
Abstract
Abstract
Background: “Dhat syndrome” is described as a culture-bound syndrome, common mainly in the Southeast Asian region, including Nepal. We have limited data on this problem from Nepal.
Objective: To study clinico-demographic profile of “Dhat syndrome” cases, with the focus on its clinical presentations seen in psychiatry out-patient clinic of B. P. Koirala Institute of Health Sciences (BPKIHS).
Methodology: All consecutive out-patients with the diagnosis of “Dhat syndrome” coming into contact of the investigator in psychiatry OPD were enrolled during 12 months of study period. A pretested short questionnaire, including their view about “semen loss” and “masturbation,” was used. Psychiatric diagnoses were made according the International Classification of Diseases, Tenth Revision (ICD-10).
Results: Majority of the subjects were of productive ages; average age was 25 years. More of them were of Terai origin and from villages, though there were people also from other ethnic groups and urban settings. Most of them were educated but up to a middle/secondary level only. Most of the cases presented with depressive and anxiety symptoms, and semen loss, and were worried because they had heard or read that semen loss or masturbation was bad for health. They viewed semen as precious, something to be preserved, and masturbation a bad practice. Beside Dhat syndrome, two-thirds of the subjects (68%) had other ICD-10 psychiatric disorders, the most common being depression.
Conclusion: Psychiatric diagnoses are common among patients with “Dhat syndrome.” Most of these people view semen loss as a bad sign and masturbation a bad habit. Sex education is warranted for better health.
Introduction
Concept of “Dhat syndrome” (DS) or “semen-loss syndrome” is prevalent with different names in various cultures: Eastern and Western. However, it is common in the Indian subcontinent 1 and is also called “neurosis of the orient.” 2 This term DS was first used in Western text by N.N. Wig to characterize the condition by vague somatic symptoms of fatigue, weakness, anxiety, loss of appetite, and guilt attributed to semen loss through nocturnal emissions, urine, and masturbation even when there was no loss of semen. 3 Hypochondriacal, anxiety, and depressive symptoms are major psycho-pathology of semen loss in this syndrome, which is included in the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) (DSM-IV) under Appendix I as a “culture-bound syndrome” 4 and in the International Classification of Diseases, Tenth Revision (ICD-10) under “other specific neurotic disorders” (F48.8) as undue concern about the debilitating effects of the passage of semen. 5 Both the DSM-5 and the ICD-11 seem to struggle regarding how best to present cultural issues, including those related to DS. 6
Patients with this syndrome are usually young, recently married, belonging to average or low socioeconomic status (often a student, laborer, or farmer), from rural area, and from family with conservative attitudes towards sex.1, 7, 8 Duration of symptoms may vary from less than three months up to one year, even up to 20 years.1, 9, 10 Erectile dysfunction and premature ejaculation are the most common comorbid psychosexual dysfunctions and depression, anxiety, somatoform/hypochondriasis the most common psychiatric disorders in DS.7-11 Majority get the information about DS from friends, colleagues, or relatives; and the fear of semen loss and its cure is reported to be propagated by vaidyas, hakims, and advertisements.1, 7 Emphatic listening, a non-confrontational approach, reassurance, and correction of erroneous beliefs, along with the use of placebo, and antianxiety and antidepressant drugs are some treatment strategies.1, 3
There is scarcity of data about this common distressing illness, including its psychiatric comorbidity in the Nepalese context.12, 13 This study was carried out in the Department of Psychiatry, B. P. Koirala Institute of Health Sciences (BPKIHS), Nepal, in 2008/9 to see the clinico-demographic profiles, comorbid psychiatric disorders, and to explore into the view about “semen loss” and “masturbation” among DS cases.
Materials and Methods
It is an institute-based cross-sectional descriptive study conducted among the psychiatry out-patients with the diagnosis of DS 5 and coming into the contact of the investigator in BPKIHS, Dharan, Nepal, from October 2008 to September 2009. Demographic profile and information about illness were recorded on the “semi-structured pro forma” designed and pretested for this study. Detailed psychiatric work-up, necessary investigations and referrals were done. Final psychiatric diagnosis and comorbidities were made according to the ICD-10 criteria. 5 The subjects were asked two additional questions: “What they think about semen loss?” and “How they see masturbation?” Their views were explored by additional more elaborate questions made by the investigator as per the need, especially to know their view about the relationship with DS.
