
Abstract
The persistent disparity in orgasm frequency between cisgender men and women during heterosexual intercourse—termed the “orgasm gap”—reflects not only physiological but also deeply embedded sociocultural dynamics. Several researchers use the term orgasm gap primarily for orgasm difficulties originating from cultural issues, whereas other researchers also use this term for broader use. Reduced orgasm frequency leads to poor sexual satisfaction, decreased desire to engage in sexual relationships and several other adverse consequences for women. Sociocultural changes happening around the world, resulting in improving women’s rights, education, independence, awareness related to sexual issues, public discourse and media representation, as well as rapidly improved scientific understanding, are influencing issues related to the orgasm gap. Against this backdrop of advancing gender equity, increasing sexual literacy, and expanding scientific inquiry, the conversation around female sexual pleasure is evolving. Efforts to address the orgasm gap now encompass media representation, educational outreach like easy availability of information and resources in books and websites, and the integration of evidence-based clinical approaches. This narrative review synthesizes current scientific findings, sociocultural narratives, and technological developments, equipping clinicians with comprehensive, context as well as culturally sensitive strategies for helping females with orgasmic difficulties.
Introduction
Sexual behavior, while evolutionary in origin—serving reproductive and survival functions—plays a far broader role in modern human life, profoundly influencing both physical and psychological well-being. 1 Both physical and psychological health are positively influenced by regular sexual activity, making it vital for physicians and healthcare professionals to understand the functioning underlying sexual behavior. A substantial amount of research has been done to find out the contributors to female and male orgasm. Additionally, scientific information regarding female sexual functioning is rapidly improving, and scientific advances continue to unravel the neurobiological, psychological, and sociocultural dimensions of female sexual function, underscoring its complexity. Sociocultural ideas often influence science and its trajectory. Sociocultural forces have influenced the scientific discourse related to female sexuality. Female sexuality passed through various phases of complete denial, misrepresentations, blame, apprehensive spectating, distortions, to radical acceptance of science-based reality. 1
Emily Nagoski, in her seminal work Come as you are 2 defines orgasm as Orgasm is the sudden, involuntary release of sexual tension. It may or may not include pelvic floor muscle contraction, intense pleasure and sensation of doneness, heightened emotional experience, increased genital sensitivity or other marked changes, usually after high sexual arousal. Orgasm is an important facet of sexual intercourse and significantly influences the perception of sexual pleasure, fulfillment, and sexual quality of life of an individual. Overall, increased levels of sexual and relational satisfaction have been reported in study3,4 by women who experience orgasm more frequently. Nevertheless, research data consistently report that women in heterosexual relationships experience a lesser number of orgasms in comparison to their male partners. Hence, this outcome that cisgender men usually have more orgasms than cisgender women during heterosexual partnered sex is defined as “orgasm gap” in literature. 4 Several researchers use the term orgasm gap primarily for orgasm difficulties originating from cultural issues, whereas other researchers use this term for broader use also.
Several popular magazines, press articles, and media articles also reported differences in consistency in the orgasm of men and women during heterosexual intercourse resulting into popularizing the previously unexplored concept among the general public. Reduced orgasm frequency leads to poor sexual satisfaction, and reduced desire to engage in sexual relationships and also has several other adverse consequences for women. Sociocultural changes happening around the world are resulting in improved women’s rights, education, independence and awareness, as well as shaping the conversation, public discourse and media representation of issues related to the orgasm gap.
This narrative review seeks to address the question of how evolving scientific understanding and sociocultural shifts surrounding female sexual functioning, orgasm gap in particular, can inform clinicians in their assessment and management of female orgasmic difficulties. The objective is to integrate contemporary scientific knowledge, existing psychological theories, sociocultural perspectives, and technological developments related to the orgasm gap in heterosexual women.
The review aims to enhance clinicians’ understanding of this multifactorial issue and prepare them with nuanced, context-sensitive, and evidence-informed approaches to assessment and intervention.
Methodology
The review did not have an exhaustive, systematic data collection. It was the purposeful and integrative selection of literature that contributed to a broader understanding of the orgasm gap from different perspectives from databases, primarily PubMed and Crossref using the terms: “orgasm gap,” “female orgasmic disorder,” “anorgasmia,” “female sexual dysfunction,” “sexual script theory,” “heterosexual sexual behavior,” “clitoral stimulation,” “cultural influences on sexuality,” “CBT for sexual dysfunction,” “technological tools for sexual education.”
