
Abstract
Background:
Dhat syndrome is a culture-bound syndrome of the Indian subcontinent. Traditional and cultural teachings through generations, and myths and misconceptions about sex are its principal contributing factors. Although prevalent, there is scarcity in studies on Dhat syndrome, particularly from Bengal.
Aims and objectives:
1. To study the phenomenology of Dhat syndrome in men attending the out patients department (OPD).
2. To study the comorbid sexual and psychiatric disorders associated with Dhat syndrome.
Methodology:
This was a cross-sectional observational study conducted in the psychiatric OPD in a tertiary care medical college hospital in West Bengal. The duration of the study was 18 months. 122 patients were included in this study that fulfilled the inclusion and exclusion criteria. The diagnosis of Dhat syndrome was made as per International Classification of Diseases, Tenth Revision, diagnostic criteria for research (DCR) criteria. A semi-structured pro forma was used to obtain sociodemographic variables along with numerous physical and sexual symptoms. Mini International Neuropsychiatric Interview was applied for psychiatric comorbidities. Data were analyzed using Statistical Package for Social Studies 17 by SPSS Inc., Chicago.
Results:
122 patients met the inclusion and exclusion criteria. Majority of patients were among age group of 20 to 30 years (60.7%). 56.6% were from the Muslim community and 43.4% were from the Hindu community. 54.1% population was unmarried and 39.3% were newly married. Routes of passage were night falls in 62.3% patients, and 52.5% patients pointed toward passage through urine. Many patients reported passage of semen more than one route. All patients (100%) complained about generalized weakness and thinning of semen. 66.4% had generalized body ache, 55.7% complain about headache, 60.7% decreased body glow, 50% had loss of appetite, 98.4% had decreased self-confidence, sleep disturbance was reported in 34.3% patients, 58.2% reported that their penis was becoming smaller, and 49.2% patients reported decreased sexual capability. The most common comorbid condition was sexual dysfunction (39.3%) followed by depressive disorders (27.9%). Premature ejaculation was found in 54.17% patients and erectile dysfunction in 33.33%.
Conclusion:
Dhat syndrome is a common culture-bound syndrome in Bengal. It is widespread in the Muslim community also. The importance of exploration of sexual comorbidities in Dhat syndrome is very much needed.
Introduction
In Indian culture much emphasis has been given to the preservation of semen or “shukra.” Ayurveda, the ancient Indian system of medicine has mentioned that the balance between 7 “dhatus” or essential elements of body is important for well-being. 1 Semen is one of them and it is the perfect substance. 2 Preservation of semen has been promoted for physical, mental, and spiritual well-being even today by various religious organizations. The common belief is that food is transformed to blood, then to marrow and finally to semen. 3 It has been thought over years that 40 drops of blood are needed to form 1 drop of marrow and 40 drops of marrow are needed to form 1 drop of semen. 1 As per Bramhacharya literature, one drop of blood is formed from 100 units of food, and 100 drops of blood is needed to make 1 drop of semen. 4 As this belief is prevailing in our culture through generations it is a common belief that wastage of semen will cause imbalance of “dhatus” in our body causing physical weakness and illness. 5 Not only in Hindu culture but other religions (Buddhism, Sikhism, Islam, and Christianity) as well hold the belief that loss of semen is harmful to body and mind; thus, much emphasis has been given to its preservation.6-8