Data were entered into a computer and analyzed using “Statistical Package for Social Studies” (SPSS 17).
Results
Ethnicity, Residential Setting, and Educational Level
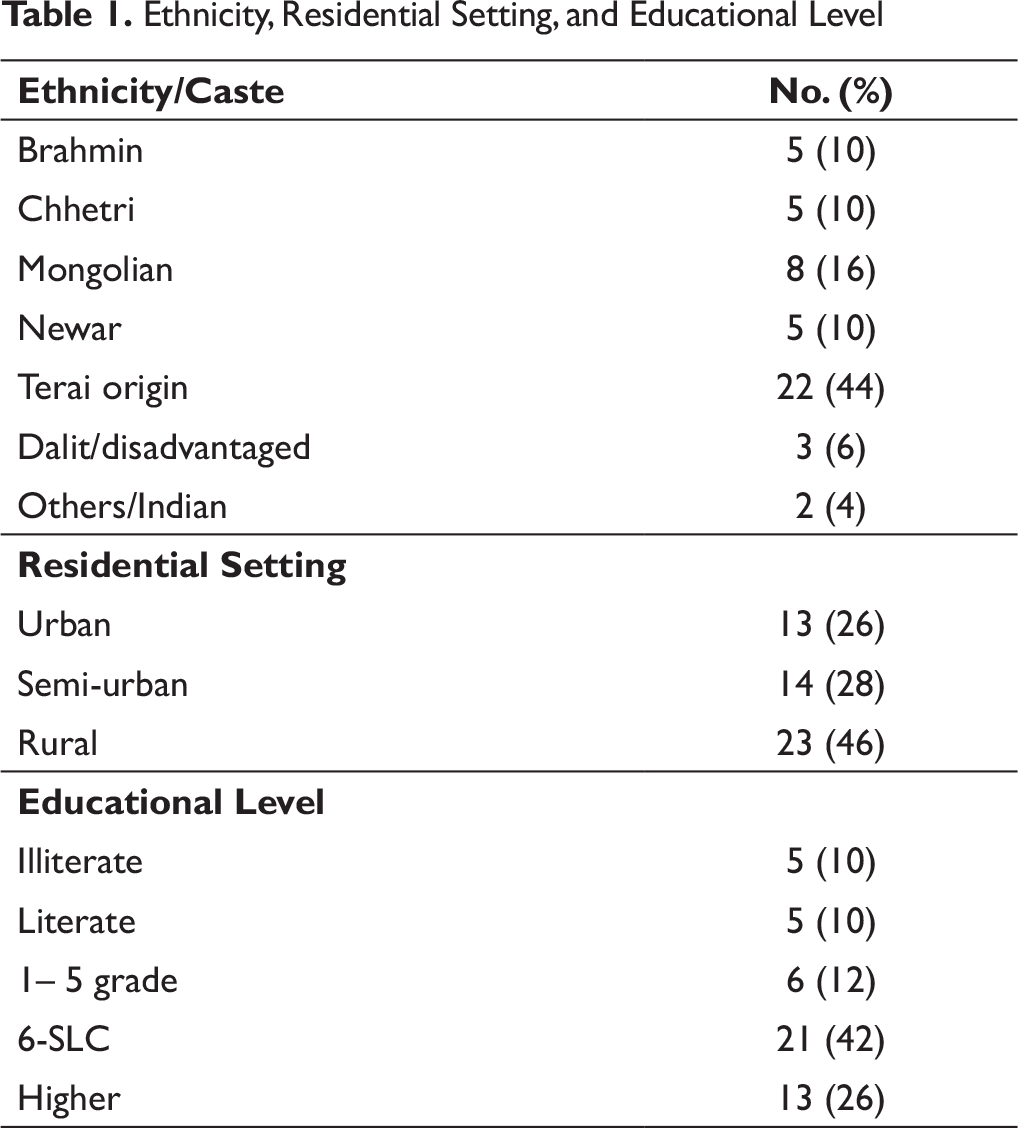
There were subjects from different ethnic groups seeking help for the syndrome, though more cases were of people of Terai (plain southern part of the country) origin (people of Terai origin include Mandal, Raya, Jha, Yadav, Shah, Gupta, etc., and those of Mongolian origin include Rai, Limbu, Tamang, Magar, Sherpa, Gurung, etc.). Subjects were from all residential areas, though more from rural settings. More of them had mid-level education (Table 1).