Peer-reviewed journal articles, major population surveys, meta-analyses, narrative reviews and relevant books on clinical practice, sociocultural theory, and sexuality were included, along with quantitative and qualitative studies, as well as emerging trends, for example, OMGYES, podcasts, apps relevant to patient education and clinician awareness. The management section predominantly emphasizes non-pharmacological strategies, with only limited consideration given to pharmacological agents. A comprehensive discussion of pharmacological treatments is not included
Sexual Functioning: Factors Influencing Sexual Functioning
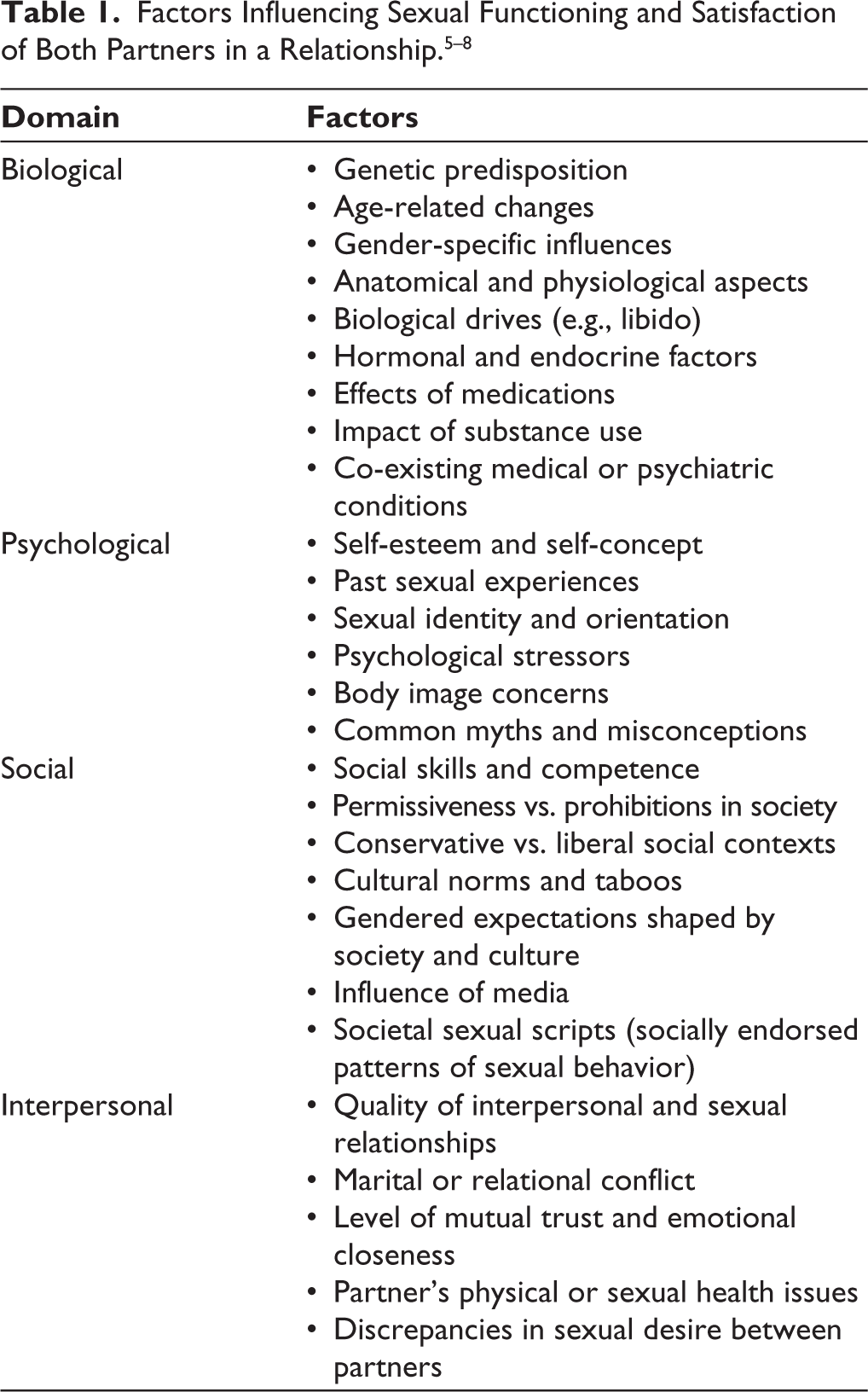
Disparities in orgasm frequency between men and women have long been recognized. However, despite this growing awareness, clinicians seem to be relatively unaware of the possible strategies required in handling clients’ issues adequately. Sexual functioning, satisfaction, and their influence on the quality of life are affected by several factors (Table 1).