Culture has immense impact on sexuality. The expression of sexuality is greatly determined by the attitude toward sexuality in individual and sociocultural levels. Indian subcontinent as a whole expresses a conservative attitude toward sexuality. Sex is a taboo in India. Various myths about sexuality are widely spread in the subcontinent and traditional practitioners such as hakims and vaids, and unqualified practitioners such as quacks and self-proclaimed sex specialists have been continuously reinforcing these myths and misconceptions.9-13 In this cultural background people from the Indian subcontinent often suffer from a culture-bound syndrome called the “Dhat syndrome,” which is characterized by excessive preoccupation with loss of semen. Patients usually present with a wide range of vague somatic symptoms such as weakness, fatigue, loss of appetite, generalized body ache, etc.14–16 Many people have sexual dysfunctions in forms of erectile dysfunction, premature ejaculation, performance anxiety, excessive worry about sexual activities, decreased size of genitalia, etc. 17 Sexual dysfunctions are the most common type of comorbidity associated with Dhat syndrome. Numerous psychiatric disorders are found as comorbid conditions with Dhat syndrome. Depressive disorders being the second most common comorbidity with reported prevalence is 40% to 66% across studies;17-19 others being generalized anxiety disorders, panic disorder, somatoform disorders, and hypochondriasis.17, 20 Most of patients used get the information regarding usefulness of semen preservation from friends, relatives, local vaids, quack practitioners, or from advertisement by Ayurvedic practitioners. 21 People often attribute the syndrome to be because of excessive sexual stimulation, reading porn literature, seeing blue films or erotic pictures, masturbation, breaking in love affair, black magic, premarital or extramarital sex, intercourse during masturbation, bad habits like alcohol addiction, sleep problems, and so on. People suffering from the Dhat syndromes often seek treatment by traditional herbal or Ayurvedic medicines. They often take vitamin supplementation, antibiotics, aphrodisiacs, and even marriage as possible cures for improvement of health.3, 22, 23 Studies have suggested that Dhat syndrome is more frequently seen in young adults of the second to third decades, unmarried or newly married males, from families where a conservative attitude toward sex prevails, middle to lower socioeconomic status, comparatively less education level, and more in rural population than urban population.17, 20, 22, 24
Although it is the most prevalent culture-bound syndrome in our country, and so in Bengal, there is lack of literature from Bengalese population regarding the Dhat syndrome. In this study, focus has been given on detailed description of sociodemographic variables of patients suffering from Dhat syndrome, their various associated physical symptoms, and comorbid psychiatric disorders.
Material and Methods
This was a cross-sectional observational study conducted in the psychiatric OPD in a tertiary care medical college hospital in West Bengal. Permission from college ethical committee was obtained before conducting the study. The aim of the study was to study the sociodemographic profile of patients of Dhat syndrome, its manifestation, and the comorbidities associated with this disorder. The duration of the study was 18 months (August 2018 to February 2020). All patients visiting the OPD of the investigators (on Monday and Friday) and being diagnosed with Dhat syndrome were approached. The exclusion criteria were mental retardation, psychotic illness, organic mental illness, and organic cause of discharge through urethra or anus. Those patients who were willing to give informed consent were included finally in the study. Diagnosis of Dhat syndrome was made as per the International Classification of Diseases, Tenth Revision, DCR criteria. 25 A semi-structured pro forma was used to obtain sociodemographic variables along with numerous physical and sexual symptoms. The list of the symptoms was prepared from the review of literature. There was a provision of inclusion of additional symptoms if reported by patients. Mini International Neuropsychiatric Interview was applied for psychiatric comorbidities. 26 Data were analyzed using “Statistical Package for Social Studies 17”.