There were subjects from various professions, most commonly, students (50% [25]), service (26% [13]), farmers (14% [7]), laborers (6% [3]), and business (4% [2]).
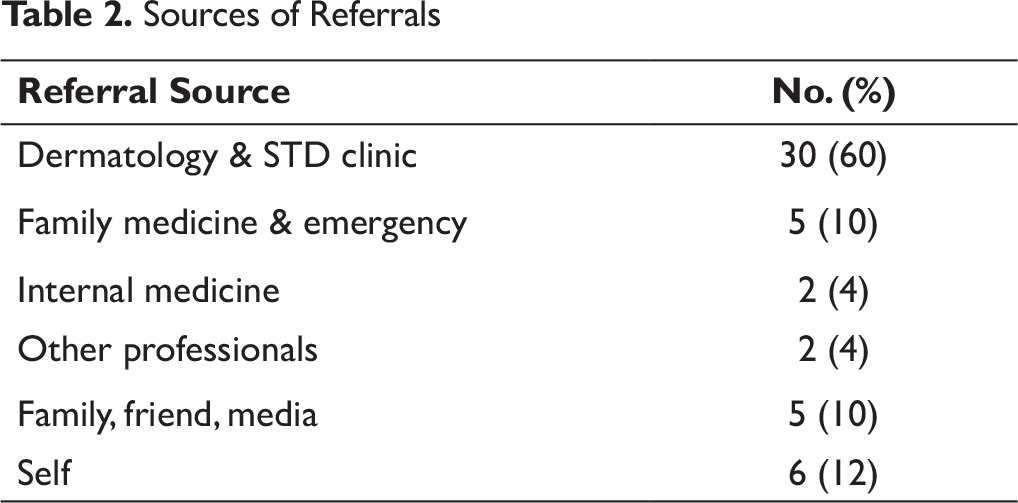
Most cases were referred by other departments of BPKIHS, mainly Dermatology (Table 2).
Sources of Referrals
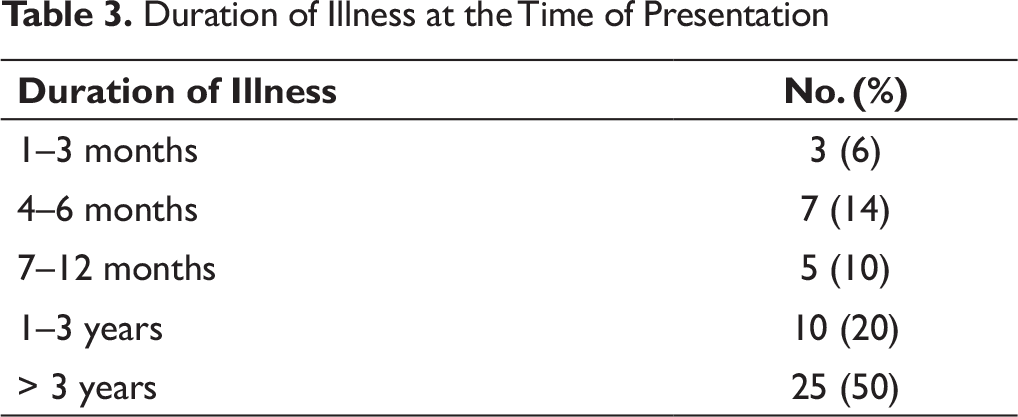
Duration of Illness at the Time of Presentation
Precipitating Stressors*
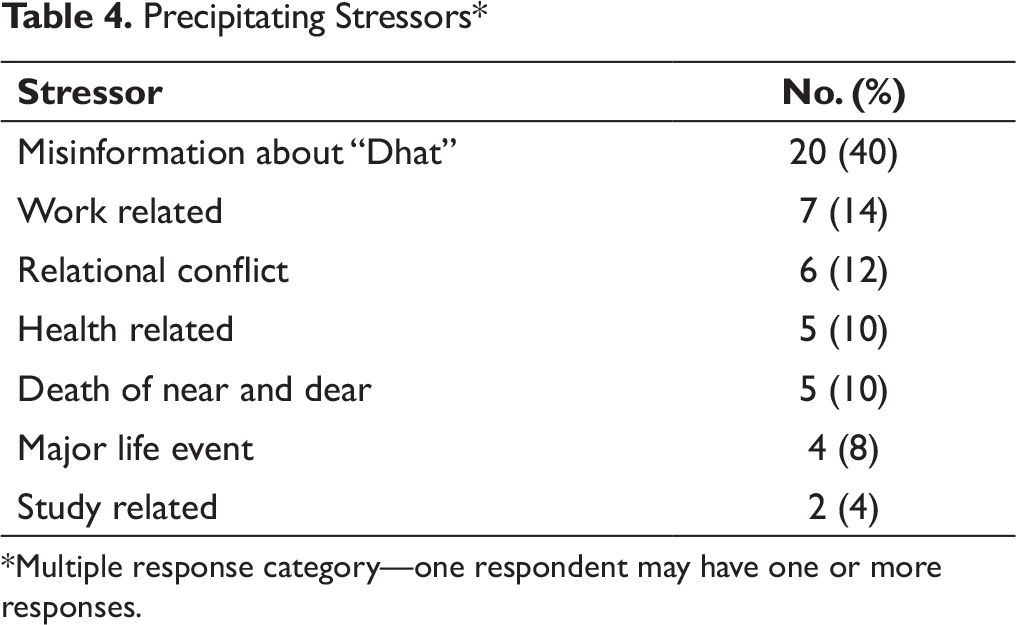
*Multiple response category—one respondent may have one or more responses.
