
Abstract
Koro syndrome has been colorfully described as a pathological distortion of one’s body image of the genital organ. In Koro, body image dysphoria is characterized by severe anxiety related to the delusional idea that one’s genitals will shrink and retract into one’s abdomen, eventually leading to death. This syndrome was first reported in South East Asia, where endemics have been described, but it has also sporadically occurred globally. We present a systematic literature review on Koro syndrome and report 7 cases from Canada. A search review with PubMed and Google Scholar resulted in 504 entries. Sixty-seven manuscripts were eventually selected following a thorough elimination process. The resultant literature underscored the cultural diversity that underlay the reported cases. Various aspects of Koro have been examined (eg, etiological, clinical, diagnostic, and cultural aspects). It has stimulated substantial scholarly debate, discussions, correspondences, and arguments from anthropological, psychiatric, psychological, and biological perspectives. In our series, it seems that Koro could have been misattributed here. The primary concern was not with penile retraction of the cases. To our knowledge, this is the first time that a series of cases is documented from North America where the syndrome is often ignored. We highlight the potential differences between the classical Koro syndrome and a collection of beliefs related to the perception or delusion of penile retraction in other codable psychiatric disorders, Koro-like syndrome. Understanding Koro syndrome beyond geographic boundaries is in line with our collected case reports of Koro from outside Asia.
Keywords
Introduction
In a stimulating editorial on Genital Dimensions, Drs Rao and Andrade wrote, “A physically attractive male is moderately but not excessively muscular, slim to moderate in build, and endowed with a large penis. These and many other idealized attributes vary across societies and across time.” 1 Koro is characterized by the extreme anxiety that results from the perception that one’s penis is shrinking or fear of its retraction into the abdomen and resultant death.2,3 Recently, Chowdhury and Brahma 2 suggested several options to ameliorate the studies: Koro-clinical diagnostic issues, demography of cases, comorbidity addiction/other mental and physical illness, boundness with culture, epidemic specificity, treatment traditional/modern, and recurrent Koro. Complete and incomplete forms of Koro are distinguishable because the latter forms typically do not entail a fear of imminent death (Table 1).
Distinction Between Classical Koro and Koro-Like Syndrome
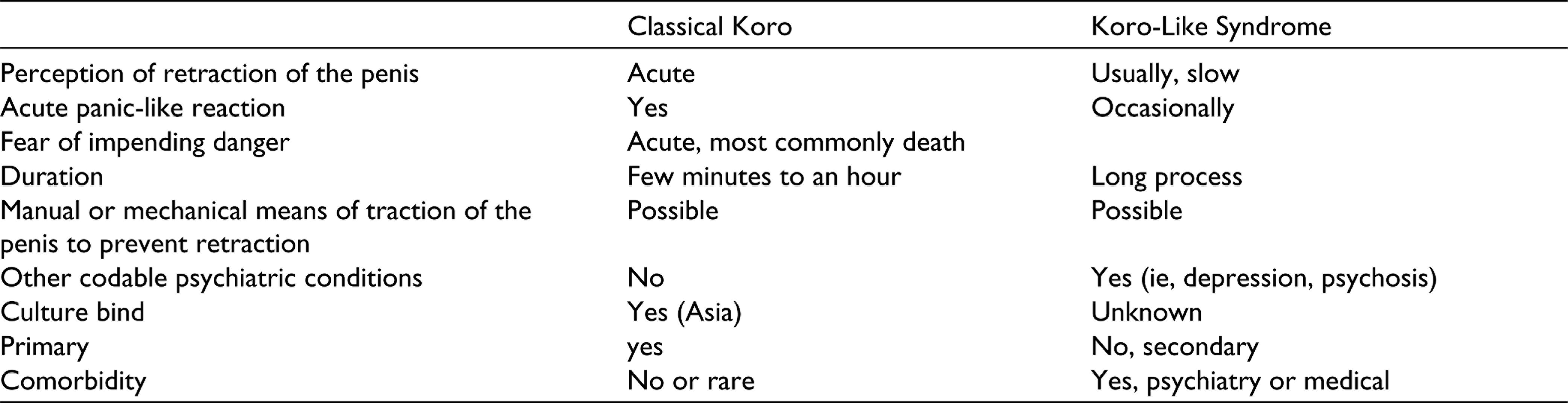
It happens that urologist colleagues request psychiatric consultations because they feel powerless in the face of patient complaints. The initiative for this article follows a succession of requests in Canada. Koro-like syndrome is often secondary to a urological complaint, and it occurs despite the normality of external genitalia, scrotums, cord structures, and testes. 4 Patients with Koro-like syndrome sometimes opt for penis enlargement surgeries at outpatient urology clinics. 4 It is important for clinicians to routinely enquire about symptoms such as impotence and a loss of virility and sexual control because patients tend to be reluctant to report these issues spontaneously. 5
However, patients concerned about the retraction of penis should not be attributed to Koro syndrome when they have other codable psychiatric disorders (psychosis and depression) and responded with psychotropics. We investigated here a novel research question to understand the syndromal presentation of Koro symptom in other diagnoses and separate it from the identity of Koro syndrome, which is culture-bound. We will describe a series of patients from North America, where it seems that Koro could have been misattributed here. The primary concern was not with penile retraction of the cases.