Results
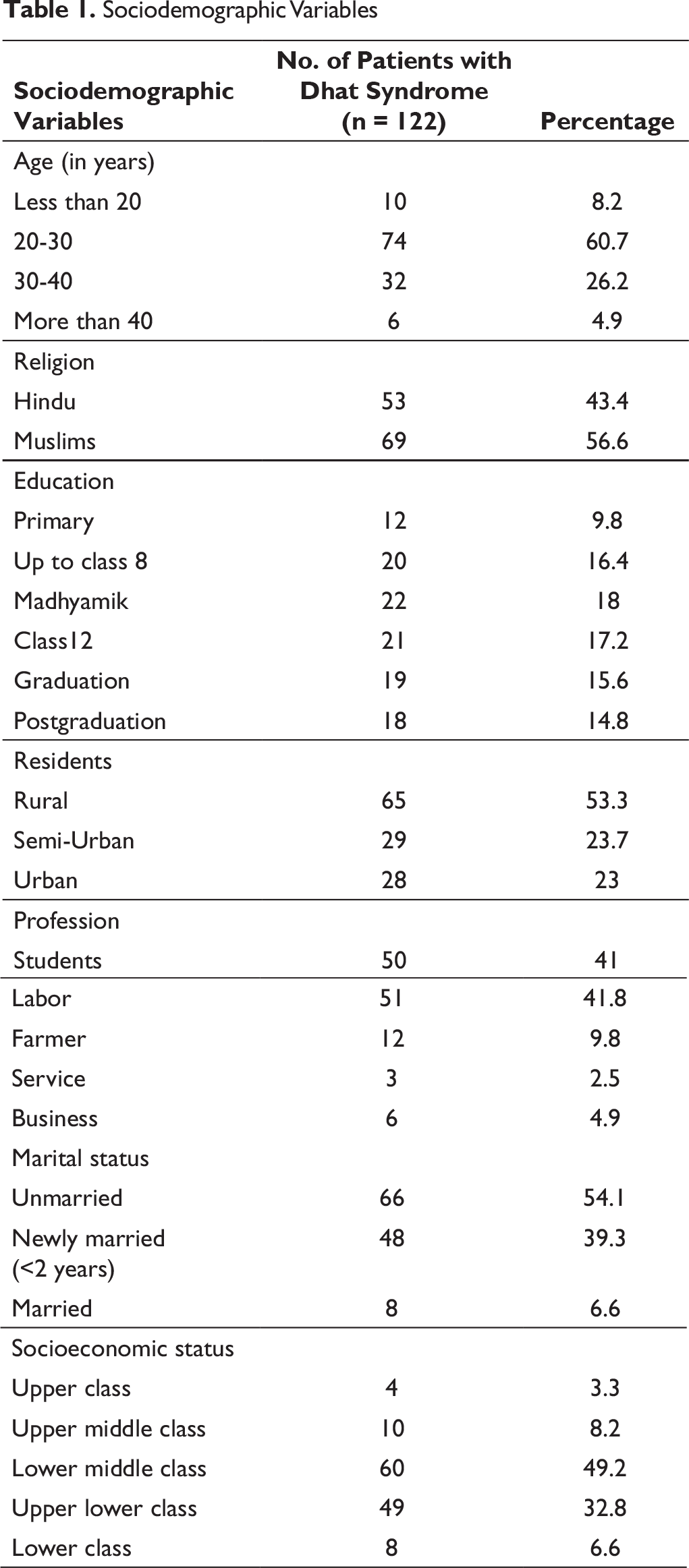
We had 122 patients meeting the inclusion and exclusion criteria. Majority of patients were among the age group of 20 to 30 years (60.7%), followed by 26.2% in the age group of 30 to 40 years. 56.6% were from the Muslim community and 43.4% were from the Hindu community. 54.1% population was unmarried and 39.3% were newly married (married less than 2 years). Regarding education, 9.8% were educated up to the primary level, 16.4% were educated up to eighth standard, 18.4% up to madhyamik, 17.2% up to higher secondary, 15.4% were graduates, 14.8% were postgraduates. 41% were students, 41.8% laborers, and 9.8% were farmers. For details of the sociodemographic profile, refer to Table 1.
