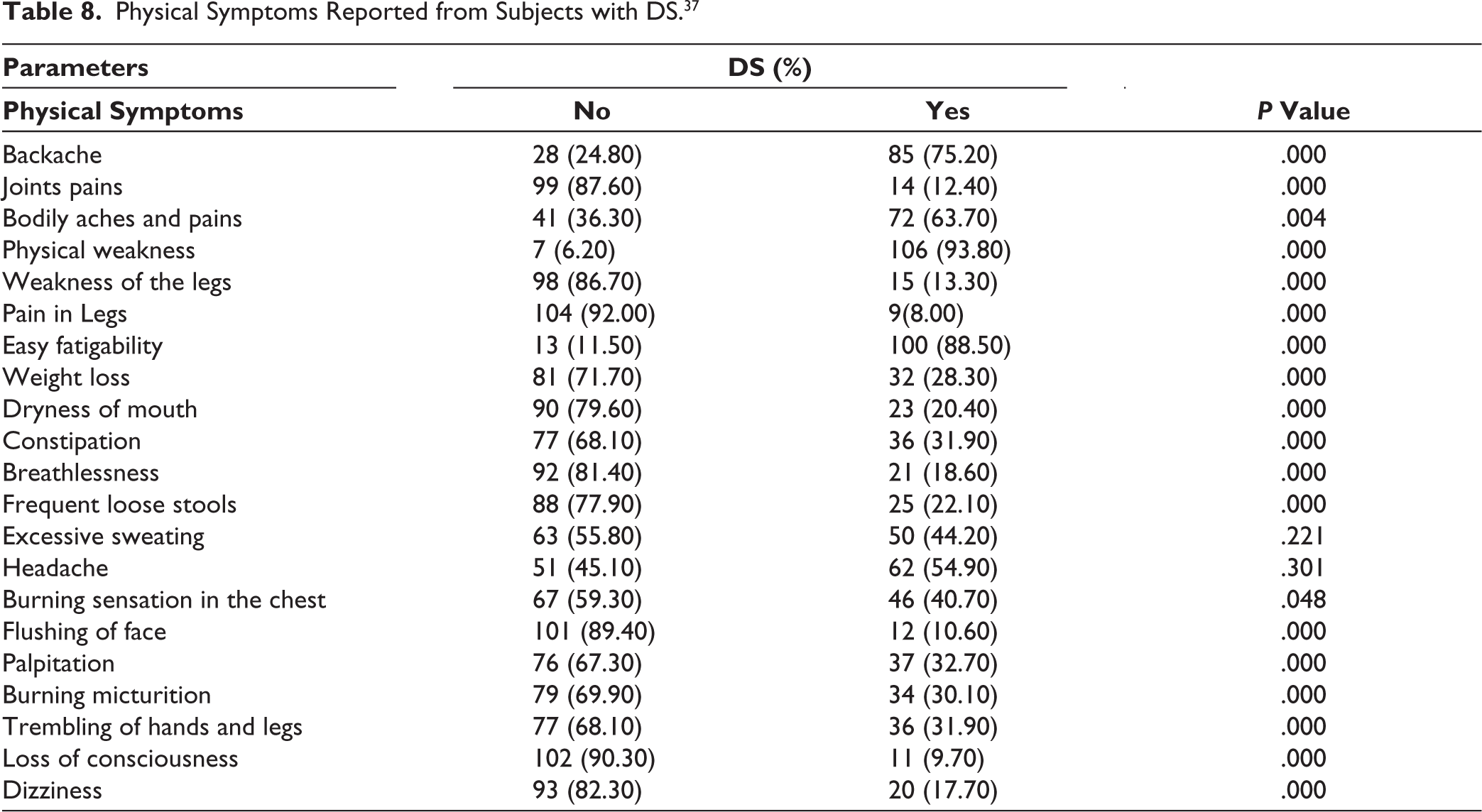
In Table 8, subjects with DS were interviewed in detail, and the symptoms they attributed to their “loss of semen,” considered a response for the disorder, were grouped. 21 different physical symptoms were assessed during the interview of 113 subjects with DS. The statistically significant physical symptoms reported from subjects with DS in this epidemiological study were physical weakness (93.80%), easy fatigability (88.50%), and backache (75.2%). The least common reported symptoms were pain in legs (8%), loss of consciousness (9.70%), flushing of face (10.60%), and joint pains (12.4%).