To do so, we first review the literature and present a case series to illustrate that this condition of expressing complaints about penile retraction can be seen worldwide. The participating patients provided informed consent, and 2 of them participated in the redaction of the article by providing relevant comments and suggestions.
Traditionally, culture-bound syndromes are usually localized in a specific area. Therefore, they are difficult to understand for outsiders to this cultural context. Interestingly, authors from India conducted a cross-sectional study highlighting the importance of understanding Koro syndrome beyond “geographic boundaries” and relating it to the phenomenon of migration stress: “It is time we stop seeing it just as “‘culture-bound syndrome’” and begin seeing it also as a social disorder caused by “‘distortion of body related beliefs’.” 6 Our article is intended to discuss the thesis of these authors, and our collected case reports of Koro are from Canada. 7 To our knowledge, this is the first time that a series of cases is documented from North America where the syndrome is often ignored.
Literature Review
A search of electronic databases for articles that have been published between 2006 and 2021 (inclusive) yielded 67 peer-reviewed articles that pertained to Koro. Specifically, we searched PubMed and Google Scholar for articles without language restriction. The articles were first abstracted by a reviewer (AT), and the abstractions were verified by a second reviewer (ES). We searched (a) PubMed for titles and abstracts that contained the word “Koro” and (b) Google Scholar using the “advanced search” and “with the exact phrase” options (ie, “Koro” in the title). Consequently, PubMed and Google Scholar yielded 67 and 504 articles (excluding patents or citations) that had been published between 2006 and 2021, respectively. Following the elimination of articles that reported unoriginal, incomplete, or irrelevant results and duplicate search results, we abstracted the information derived from 67 articles (case studies/series: n = 35). A review of the resultant literature underscored the cultural diversity that underlay the reported cases of Koro. It also revealed that various aspects of Koro had been examined (eg, etiological, clinical, diagnostic, cultural aspects). It has stimulated substantial scholarly debate, discussions, and correspondences. Arguments have been presented from anthropological, psychiatric, psychological, and biological perspectives.
Koro refers to the “head of a turtle” in Malay 8 ; however, the precise geographical origin of Koro remains unclear. Some of the first clinical descriptions originated from Sulawesi, an island in the Indonesian archipelago. 9 Although some cases have been identified in South China, like Guangdong and Fujian provinces,8,9 Koro is primarily associated with Southeast Asian cultures. Table 2 details the case reports included in this review from patients of Asian origin.
Koro Case Series With Patients of Asian Origin
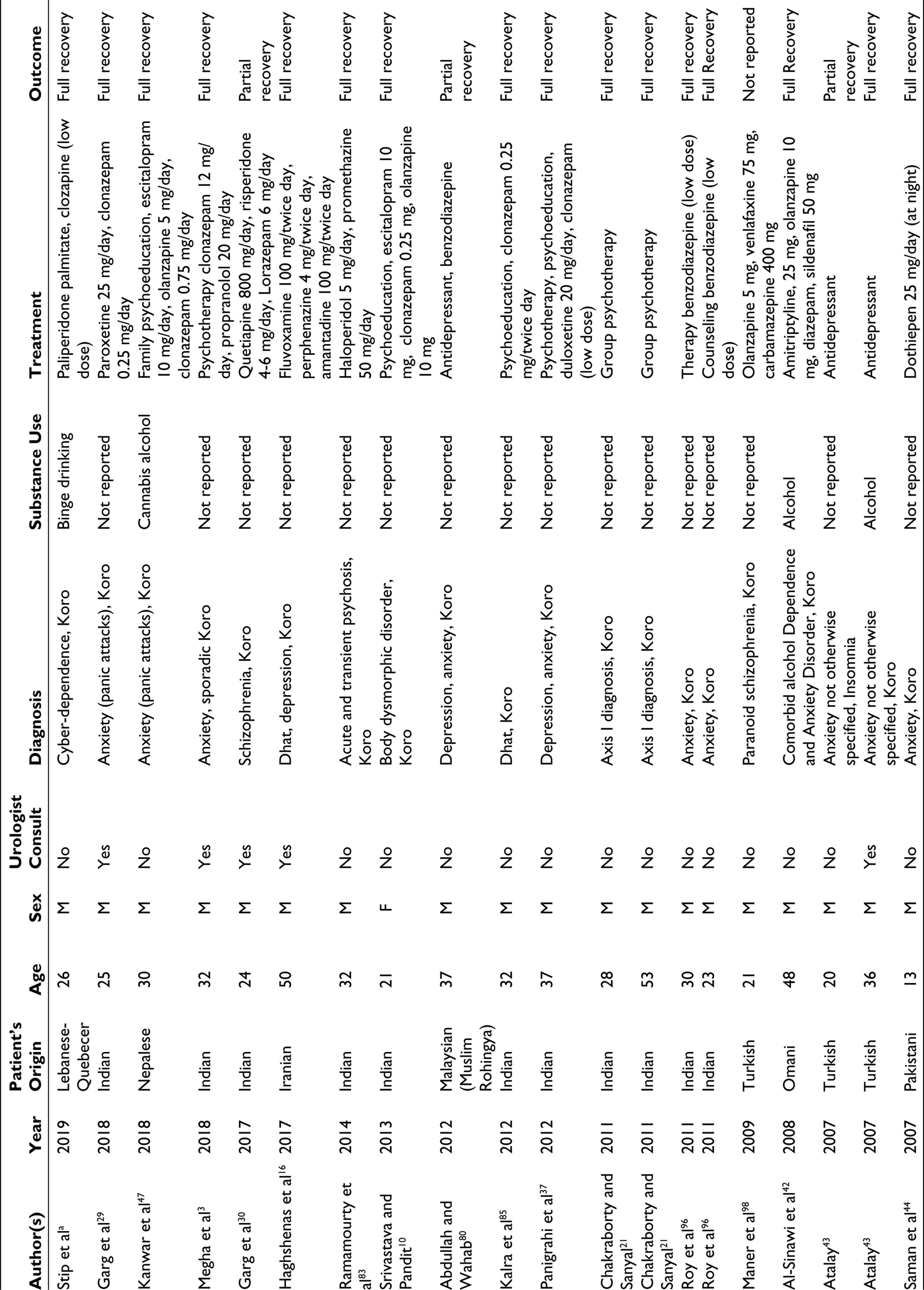
aData collected in the current clinical study.