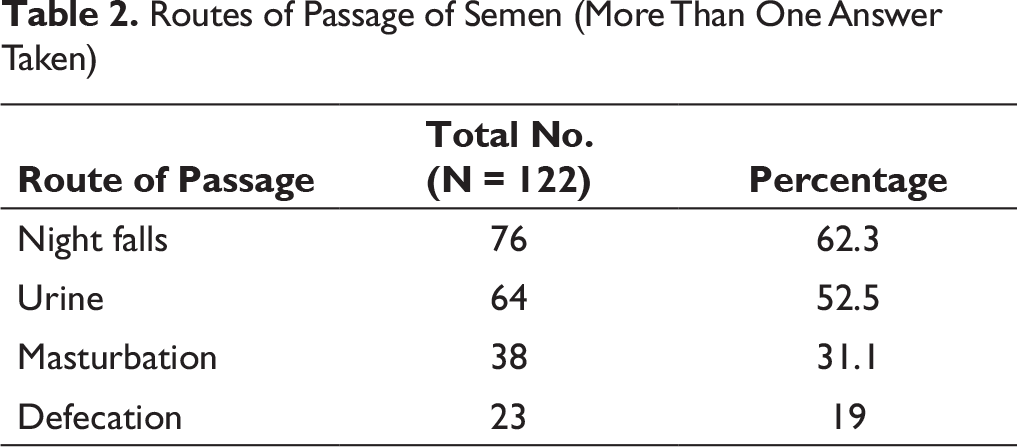
Routes of passage were night falls in 62.3% patients and 52.5% patients pointed toward passage through urine. Many patients reported passage of semen more than one route (Table 2).
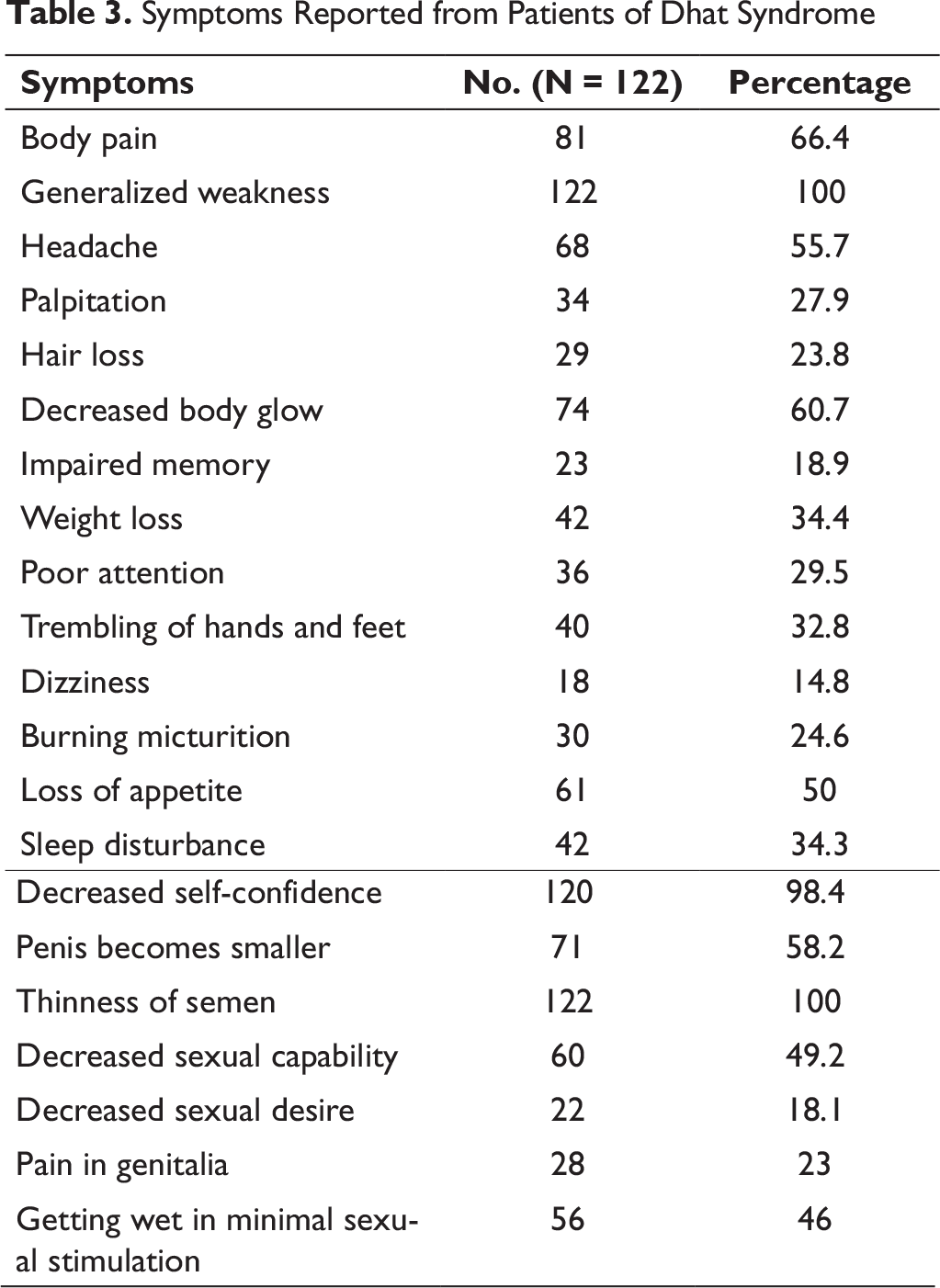
Patients of Dhat syndromes almost always present with multiple somatic symptoms. All patients (100%) complain generalized weakness, 55.7% complain of headache, 66.4% had body pain, 60.7% patients has a complain of decreased body glow, 35.2% patients mentioned about decreased size of genitalia, 50% had loss of appetite, 98.4% had decreased self-confidence, and sleep disturbance was reported in 34.3% patients. All patients reported thinning of semen. 