Biological Factors
Various biological factors are at play when it comes to understanding the elusive mechanism of sexual behavior and responses in males and females. Central neurochemical system, namely, dopaminergic and serotonergic systems, appear to play a significant role in desire, arousal and orgasm. Sexual response intricately depends on the interaction among the endocrine, nervous and genetic factors. Although males and females share similar neural mechanisms underpinning sexual functioning, the expression of sexual responses differs significantly. The classical model proposed by Masters and Johnson delineates sexual response into four phases: excitement, plateau, orgasm, and resolution. 10 Kaplan later introduced a clinically oriented triphasic model—desire, excitement, and orgasm 11 —which offers enhanced applicability in therapeutic contexts.
A twin study explored the apparent genetic influence on female orgasmic dysfunction. 9 The data clearly demonstrates a significant genetic contribution to the difficulty in achieving orgasm. Finding suggests the heritability of difficulty reaching orgasm was at 34% during intercourse and 45% during masturbation. Therefore, this indicates that variations in female orgasmic dysfunction have genetic roots as well and are not solely influenced by cultural factors.
Psychological Factors
Psychological factors like body image, self-esteem, life stressors, sexual identity, sexual orientation and misconceptions have significant effects on the occurrence and dysfunctions of sexual functioning. A study by Carlos, Juan and Perez 10 analyzed a rarely studied psychological construct, subjective orgasm experience (SOE), in the sexual contexts 11 of relationships and solitary masturbation in 179 heterosexual and homosexual couples. SOE refers to the perception, sensation and/or evaluation of orgasm plays a significant role in sexual functioning. Among the findings, the study revealed that the intensity of partners’ orgasm experience during solitary masturbation had an influence on the intensity of SOE during sexual relationships, with variation observed based on the type of couple, heterosexual and homosexual.
Studies12,13 exploring cognitive-affective aspects that are involved in the development, progression and maintenance of sexual difficulties. The results showed that women experiencing sexual difficulties had more negative automatic thoughts during sexual activity. These thoughts centered around failure and disengagement, sexual abuse, lack of affection from their partner, passivity, negative body image, and fewer erotic thoughts.
In a recent publication by Cerwanka et al., 14 researchers analyzed data from the German Health and Sexuality Survey (GeSiD) to explore sexual practices, frequency of sexual activity and masturbation, relationship satisfaction, feelings of love and closeness, and general sexual satisfaction. The study included responses from 1,641 sexually active women in heterosexual relationships, aged 18–75, who reported their experience of orgasm during their most recent sexual encounter. The findings indicated that sexual activity frequency, relationship satisfaction, feelings of love and intimacy were strongly correlated with each other and were individually associated with a higher likelihood of experiencing orgasm. These findings underscore the interconnected nature of relational and emotional factors in shaping orgasmic outcomes in women.
A study conducted by Hite 15 reported that women have more orgasms when they engage in sex with other women, and also while masturbating. Similarly, according to a Portuguese convenience sample of 3,687 women, 92.3% were able to achieve orgasm while masturbating. 16 Another US study 17 was conducted to examine the frequency of orgasms among individuals of different sexual orientations. The study gathered data from 6,151 men and women, aged 21 to 65+, in the United States. Results were obtained from a subset of 2,850 singles (1,497 men and 1,353 women) who had engaged in sexual activities within the previous 12 months. The findings revealed that for men, the average occurrence rate of orgasm did not vary significantly across sexual orientations (heterosexual men 85.5%, gay men 84.7%, bisexual men 77.6%). Conversely, among women, the mean occurrence rate of orgasm varied notably by sexual orientation (heterosexual women 61.6%, lesbian women 74.7%, and bisexual women 58.0%). It was found that homosexual women had a significantly higher likelihood of experiencing orgasms compared to heterosexual or bisexual women.
A similar study by Frederick et al., 18 involving 52,288 participants of various sexual orientations, revealed that heterosexual men exhibited the highest likelihood of experiencing orgasms during sexual intimacy (95%), followed by homosexual men (89%) and bisexual men (88%). Among women, lesbian individuals reported the highest frequency of orgasms (86%), followed by bisexual women (66%) and heterosexual women (65%). These data highlight how sexual orientation and behavioral context can impact female orgasmic frequency.