Ancient Chinese medical literature has documented a comparable syndrome called “suo-yang” in Mandarin and “suk-yeong” in Cantonese. The core features of this syndrome pertain to the penis; therefore, Koro is evidently a male-specific condition. However, very rare cases of women who feared the involution of their vulva and breasts have also been reported. Nevertheless, it is noteworthy that most cases of Koro among women occurred during epidemic outbreaks. Indeed, there are very few case reports of sporadic Koro among women. 10 In non-Asian countries, individuals with Koro and their families often report that they have never heard about this syndrome or these symptoms nor had any contact with individuals from eastern countries. However, in this era of globalization, the possibility of exposure to syndromes that are specific to other cultures cannot be eliminated entirely.6,11
Koro is a relatively rare syndrome; according to Yap, only 19 cases of Koro had been reported in Hong Kong over a span of 15 years. 8 However, this syndrome can sometimes reach epidemic proportions: in Singapore, many cases were reported after an infection 12 ; in Thailand, a thousand cases were identified after the Vietnam War 13 ; and in Guangdong province, 2 similar outbreaks had occurred between 1984 and 1985 and in 1987, and approximately 2,000 cases were reported. 9 This syndrome has also been observed in India, a very different and culturally diverse society predominantly shaped by Hindu and Islamic cultures. 14 Koro has been sporadically reported in the United States, Great Britain, Canada, Greece, Jordan, Nigeria, Iran, Egypt, Sudan, Saudi Arabia, Jordan, and Oman.7,15–18 Furthermore, over the past 30 years, several cases of sporadic Koro attacks have also been reported among non-Asian patients (Table 3).
Koro Case Series With Patients of Non-Asian Origin
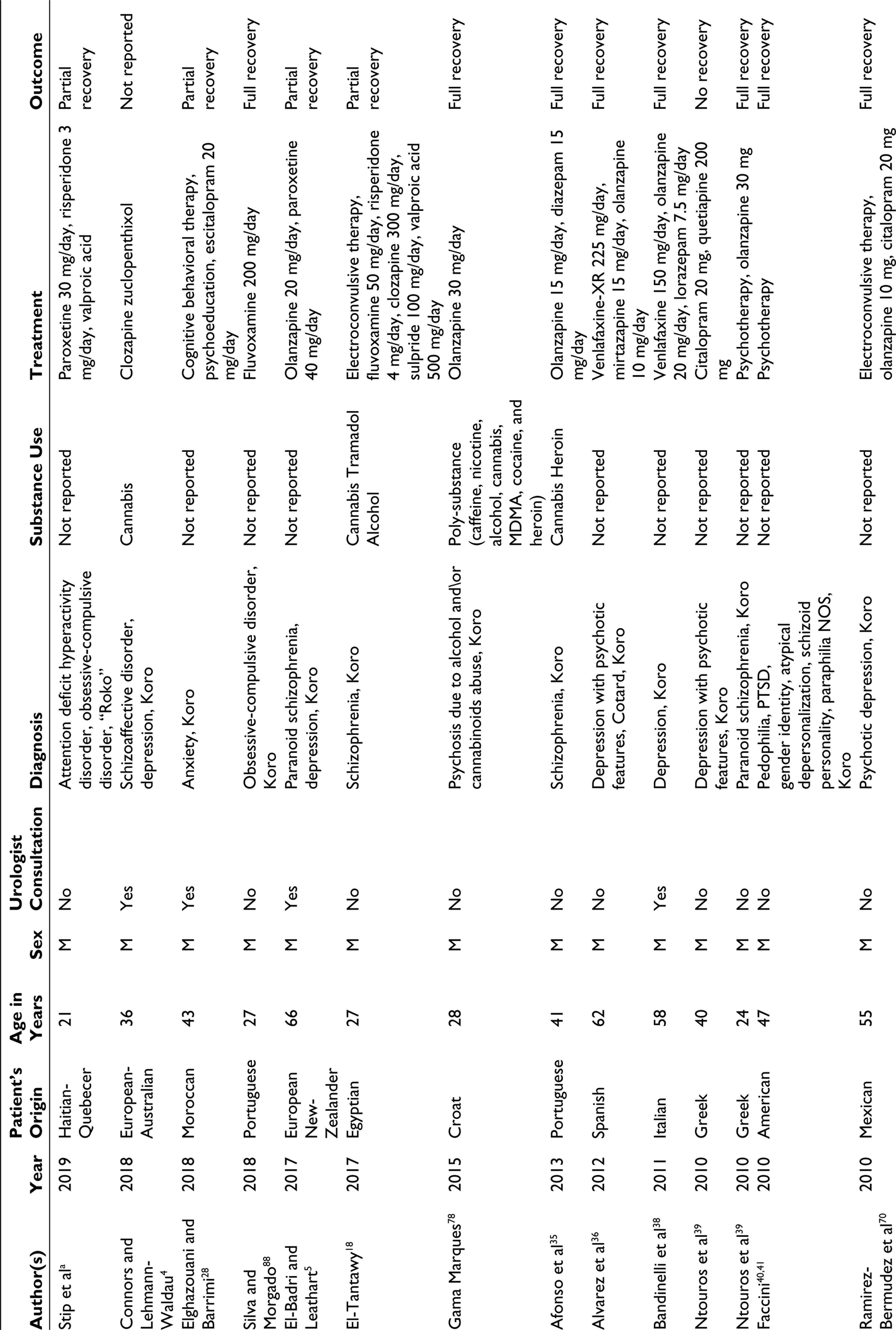
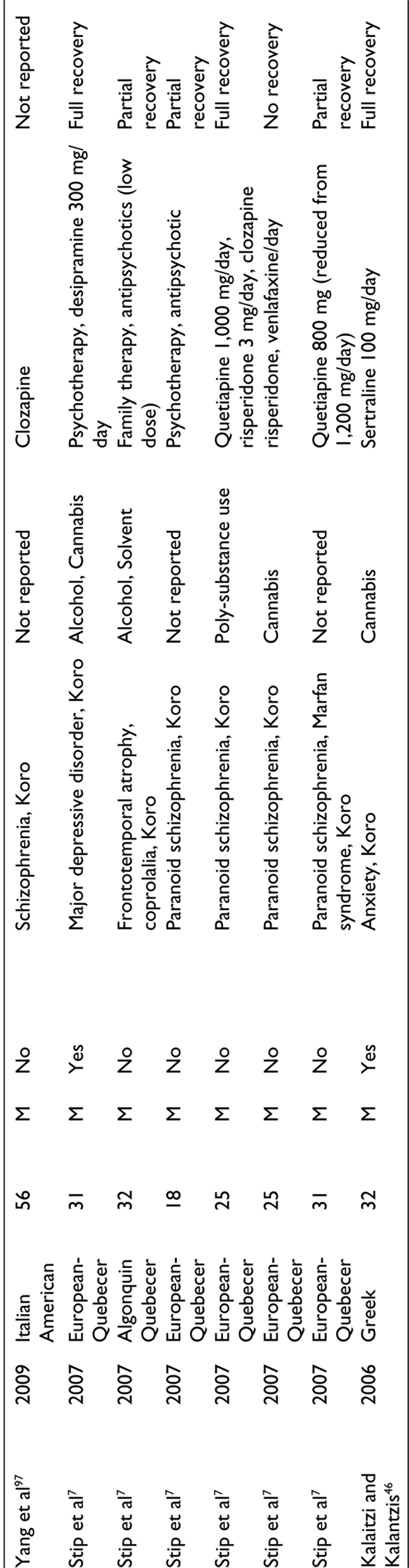
aData collected in the current clinical study.
Further, there have been more recent reports of epidemic outbreaks in China, India, Singapore, and Thailand.18–21 Thus, these findings underscore the importance of considering a patient’s cultural background when making a diagnosis. Moreover, this syndrome typically occurs in isolated cases and presents as a comorbidity of severe psychopathologies or cerebral lesions.22–24 Interestingly, Crozier has argued that classifying these syndromes as culture-bound diagnoses can hinder evidence-based treatment and result in stigmatization. 25 However, it is not clear why describing a syndrome as culture-bound is stigmatizing.