Physical Symptoms Reported from Subjects with DS. 37
Subjects with DS who attributed their symptoms to the loss of semen were also interviewed for their psychological attributional styles (Table 9). About 19 different psychological symptoms were assessed during the interview of 113 subjects with DS. The most common psychological symptoms reported by the subjects with DS were low self-esteem (100%), loss of interest in any activity (95.60%), feeling of guilt (92.00%), and decreased social interaction (90.30%), which were statistically significant. The least common ones were those of restlessness (0.00%), excessive shy feeling (16.80%), and lack of interest in previously pleasurable activity (26.50%).
Psychological Symptoms Reported from Subjects with DS. 37
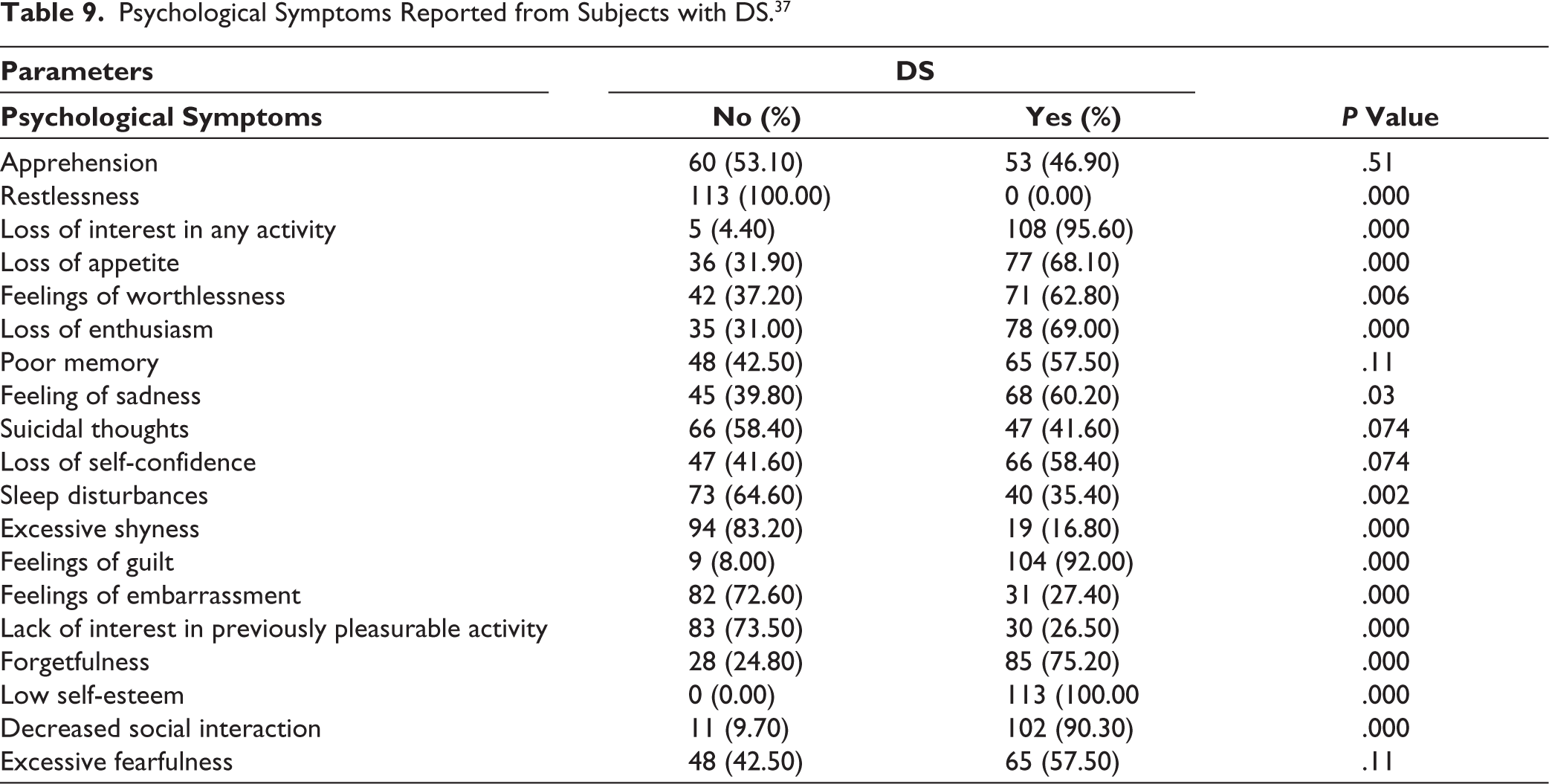
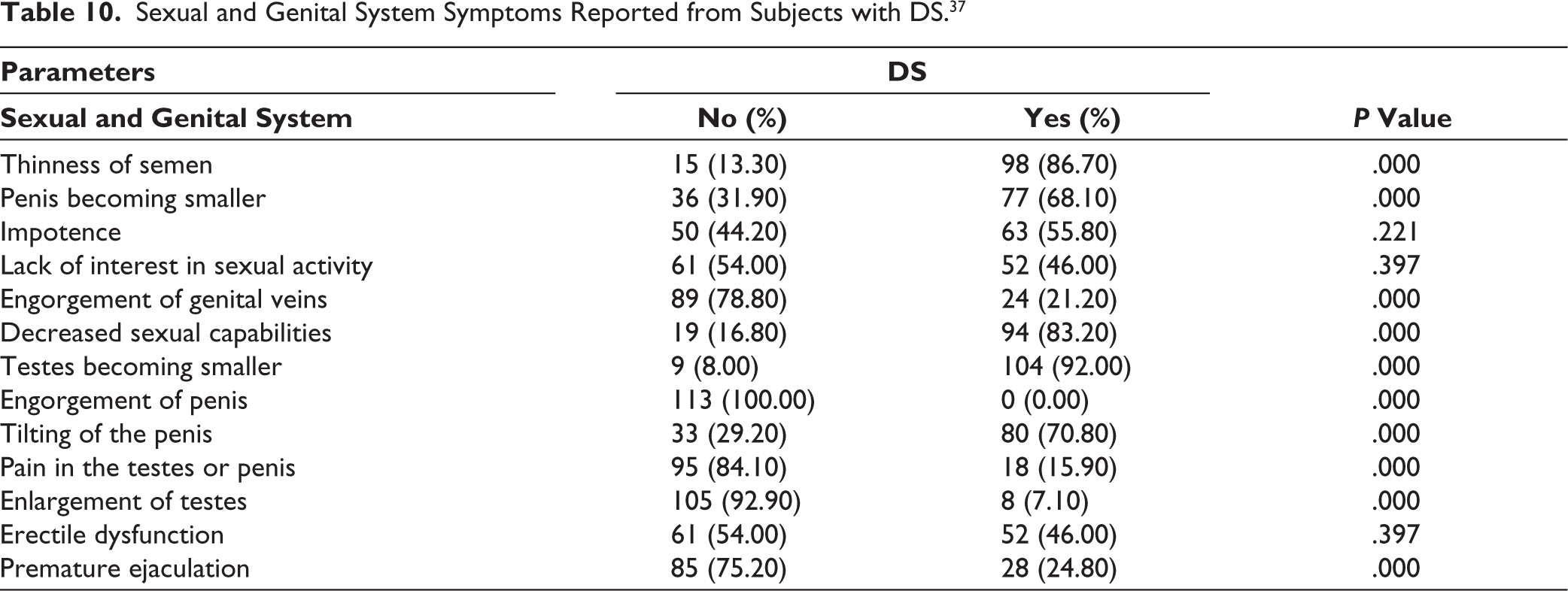
Table 10 summarizes the perceived sexual and genital symptom profile of the patients who attributed loss of semen to DS. About 13 varied sexual and genital system manifestations were assessed during the interview of 113 subjects with DS. The most common sexual symptoms reported from the subjects with DS were testes becoming smaller (92.00%), thinness of semen (86.70%), decreased sexual capabilities (83.20%) and tilting of penis (70.80%) with highly statistically significant changes (P = .000), while engorgement of penis (0.00%), enlargement of testes (7.10%) and pain in testes or penis (15.90%) were reported by very few.