In majority (80% [40]), some precipitating stressors were identified. Recent misinformation about “Dhat” and sexual problem was clearly the most common factor (Table 4).
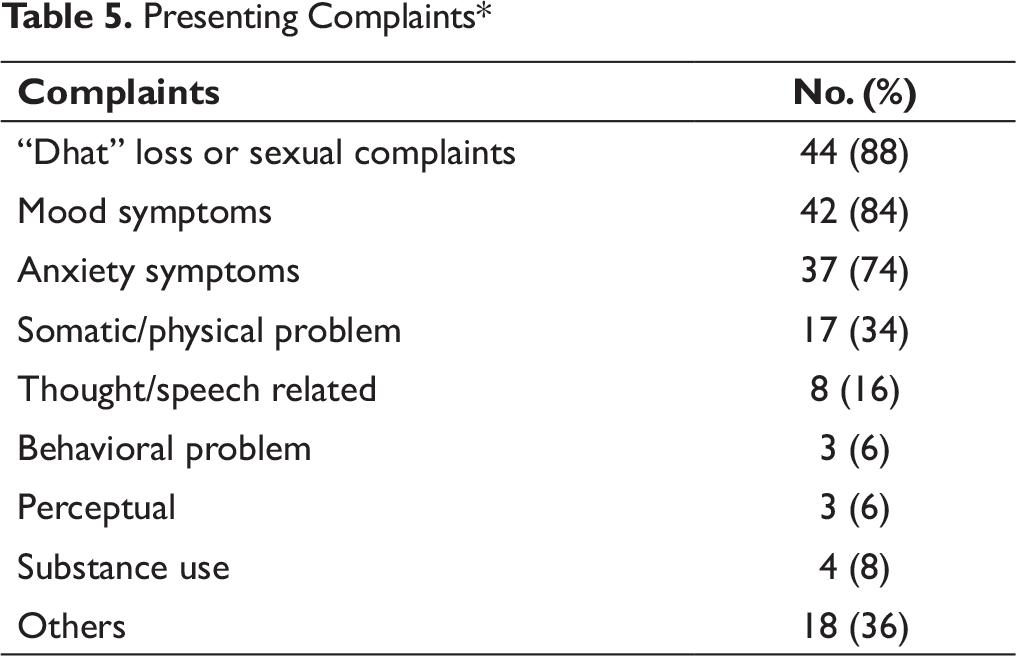
“Dhatu loss” was attributed by all subjects for current symptoms; and recent misinformation from some source regarding “Dhatu loss” and other semen loss related complaints were, clearly, the most common ones. Mood, anxiety, and somatic symptoms were other major presentations (Table 5).