Koro is classified as an “other specified obsessive-compulsive and related disorder” in the Diagnostic and Statistics Manual of Mental Disorders, 5th Edition (DSM-5).26,27 Before the publication of the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10), Koro-like symptoms tended to be subsumed under other diagnoses, for example, delusional disorder.26–28 Furthermore, individuals with Koro symptoms often present without a clear history of psychosis or psychiatric illnesses.29,30 Some studies, however, have demonstrated a clear link with psychosis and other psychiatric disorders. Koro has also been observed in patients with schizophrenia, depression, obsessive-compulsive, body dysmorphic, somatoform, panic disorders, depersonalization, sexual disorders not otherwise specified, conversion reactions, poor intellectual functioning, and voyeuristic tendencies.4,14,31–34
In individuals with Koro-like syndromes and comorbid disorders, Koro-like symptoms can be chronic. Primary (either in sporadic or epidemic contexts) and secondary (in the presence of comorbid mental disorders) forms of Koro are distinguishable. For example, Haghshenas 16 identified a variant of Koro: a case of a 50-year-old individual with symptoms of Koro. He also had a comorbid condition, namely, Dhat, but did not fear the loss of semen. Dhat syndrome is typically characterized by a preoccupation with premature ejaculation or impotence and a fear that one is losing semen through the passage of urine. 17 Moreover, Koro-like syndromes can be conceptualized as nonspecific syndromes related to other psychiatric disorders (eg, anxiety, depression, schizophrenia, somatic conditions) and biological conditions (eg, urological diseases, brain tumors, other neurological diseases, mild cognitive impairment, Alzheimer).33–45 In a psychotic context, the retraction by evil or persecutors must be differentiated from the symptom of Koro, dynamic, sudden. In psychotic complaints, it is usually a slow or long process. 2
The onset of Koro is often associated with cannabis, alcohol, amphetamine intoxication, or heroin withdrawal.3,18,46 Even a one-time use of cannabis can induce a severely distressing mental health condition such as Koro. 47
Case Studies
In this section, a case series of 7 patients with Koro who had sought our consultation services in the province of Quebec in Canada is presented. Some case reports are translations or adaptations of our previously published findings (ie, in French). 7
The first case is a 26-year-old man of Lebanese origin who was initially admitted with an unspecified psychosis. He improved rapidly with aripiprazole and was discharged, but on follow-up a few months afterward, he presented again with similar psychotic symptoms, mainly auditory and somatic hallucinations, with persecutory delusions and a severe Koro syndrome. He previously trained as a pilot, but he was living at home with his mother at the time of his admission, working as a security guard. He had significant episodes of binge drinking in the past, which ended 1 year before the apparition of his symptoms. Otherwise, he does not take recreational drugs. During his admission, he spent 16 to 18 h per day playing video games online and interacted minimally with his copatients. He was initially cordial with the treating team but became suspicious as he believed the team was not treating his Koro syndrome and was actively involved in plotting to penetrate him or performing oral sex on him at night to reduce the size of his penis. This paranoia was compounded by an acute dystonic reaction to a neuroleptic injection for aggression and the unfortunate installation of a sound-level meter outside his window by the hospital, which he believed was used to record his auditory hallucinations. The urologist tried to reassure him. He was finally treated with long-acting antipsychotic medication and clozapine and became relatively stable.
The second patient initially consulted a urologist for premature ejaculation and subsequently consulted a sexologist. He was referred to psychiatry for exhibitionism. During the interview, he reported sexual tensions over the past 2 years: he had developed problems related to ejaculation and hypoerection, which had negatively affected his marriage. He subsequently experienced severe anxiety and fears pertaining to his genitalia; he believed his penis was shrinking and retracting into his abdomen. He was diagnosed with somatic delusional disorder, but he refused psychiatric treatment. Two years later, he presented with a depressive episode with no evidence of Koro symptoms and was successfully treated with antidepressant therapy.
The third patient was of First Nation origin (Algonquin) with a history of alcohol and solvent abuse. He had witnessed substantial promiscuity within his family since his early childhood. Over the past 3 years, his relatives reported that he had been exhibiting increasingly bizarre behaviors with periods of marked aggression and rambling, and disjointed discourse. He was admitted following a deterioration in his mental state. He was uncooperative toward the medical staff, and his reluctance appeared to be related to a systematized delusion of persecution. During his hospitalization, he continued to soliloquize; this was accompanied by coprolalia and animal vocalizations. Eventually, the patient disclosed that he had been in love with his brother, with whom he had had sexual intercourse. His delusional belief that his penis was retracting resulted in peculiar behaviors; for example, using laces or strings, he pulled on his penis to prevent it from shortening and retracting into his abdomen, and regularly masturbated to avoid this retraction. A computed tomography scan revealed frontotemporal atrophy, and he was diagnosed with an organic brain syndrome. Unfortunately, the patient’s condition did not improve, and his symptoms of social withdrawal and sexual preoccupations persisted.
The fourth patient had been diagnosed with paranoid schizophrenia 3 years earlier. He had been referred to our First episode psychosis program for specialized psychosocial rehabilitation. His childhood was characterized by persistent family conflict and abuse. Following a romantic breakup at the age of 16, he adopted misogynistic beliefs and became very shy around women. Unable to build satisfying relationships with women, he developed a behavioral addiction to masturbation and frequently visited a commercial sex worker. Furthermore, the sight of sexual material triggered aggressive crises, including threats directed toward his mother. He eventually revealed his fear of losing his penis: “It is like a piece of ice under the roof; it melts in the heat, and it will disappear.” Only masturbation and the services of a sex worker were able to reassure him and preserve the entirety of his genitalia. An atypical antipsychotic was prescribed; it yielded mediocre results and was unsuccessful in controlling his delusional symptoms.
The fifth patient presented himself to our emergency room with suicidal ideations and claimed to be “sexologically disturbed.” He requested medication that could treat his genitals. This patient had been diagnosed with schizophrenia at the age of 16 and had a history of polysubstance use (heroin, cocaine, and solvents). Upon examination, he was anxious and experienced olfactory (genital odors), auditory, and visual hallucinations. He reported that he had suffered a “rape of his brain” and added that his penis was retracting into his abdomen. The culmination of this process would eventually force him to commit suicide. These typical Koro-like symptoms were part of a somatic delusion, whereby the patient believed that he was being transformed into a woman. Prior, he had suffered from premature ejaculations during his heterosexual encounters. Subsequently, he had avoided closeness with women and declared that he was a gay man. Even after 1 week of hospitalization, his delusions and severe thought disturbances persisted. Clozapine was reintroduced because he had responded well to this treatment in the past.