Sexual and Genital System Symptoms Reported from Subjects with DS. 37
Discussion
The results of this epidemiological study among 907 subjects shed light on important parameters such as demographic and socioeconomic status, prevalence of DS, comorbid psychiatric and sexual disorders with DS, and symptom profile described under physical, psychological, and sexual symptomatology. To the best of our knowledge, this is the first epidemiological study anywhere in the world on this particular disorder. The prevalence of DS was found to be 12.5% in the studied general population (125 per 1,000 population). Out of 907 subjects from the south Indian rural population, 113 subjects were found to have DS.
In terms of demographic and socioeconomic status, highest prevalence of DS was observed between 18 and 30 years of age groups (69.90%), in those without formal education (29.20%), unmarried groups (68.10%), those residing in nuclear family (60.20%), agriculturists (32.70%), lower middle socioeconomic class (43.40%), and in people without chronic medical disorders (93.70%), smoking or alcohol addictions (77.90%). This study also reveals that the prevalence of DS is higher in males from rural areas, especially those with lower age, recent marriage, illiteracy, low socioeconomic status, and many more. Similar findings have been replicated multiple times in previous studies.13,17,21,31–33,35 Though commonly spoken about in the rural population, DS has also been observed in the urban males. 44 An earlier study done by Khan 13 in Pakistan found 1,777 subjects with DS based on the ICD-10 diagnostic criteria. According to this researcher, DS was observed among subjects with ages ranging from 12 to 65 years, with a mean age of 24 years. However, a 2019 study by Shakya 45 reported that average age of 25.4 years, with age range of 14–45 years for DS and higher prevalence of DS (34%) was found within the age group of 16–20 years in Nepal. Another recent study by Shahi et al. 16 reported mean age of 25.39 (±5.81 years). The study also reported that the majority of the patients (61.53%) were educated beyond matriculation.
In the present study, about 25.7% of the subjects with DS had comorbid major depressive disorders, which is comparatively less than in the earlier studies on patients with DS with comorbid psychiatric disorders.20,33,35,44,45 In recent studies from the Indian sub-continent by Shakya, 45 Manore et al., 46 and Shahi et al. 16 reported depression as the most common comorbidity with a percentage of 68%, 38%, and 20.5% respectively. This becomes an important consideration as, through decades, DS has been criticized as not being an “independent disorder,” but actually a cultural variant of depression. 9 Longitudinal studies have reported DS to have poor long-term diagnostic validity, and the common association with depressive disorders has been a strong argument to consider DS under the broader “narrative” of depression and anxiety.47,48 On the other hand, in the study of sexual disorders, erectile dysfunction (42.90%) was most prevalent in the studied subjects compared to premature ejaculation and hypoactive sexual desire groups, which were evidenced by previous studies on DS.1,34,35,40,45,49 Regarding erectile dysfunction, the present data observed comparatively higher values than the earlier reported data of the DS patients in Nepal, 45 but within the range of another study by Prakash. 1 However, a recent study from India reported a higher prevalence of premature ejaculation (50.42%) followed by erectile dysfunction (46.15%) in patients with DS. 16 Moreover, few studies have actually concentrated on diagnosing sexual dysfunction, and in those that have reported sexual dysfunction in DS, the use of any validated tool for diagnosis has not been mentioned. As briefed above, the present study used IIEF and PEDT, which are well-validated in the Indian context. This forms an important strength of the study. However, the varying results could have also been due to the difference in sample size and the different diagnostic procedures followed in each study.