58.2% reported that their penis was becoming smaller, and decreased sexual capability was reported in 49.2% patients (Table 3). 15.6% patients did not have any comorbidities.
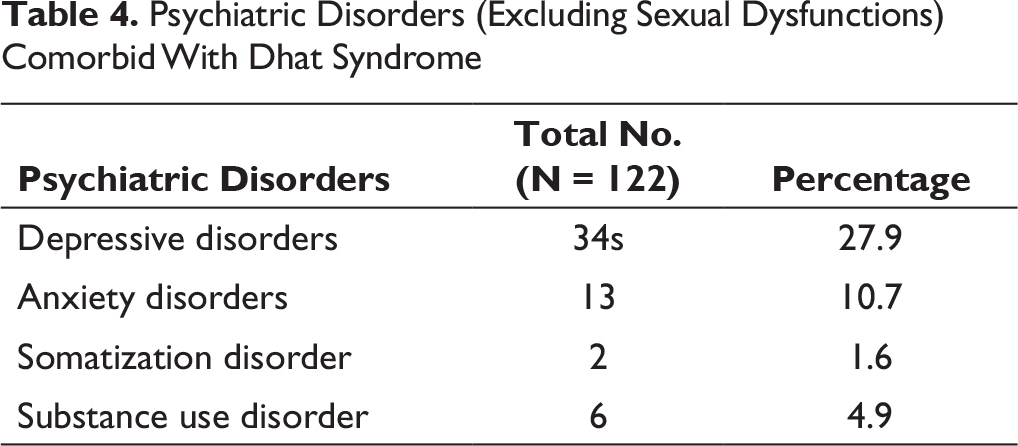
The most common comorbid condition was sexual dysfunction (39.3%) followed by depressive disorders (27.9%). Anxiety disorder was found in 10.7% patients (Table 4).
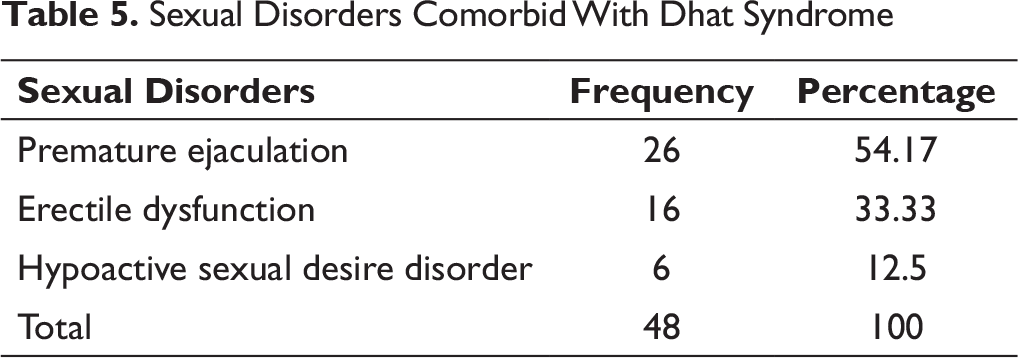
For the assessment of sexual dysfunction, the persons who were sexually active were chosen. We found that 66 patients were sexually active. Among them, 48 (72.7%) were found to have sexual dysfunction (Table 5). Premature ejaculation was found in 54.17% (n = 26) patients, erectile dysfunction was found among 33.33% (n = 16), and hypoactive sexual desire disorder was found in 12.5% (n = 6) patients.