The sixth patient initially presented himself to our ward with persecutory auditory hallucinations. He also reported mystical and persecutory delusions such as a fear of “getting [his] penis magically removed.” He had previously disclosed that his father had physically abused him and sexually abused his sister. A month after hospitalization, he articulated how much he dreaded what the voices were predicting (ie, he would lose his genitals) during an interview. This was often accompanied by the paranoid belief that his genitals were being suctioned into his body, which he attributed to a satanic spell. He, therefore, held his penis with his hands to prevent his genitalia from being pulled in and regularly examined his penis. He developed an irrefutable belief that the invagination of his genitals would ultimately lead to his death: “It is impossible to live without one’s sexual organ.” His delusions did not respond to treatment.
The seventh patient had been referred to the hospital’s emergency department because of suicidal ideation. The patient had treatment-resistant schizophrenia, for which he had been admitted to the psychiatric ward over 20 times. He was also known for Marfan syndrome. His current symptoms differed from previous hospitalizations for persecutory delusions, auditory hallucinations, and, occasionally, suicidal ideation or behavioral disorders. The voices in his head had become coercive, commanding him to commit suicide, and predicted that his penis and testicles would disappear. He became obsessed with this idea and constantly checked the dimensions of his penis. He often masturbated to measure the size of his erect penis. He experienced significant shame about his condition; therefore, he maintained a distance from others and had trouble talking about it. Following treatment, he was almost asymptomatic; he rarely had auditory hallucinations or thoughts of genital invagination.
Classification and Diagnostic Associations
This literature review revealed that Koro could be described as either an independent psychopathological phenomenon or a manifestation of primary pathology. 2 This is primarily reminiscent of Kraepelin’s conceptualization of hypochondriasis, followed by depressive (Cotard delusion), anxiety (panic disorder), and psychotic disorders (schizophrenia), and some organic brain syndromes (eg, tumor, epilepsy, syphilis).
Over the last century, Koro has evolved from a culture-bound condition into a globally prevalent pathology. However, consensus about its classification within the DSM or ICD has not yet been reached. Consistent with the cultural perspective, Yap 8 has described Koro as a culture-bound syndrome that entails depersonalization. However, Hughes 48 has recommended its inclusion in the diagnostic criteria for somatoform disorders. According to Edwards, 49 Koro can be classified as a genital retraction panic disorder. Bernstein and Gaw 50 reviewed past attempts to define and classify Koro and presented it as a new diagnosis that should be included in the DSM-IV. Unfortunately, however, this had no effect on the nosology of the DSM-IV. Nevertheless, the DSM-5 classifies Koro as an “other specified obsessive-compulsive and related disorder,” specifically in relation to Dhat. Given the evolution of its classification, both conceptual and descriptive inadequacies are found in the DSM’s definition; therefore, there is a need for further debate about what constitutes an “exotic deviance”.8,46,51–59
Etiologies, Formulation, and Models
Koro has been described as a condition that is caused by the devil, especially in Southeast Asia. Indeed, past studies have shown that laypeople implicitly believe that Koro is a state of demonic possession. Furthermore, it is traditionally believed that the spirit of the dead, which does not have a penis, may disguise itself to steal the penis of a living man. Several hypotheses have been developed in accordance with major explanatory models within the field of psychiatry.60,61
Body image is an integral component of one’s self-concept. The genital organs are associated with one’s gender identity, and abnormal perceptions of one’s genital organs can lead to body integrity identity disorder. From a psychodynamic perspective, Koro raises questions about the sexual ambiguity that results from invagination (ie, the penis is transformed in such a way that it resembles female sex organs). Notably, in the Celebes Islands, where this syndrome was first described, transvestite priests and healers can be commonly found. Moreover, in the third clinical case that has been reported in this article, the emergence of Koro was associated with homosexual practices; further, the patient disclosed that he had engaged in sexual activity with his brother, with whom he had also been in love. In contrast, the fifth case raises the issue of transsexuality (ie, the patient believed that he was being transformed into a woman). Meanwhile, Rin 62 has explained that, in the Chinese version of Koro (ie, suoyang), the fear of a disappearing penis is related to a broader fear of losing vitality, which is associated with the “yang” (which represents masculinity, firmness, and force). Furthermore, according to a popular Chinese belief, masturbation and wet dreams (ie, in contrast to sex with a partner, which allows a healthy exchange of the yin and yang) lead to a waste of sperm, which is a source of energy.
Concordantly, Rin has identified the absence of paternal models (which are conducive to identification), a high frequency of masturbatory behaviors, and confusion regarding one’s sense of masculinity as potential explanations for the development of Koro. 62 Moreover, Koro can be conceptualized as a manifestation of the anxiety associated with the challenges involved in becoming a strong male figure and the fear of not being able to do so; this explains why many patients develop this syndrome during early adulthood.
From a psychodynamic perspective, Koro can be conceptualized as a condition that is associated with castration anxiety. However, Kobler 63 has articulated four reasons, which support the contention that Koro is not a manifestation of typical castration anxiety. First, there is no symbolization of the phallus in Koro (ie, a man is afraid of losing his penis, not the eyes or any other part of his body). Second, there is no clearly identifiable castrator. Third, instead of camouflaging his penis, an individual with Koro may expose his penis to others and sometimes even ask a relative to hold it; this behavior is indicative of a relative absence of the fear of possible castration. Finally, in complete Koro, intense anxiety stems from the fear of death, not the fear of potential loss of the penis.