The most common physical symptoms reported from subjects with DS in the present study were physical weakness (93.80%), easy fatiguability (88.50%), and backache (75.2%). While low self-esteem (100%), loss of interest in any activity (95.60%), feeling of guilt (92.00%), and decreased social interaction (90.30%) were the frequently reported psychological symptoms. Common sexual symptoms reported were the testes becoming smaller (92.00%), thinness of semen (86.70%), decreased sexual capabilities (83.20%), and tilting of the penis (70.80%). It was reported in past studies that patients with DS are known to manifest a great variety of physical, psychological, and sexual symptoms, which are attributed to loss of vital essence like semen or “dhatu” in the South Asian population.49–51 Singh had found that 73.8% of patients with DS had physical and psychological symptoms, which included headache, depressed mood, and anxiety. 52 Bhatia and Malik 50 also reported DS in 144 subjects with physical symptoms, among which weakness and fatiguability were reported by 71% and 69%, respectively. However, another recent study, physical illness (34%), mood symptoms (84%), anxiety symptoms (74%), and premature ejaculation or erectile dysfunction as sexual disorders in DS subjects have been reported. 45 The present research pertaining to varied manifestations of DS reconfirmed its polymorphic nature, which again needs to be interpreted based on the cultural connotations of rural India. Misinformation, rumor-mongering, and misattributions are important components of symptom formation in DS patients that help in formulating a comprehensive management plan. 36 Even though the study looked at their perceived symptoms and physical attributions, it did not examine these factors in depth, which remains a limitation. Addition of a qualitative component would have been better in understanding their lived-experiences and attributional styles. Also, the pathways to care for these patients serve as an important area of study. Studies show predominant consultation with traditional healers and psychiatric referrals occur much later.15,48 Symptoms reported in our study were also found in various other research, ranging from past to recent times.21,22,27,33,34,36,45,49 Considering the high prevalence of DS in this epidemiological study, higher psychosexual comorbidity, and relatively moderate association with depression and chronic medical conditions, it can be posited that categorizing a polymorphic Culture Bound Syndrome (CBS) such as DS just under the broader rubric of “mood disorders” might be at best a reductionistic approach, leading to neglect in understanding the cultural nuances responsible for its evolution.
Conclusion
DS has always been an enigmatic disorder in psychiatry. The DSM-5 has only reserved it for the appendix without a categorical number, 53 and the upcoming ICD-11 is already debating about its nosological “niche,” most probably to be subsumed within an overarching category. 54 It has been argued that the “cultural idioms of distress” in DS are not unique to CBS, but can be considered as “sociocultural phenotypes” of major mental disorders. 54 On similar grounds, DS can be a distressing problem which overlaps with severe mental disorders such as depression, body dysmorphia, or delusional disorder. It offers unique understandings of the influence of culture and beliefs on psychopathology, further compounded by a lack of formal education and misinformation. However, it is to be understood that improvement in formal education levels may not reflect in a better understanding of this disorder; instead, specific sex education needs to be a part of the curriculum. 16 This community-based study in the rural population attempts to provide an overview of the common correlates of DS. It was observed that it is highly prevalent in a large group of the Indian society, mainly rural, young, unmarried men belonging to the lower socioeconomic class. In terms of physical and psychological symptoms, the common symptoms included physical weakness, fatigue, feeling depressed and hopeless, and anhedonia, while sexual dysfunction was observed in 50% of the patients, with premature ejaculation being the most common comorbid sexual dysfunction. The perceived changes in genitals, backache, and weakness were common manifestations that formed part of the DS symptomatology. It again points to the fact that individuals with this disorder culturally link psychosexual health to physical strength, vitality, and QoL, as discussed in earlier studies.20,35,36 People affected with DS do fear about their impotence and sexual functioning. Whether the psychological fear and symptoms in DS have a “cause-and-effect” relationship is still unclear, but longitudinal and mixed-method studies are necessary to disentangle the enigma of DS. There is a need to reconsider DS in the light of the newly available literature, so that, as a psychiatric disorder, it can establish its own clinical, phenomenological, and diagnostic standpoint. Whether or not DS will stand the test of time as a diagnosis is debatable, but this might facilitate awareness, early detection, and prompt treatment of this troubling disorder at various levels, which will be clinically beneficial.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Ethical Committee of JSS Medical College, Mysore vide JSSMC / ICE / 2510/2012-13 dated 25.10.2012 for the title “Comprehensive study of Prevalence rates, Symptom Profile, Comorbidity and Management of Dhat Syndrome in Rural and Urban Communities”.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Indian Council of Medical Research (ICMR), New Delhi vide No. 5/4-4/30/M/2008-NCD-1 originally sanctioned for the Suttur Study titled “To evolve a Module for Identifying the Psychiatric Morbidities Amenable for Identification and Management at Primary Health Centre set up with low cost”.
Informed Consent
Written informed consent was obtained from the participants.