Presenting Complaints*
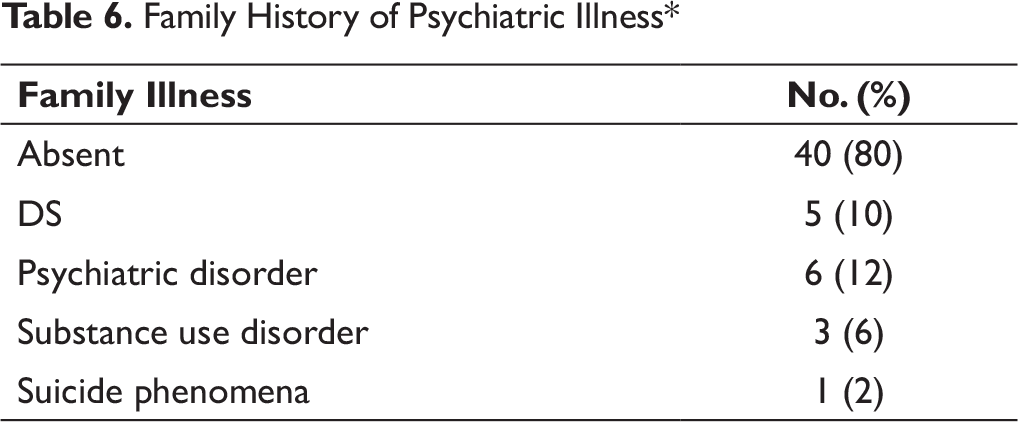
Family History of Psychiatric Illness*
Premorbid Personality Traits/Disorders*
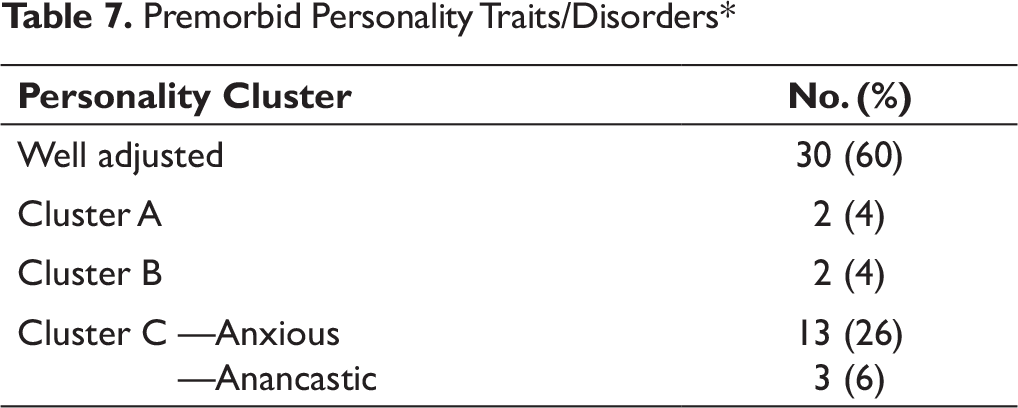
One-third (17) of the subjects had ab/used psychoactive substances, mainly alcohol (20% [10]), nicotine (16% [8]), and cannabis (4% [2]). Many of these subjects had anxious traits (Table 7).
Some subjects (18% [9]) had other diagnosed physical illness as well.