Sociodemographic Variables
Routes of Passage of Semen (More Than One Answer Taken)
Symptoms Reported from Patients of Dhat Syndrome
Psychiatric Disorders (Excluding Sexual Dysfunctions) Comorbid With Dhat Syndrome
Sexual Disorders Comorbid With Dhat Syndrome
Discussion
Dhat syndrome being the most prevalent culture-bound syndrome in Indian subcontinent is widespread also in Bengal. But there is lack of studies exploring this syndrome, particularly among Bengalese. So it is still relevant to explore detail in today’s context. In our study, most of the patients were young adults of 20 to 30 years of age, from rural background; the findings are corroborative with most of the studies in our country.12, 13, 17, 20 We found Dhat syndrome most prevalent among students and laborers. A study by Nataraj et al revealed it to be visible in most patients from agricultural background. 27 Chadda and Ahuja found that Dhat syndrome is most prevalent in daily wage laborers, farmers, and shopowners. 28 Muslims were more in number than Hindus. All studies have found the disorder is more in Hindus in India, but almost all studies have shown that Dhat syndrome is also found among Muslims in a quiet good number.18, 24 More number of Muslims in this study was probably due to the religious profit of patients attending this particular hospital OPD in general. We found practically no difference in the education level among patients. It is generally believed that Dhat syndrome usually found in low to middle socialeconomic status, but a review of literature of records by Kendurkar et al by reviewing records of 1242 patients between 1979 and 2005 has shown that it is irrespective of educational status or domicile. 29 As found in most of the studies in the country, most of the patients are referred from OPD of dermatology and vernal diseases. 30 It is due to the common notion in the country that sexual diseases are treated by skin specialists. Most common route of passage of semen was nocturnal emission or night falls, followed by through urine. This finding was also found in a multicentric study by Grover et al, but they also found a significant number of cases while passing stool; on the other hand, we did not find it in more than 3 cases. 20 We found sexual dysfunction in 39.3% cases, most significantly among 72.7% patients who were sexually active. This indicates that sexual dysfunction is comorbid with Dhat syndrome in more than two-thirds of patients who are sexually active. In our study we found a significant number of patients who are newly married. Premature ejaculation is the most common sexual disorder. In our study comorbid depression was found in about one-fourth of the patients. Studies conducted in India showed a significant proportion of depressive comorbidity with Dhat syndrome. In India some studies found depressive disorders to be the most common comorbid condition, whereas some studies found sexual dysfunction to be the most common. It is mostly due to differences in the study setting.19, 20, 31, 32 Patients with Dhat syndrome manifest with a range of physical, psychological, and sexual symptoms which are attributed to the loss of semen. The most common symptoms found in our study are generalized weakness, decreased body glow, body ache, headache, poor attention span, sleep disturbance, decreased confidence, thinness of semen, decreased sexual capability, penis becomes smaller, etc.; finding corroborative with most of the studies.1, 3, 4, 17, 20
Conclusion
Dhat syndrome is commonly found in young males, unmarried or newly married, of all educational level and middle to lower socioeconomic status. Dhat syndrome is widespread in the Muslim community along with the Hindus. Most common mode of semen loss is night falls. Sexual dysfunction in the form of premature ejaculation is the commonest comorbidity. Depression is found in about one-fourth of patients. A wide range of somatic, psychological, and sexual symptoms are the common symptoms presented with Dhat syndrome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.