In contradistinction to classic castration anxiety, wherein the threat of loss of one’s penis originates from an external forbidding authority, in individuals with Koro, this threat stems from within. Accordingly, castration anxiety is more closely related to a threat to one’s integrity and the fear of losing a sense of self, resulting in excessive guilt or self-punishment in response to this conflict. Freud has noted that “already in childhood the penis is the leading erotogenic zone and the chief auto-erotic object, and the boy’s estimate of its value is logically reflected in his inability to imagine a person like himself is without this essential constituent.”64,65 Furthermore, Lacan has made the following observations: “For these objects, whether part-objects or not, but certainly signifying objects—the breast, excrement, and the phallus—are no doubt won or lost by the subject.”66,67 Similar to Cotard syndrome,68–70 in Koro, the negation of a vital body part symbolizes the negation of the subject.
Thus, the loss of the phallus, which is a symbol of power and virility, will result in a complete collapse of narcissism; hence, this belief may evoke extreme anxiety. As Sims 71 has observed, narcissism entails a fear of imminent threat to one’s body integrity rather than a distorted view of one’s body, which is the case in individuals with dysmorphophobia. This fear leads to desperate attempts to preserve body integrity. In the patient with Marfan syndrome, a preoccupation with the length of certain parts of his body (eg, his fingers), a semiological element inherent to this genetic syndrome, is easily observable.
Other scholars have delineated the psychophysiological origins of Koro, specifically concerning its size and form. Yap 8 has emphasized that concrete experience of the narrowing of the penis during cold weather is a trigger for Koro. Thus, normal changes in the size of the penis may draw excessive attention from an individual who is easily emotionally aroused and sensitive. 72 Current understandings of Koro have been enriched by cognitive and neurophysiological models. Brain lesions, including a right temporoparietal ischemic vascular accident, 73 and a tumor of the corpus callosum 74 have been reported. Relying on electrophysiological methods, Joseph 75 attempted to draw associations between episodes of Koro experienced by 2 patients and a form of complex partial epilepsy of temporal lobe origin, which they had been diagnosed with. The rationale that underlay Joseph’s hypothesis was grounded in the role of (a) temporal lobes in body image perception and (b) the limbic system and neocortical zones in the integration of sensory information processing. 76 Temporal lobe disturbances have also been observed in individuals with other psychiatric disorders (eg, schizophrenia). Incidentally, 4 of the 7 patients whose case reports have been documented in our case series had schizophrenia. The neurophysiological abnormalities specific to this pathology appear to serve as a fertile ground for the onset of Koro, especially in individuals with internal conflicts regarding sexuality and their sense of masculinity.
In addition, Chowdhury 77 examined the perceptual distortions that underlie the organ representations of patients with Koro. Chowdhury conducted a drawing test, whereby his patients were required to draw their penises. The results revealed that when compared to the control group, patients with Koro not only perceived their penises to be shorter and narrower but also more easily detachable (ie, a solid line connected both sides of the organ at its base).
The brain mechanisms that contribute to the subjective perception of penis retraction are yet to be identified. Koro has been compared to Capgras and Othello syndromes as a right frontotemporal impairment. 78 The right hemisphere is involved in the ability to relate to the internal and external world, self-monitoring, and other behavioral dysfunctions. In patients with Capgras or Othello syndrome, the left hemisphere creates an interpretation of the world founded upon false evidence, thereby causing an individual to draw fallacious conclusions.79–81
Treatment
Treatments primarily target the underlying psychopathologies through pharmacological means and by providing psychotherapeutic support; these strategies have yielded variable outcomes. 82 Pharmacological treatments primarily target the underlying psychiatric disorders (eg, using selective serotonin reuptake inhibitors, selective serotonin reuptake inhibitors [SSRIs]). 83 Antipsychotic medications can alleviate the symptoms of psychosis and mood disorders. In individuals with underlying psychotic disorders, the treatment of sporadic Koro depends on its etiology and the effectiveness of antipsychotics in controlling the associated psychotic features. Electroconvulsive therapy has also been used to treat a sporadic case of schizophrenia with Koro, 20 but evidence about its effectiveness in treating Koro is limited. Finally, Koro appears to be responsive to psychoeducation and interventions that provide reassurance.84,85 Evidently, further research is needed to understand the development of Koro-like symptoms, which have been observed in individuals with schizophrenia.
In conclusion, an analysis of our case series and other case reports (Table 2) revealed that, out of a total of 42 patients, 28.6% (n = 12) had received antipsychotic medication without antidepressants; a positive outcome was observed in 7 patients. A total of 23.8% (n = 10) of the patients received an antidepressant without antipsychotics (response rate = 80%, n = 8), and 4 of them received only SSRIs. Further, 33.3% (n = 14) of the patients were treated with both antipsychotic and antidepressant drugs, and 3 of them received an additional mood stabilizer. Benzodiazepines were a common adjunct to treatment; 9 patients had been treated with additional anxiolytics, whereas 4 patients had been treated with only benzodiazepines. Psychotherapy was also provided to 12 patients, either alone (n = 3) or as an adjunct to pharmacotherapy.
The Debate About Cultural Universals
Koro is often described as an epidemic that is localized within Asia. However, Koro-like syndrome has also be observed in isolated cases in Quebec (as demonstrated by our case series). The fear of a disappearing penis has been reported worldwide. 16 The symptom cluster characteristic of Koro is not culture-bound because it has been observed within non-Asian populations.5,18,30,86–88 Consequently, the aspects of epidemic presentations that correspond to a very culturally specific phenomenon may be distinguishable from isolated cases related to other conditions.89,90 In this context, we must better highlight the potential differences between the real Koro syndrome and a collection of beliefs related to the perception or delusion of penile retraction in other codable psychiatric disorders.