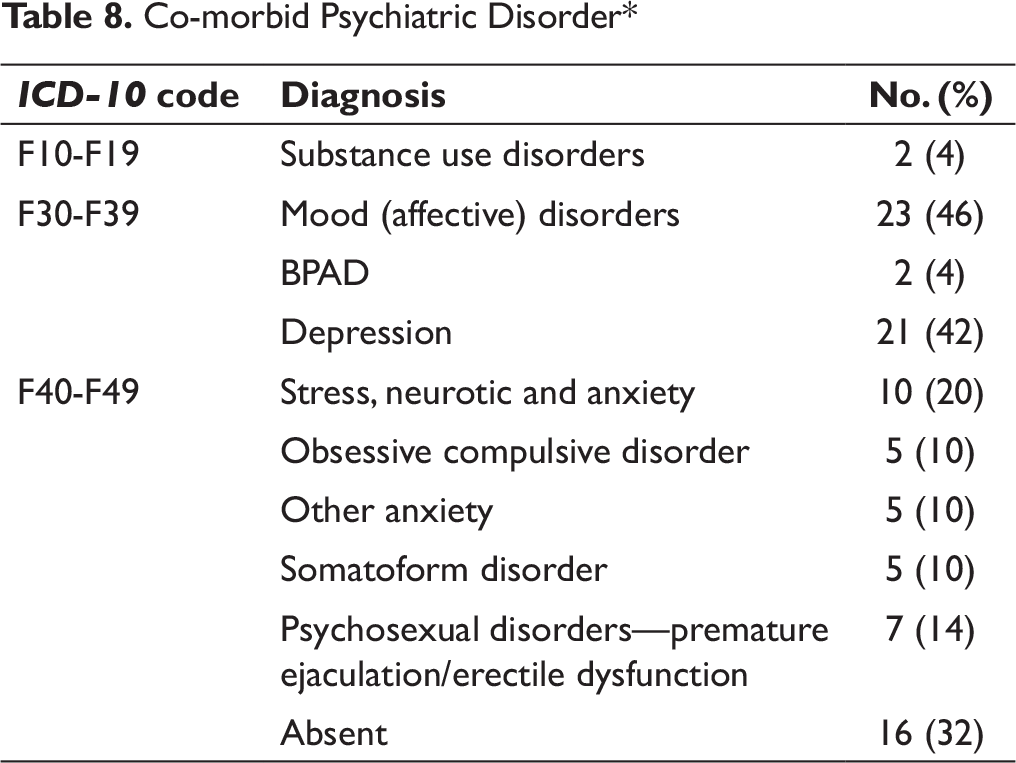
Two-thirds of these patients (34 [68%]) had some other mental illness (ICD-10) too. The most common psychiatric diagnosis was depression (44% [22]) (Table 8).
Co-morbid Psychiatric Disorder*
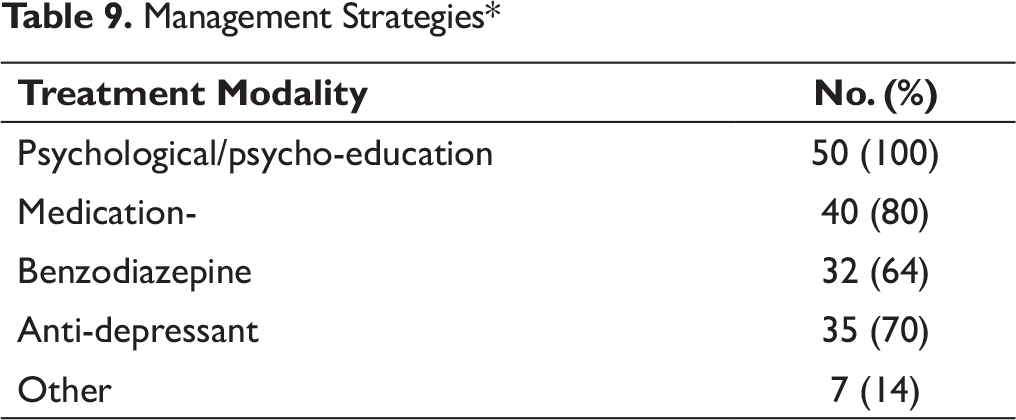
Management Strategies*
View About “Dhatu Loss” and “Masturbation”*
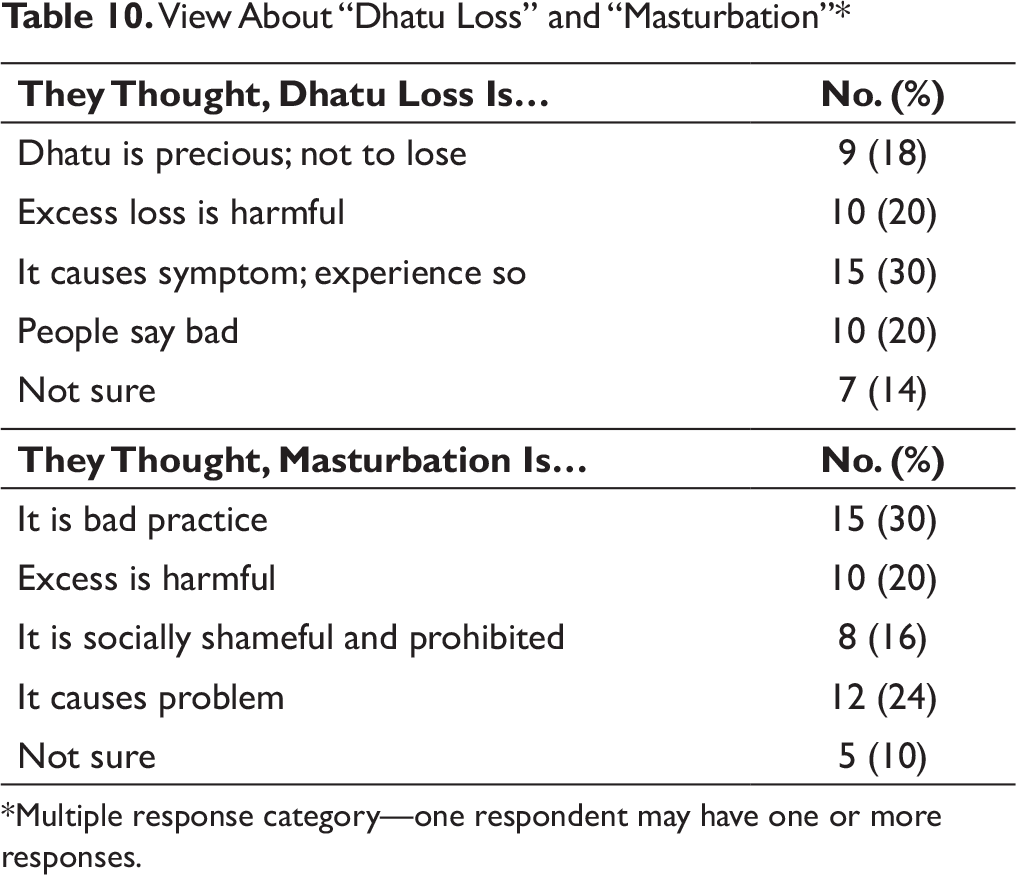
*Multiple response category—one respondent may have one or more responses.
Most of the respondents viewed “Dhatu loss” as a bad sign and masturbation as a bad or harmful practice (Table 10).
Discussion
Long back, DS was mentioned as widespread in Nepalese community as in other Indian subcontinents.1-3, 10 However, there has been a silence for long in medical literature from Nepal regarding this problem. This study was made in psychiatry out-patient setting of eastern Nepal with the modest objectives of looking into clinico-demographic profile of DS cases. Later in 2017, Dhungana et al. reported from a district in western Nepal. 13 It is still relevant to look into this problem even in today’s context of revision and update of the classification systems of psycho-social disorders.6, 14
Majority of our cases (70%) had presented after more than 1 year of duration of illness and half after more than 3 years. This is clearly after longer duration in comparison to others’ findings,1, 7, 10 including multiple set-ups, reflective of community 8 and similar to the finding of S. Grover et al. 15 They were either referred from other departments of the institute, mainly Dermatology and Venerology, or by other people because of other symptoms or increasing severity of illness. Sixty percent of our subjects were referred from the Department of Dermatology and Venerology (STD). Contrary to previous observations, 1 the onset was insidious and illness course continuous in majority of our clients.
Inherent as inclusion criteria, our subjects attributing their symptoms to semen loss (real or mainly imagined), 5 this, as a stressor, was ubiquitous. In 40% of the cases, recent misinformation about the effects of Dhatu loss precipitated and/or accentuated the symptom exacerbation; hence, they presented to us. As in other studies of psychiatric referral 16 and suicide attempt 17 from the same setting, in this study too, the common stressors reported by these cases included relational conflicts, health issues, death of some relatives, work or study issues, or other life events, mainly recent marriage. The latter finding of recent marriage or imminent marriage is consistent with the reports about DS from other parts. 1
As a defining feature, real or imagined “Dhatu loss” and other semen loss related complaints (e.g., turbid or milky urine, night falls, etc.) were the most common presenting feature. Keeping parallel to previous observations,1, 7, 10 mood, anxiety, and somatic symptoms were other major presentations in this study. Mood symptom means feeling dysphoric, sad, irritable, or labile. Anxiety features included physiological symptoms, e.g., palpitations, tremors, sweating, dry mouth, etc.; cognitive symptoms, e.g., worry mainly about the effects of semen loss in this study, ruminations, restlessness; and behavioral symptoms, e.g., avoidance of sexual topic or normal activities. Physical or somatic symptoms mean weakness, fatigue, heaviness of head, aches, etc. These symptom presentations keep well with the findings of M. S. Bhatia et al. intensively looking into common symptoms long back in an Indian scenario 10 and of M. Dhungana et al. recently in a Nepalese setting. 13 Substance use, a common problem here, 18 was reflected as a presenting complaint in this study as well.