Because clinical approaches have remained virtually unchanged, the following question gains salience: what do we (ie, clinicians) need to do to improve the diagnosis and management of Koro? Creating greater awareness about Koro and developing better diagnostic tools or related clinical assessments partially answer this question. Indeed, clinical approaches should remain focused on individual differences and the phenomenological aspects of this disorder.
Koro Versus Body Dysmorphic Disorder
Several parallels can be drawn between body dysmorphic disorder (BDD) and Koro, especially chronic Koro-like syndrome. Deepening our understanding of these psychiatric conditions will facilitate delineating the typical characteristics of pertinent sociocultural influences and the many core features of their clinical presentations. Furthermore, a central feature of Koro is distorted perceptions of one’s own body parts (notably, the genitals); these disturbances are neither unique nor limited to this syndrome. 91 For example, some authors found that, over time, patients with Koro consistently perceived their penises to be increasingly smaller than their actual sizes.92,93 This finding is similar to what is typically observed in patients with BDD.
Koro has traditionally been associated with the misperception of genital organs. However, in the literature, Koro has also been described as a condition that can involve other body parts (eg, nose, ears, tongue); this characterization is more closely associated with BDD. 94 Interestingly, some authors have unified Koro and BDD into a singular condition and postulated that they both describe different severities of the same semiological entity along a continuous spectrum. Accordingly, Koro-like syndrome can be regarded as a severe manifestation of BDD, whereby body image disturbances are accompanied by not only anxiety and repetitive behaviors but also somatic distortions, which can lead a person to believe that his/her body parts are actually changing. 94 Another characteristic of BDD, which is a hallmark feature of Koro, is intense anxiety and the distress that results from perceptual disturbances. Such distress can be manifested as panic attacks, which are attributable to the disorder. 16 The presence of BDD-cued panic attacks is associated with more severe BDD presentations, social anxiety, depression, and poorer functioning and quality of life. Severe BDD can cause delusions about one’s body; these symptoms are akin to the psychotic disorders that have been associated with Koro-like syndrome. 94
Patients with BDD may seek reassurance by looking at their penises, measuring their length, comparing them to those of naked men in magazines or on the Internet, using objects to increase the size of their penises, and asking for direct reassurance from their peers. 94 Moreover, Koro can result in the exhibition of behaviors that are believed to prevent the retraction of genitals, using various devices that can be attached to the penis. 95 Although there are similarities between the 2 conditions, some behaviors (eg, grasping the genitals, asking relatives for assistance) are unique to Koro. 91
Individuals with BDD who have concerns about penis size believe that their penis is shorter than what others expect or demand it to be, resulting in fear of punishment from others. 96 Individuals with Koro also experience this fear of punishment; indeed, fear of retraction of the penis into the abdomen may represent anxiety about a type of symbolic castration, which can result in a loss of power.90,91
In individuals with Koro-like syndrome, the temporal stability of perceptual concerns about penis size may be an expression of unconscious conflicts about their sense of masculinity and sexuality. Specifically, male patients who are preoccupied with their penis size may experience distress in their relationships and sexual encounters; consequently, they may avoid such situations. 95 The development of Koro, Koro-like syndrome, and BDD has been hypothesized to be influenced by the importance that society ascribes to specific body parts that symbolize masculinity (eg, penis, muscles).69,96,97
Conclusions
Overall, the present findings highlight the need for appropriate measures of the symptoms of Koro and treatment outcomes. The illusion of penile shortening in psychosis is an example of secondary Koro. 98 In the very inspiring article from Chowdhury and Brahma, 2 the authors caution us not to automatically mix true Koro syndrome with secondary or comorbid Koro. The fact that we are North American clinicians, therefore more distant from Asian culture, our understanding of what we have described in our series of cases is strongly informed by these authors’ advice. 2 Moreover, we join their warnings. Therefore, in the psychotic context, the illusion of the dissolution of the penis by a malicious force or a complex matter of envy of another person must also be carefully differentiated from the symptom of Koro. In Koro, penile retraction is a dynamic phenomenon. It is described with suddenness and rapidity. Conversely, in delusional disorder such as somatic type, it is usually a slow or long process with a different cognitive component. Detailed sexual history remains essential in examining the role of psychosexual dysfunction, guilt, or trauma in the genesis of bizarre perception of penile morphology. Consequently, the authors advise us to respect the Koro phenomenology and diagnostic criteria, which are already precise, without any other clinical contamination.
We agree with this distinction between the secondary Koro and the primary Koro. The association of schizophrenia, affective disorders, medical conditions, and substance use disorder with Koro has been reported and discussed in more recent articles. The perception of the penis within dysmorphophobia deserves to be better clarified in the drug addict population, for instance, with cannabis. Comorbidity with Koro is an interesting and growing area of research, and therefore every researcher should be vigilant not to miss this clinical opportunity. The dialogue between clinicians from different cultures is a great opportunity. However, the question remains: how many of us clinicians really ask the question during our interviews with patients in the emergency room or in the office: do you feel that your penis has shrunk? Are you worried about this?94,95 There is a lack of data on this clinical competency.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.