Similar to previous reports from other countries and Nepal, two-thirds of these patients (68%) had other comorbid mental illness (ICD-10 diagnosis) along with DS. Depression was the most common psychiatric diagnosis, 11 followed as in other studies by stress, neurotic, and anxiety, including somatoform disorder.1, 7, 10, 14 Many of these DS patients also had psychosexual disorders, including erectile dysfunction and premature ejaculations. This finding again is in line with previous studies.1, 7, 10, 14 One-third (32%) had only DS. Based on the need, all of our cases received some sort of psychological intervention including psycho-education, sex-education, clarification, and majority of them also received medication, including antidepressants and benzodiazepines. This is consistent with the common medical practice. 1
From the perspective of socio-demography too, keeping parallel with common findings,1, 14 our patients were mostly young adult males, majority had middle-level education and were students. Though seen more among the people of Terai origins (from plain regions of southern Nepal towards Indian boarders) and from rural settings, we had clients coming also from other ethnicities and residential settings. One of the 50 total patients fulfilling the inclusion criteria was female in our observation. This finding replicates the notion of existence of this syndrome even in female patients, though much less than among males.19, 20
Clinically, our observation is also replication of the finding that these DS cases fall into any of three major groups1, 21: (a) Pure DS (with no other mental and psychosexual disorder), (b) DS with other psychiatric comorbidity (DS as part of these disorders, coincidence or these disorders accentuating DS symptomatology, or DS when not addressed appropriately or managed inappropriately which is a common occurrence as reported earlier from India and subcontinents and exacerbated by advertisements, untrained or self-claimed sex-therapists or hakim and vaidyas.1, 7, 8) and (c) DS with psychosexual disorders (mainly erectile dysfunction/impotence and premature ejaculation. This observation has been true not only in psychiatry out-patient setting but also in community-like settings 8 and psychosexual clinic. 15 This diversity of clinical picture raises question of its independent existence as a culture-bound syndrome or as a part of already established psychiatric entity. The answer is still far from the clarity.6, 14 As observed in the process of revisions and development of new versions/editions of classification systems, the ambiguity prevails because of such diverse clinical pictures arising out of the local contexts of varying perspective to semen loss in relation to onset of the symptoms. Understanding each case and managing accordingly will be the guideline as already outlined.1, 14 With this study finding also in our set-up, we recommend that young adult patients with depression, anxiety and somatoform disorders need exploration for DS and vice versa.
Our additional effort was to study their views on semen loss and masturbation, with two questions and needful clarification. Very similar to our deep-routed long-held belief,1-3 both semen loss and masturbation were bad according to majority of our subjects. As of now, DS seems to follow similar trends in its magnitude at least for foreseeable future in our parts, though there are reports of its declining trend with rising education status and increasing health/sex literacy. 2 Hence, evidence-based sex education needs to be spread at all levels for better overall health.
All our findings, however, should be viewed in the perspective of small sample size and hospital-based referral set-up basis.
Conclusion
DS cases coming into psychiatry OPD are male in majority. They are mostly young adults. Though seen more among people of Terai origins and from rural settings, it is also seen among other ethnicities and residential settings of eastern Nepal. Majority of them have middle-level education and are students.
Some had family history of similar problems in blood relatives. A few had STD treated in past. Many of these subjects had anxious personality traits.
Most cases were referred by other departments of the tertiary care institute, mainly Dermatology. Majority presented to psychiatric consultation after 1 year or more from the onset of illness. In majority of cases, some precipitating stressors were identified, recent misinformation about “Dhat” and sexuality clearly being the most common factors.
“Dhatu loss” and other semen loss related complaints were the most common ones. Mood, anxiety, and somatic symptoms were other major presentations. Two-thirds of these patients had some comorbid mental illness, depression being the most common psychiatric diagnosis. Some psychological intervention was done in all cases and majority of cases also received medication.
Most of the respondents consider “Dhatu loss” and masturbation as bad.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.