Social Factors
The concept of “sexual scripts” provides a useful framework for understanding how social behavior, including sexual behavior, is shaped and enacted. Three distinct levels are examined while scripting the sexual behavior: Sexual scripts operate at three distinct levels: (a) cultural scenarios, which define shared meanings and societal expectations; (b) interpersonal scripts, which guide interactions within specific relational contexts; and (c) intrapsychic scripts, which encompass the internalized desires and motivations of the individual.19,20
Cultural script may play an important role as a contributing factor in the orgasm gap in the absence or lack of relevant biological, psychological or interpersonal dysfunctions. Traditional narratives around heterosexual sex often prioritize male-dominated, limited foreplay, penile-vaginal intercourse and male erection/ejaculation, reinforcing the notion that men are the primary agents of women’s orgasm. Concepts such as men are the exclusive dispenser of orgasm in women, and the essentiality of penile functioning in women’s pleasure are largely influenced by cultural script as well as sexual knowledge, education and attitude of the persons involved in sexual relationships. In this cultural script, penetration is the main focus of sexual intercourse, and female orgasm can potentially be improved by lasting long, hard and deep thrusting of penis inside vagina. The women who are unable to experience adequate sexual stimulation during this process are unable to achieve orgasm. Due to limitations imposed by cultural scripts, men and women may shy away from experimenting with alternative ways of giving/receiving pleasure during sexual intercourse. Therefore, cultural script also influences the level of active involvement of females during a sexual act. Cultural prohibitions on female sexuality lead to females maintaining a passive role during sexual intercourse, and often they are not allowed/encouraged to freely speak or express their likes, dislikes and choices, etc., resulting in insufficient pleasure during sexual intercourse. Males often endorse and approve of this female behavior due to cultural conditioning promoting females having a lesser interest/involvement in sexual acts. Such cultural messaging limits both partners’ understanding of female pleasure and contributes to rigid, heteronormative expectations around performance and satisfaction.
Heterosexual sexual script often deprioritizes women’s sexual pleasure and orgasm. This narrow focus frequently overlooks the importance of sufficient clitoral stimulation and diverse sexual practices. Gusakova et al., 21 have shown that women who actively pursue orgasm during sexual intercourse have better chances of having an orgasm during sexual activity. However, many women do not actively pursue orgasm during intercourse due to various reasons related to motivation, shyness, lifestyle-related situations, relationship status, restrictions imposed by cultural script, simple unawareness or conditioned to prioritize male pleasure. This non-pursuance significantly impacts their chances of experiencing orgasm.
Clinicians need to recognize that not all women have an equal pursuit of orgasm during intercourse. This individual difference can significantly impact the occurrence of orgasm in women. A study 22 investigated the effects of the orgasm gap on various sexual outcomes for couples, such as desire and expectation for orgasm, revealed that a woman’s frequency of orgasm predicts a man’s expectation of orgasm. This dynamic may contribute to a self-reinforcing cycle: as women experience orgasms less frequently, they begin to expect and value them less, further entrenching the orgasm gap. These findings emphasize the need for clinicians to explore expectations and relational dynamics when addressing orgasmic difficulties.
Males attain orgasm (penetration) in a different way a women reach orgasm, and this is not yet known to a large percentage of individuals and even clinicians. Many individuals—and even healthcare providers—continue to hold outdated beliefs about the mechanisms of female orgasm, underscoring the urgent need for updated education and training.
During heterosexual encounters, men are no longer considered an exclusive dispenser of orgasm to women, but they are considered enabling partners to facilitate mutual pleasure and allow women to explore, pursue and enjoy orgasmic pleasure. 1 This shift toward mutuality and shared responsibility is key to bridging the orgasm gap and fostering fulfilling sexual relationships.
The cultural representation of women is changing. The women are poised to play an important and dominant role in their lives, including their sexual experiences. The current science is helping clinicians to be more at ease, freeing them from cultural connotations of orgasm and female sexual pleasure. A more objective view is possible. These developments—fueled by feminist movements, human rights advocacy, and calls for gender equity—are enabling a more objective, inclusive, and evidence-informed approach to female sexual health.
Interpersonal Factors
Interpersonal dynamics play a critical role in the manifestation and maintenance of sexual difficulties within relationships. Sexual difficulties can stem from problematic relationships or, conversely, they may lead to relationship dissatisfaction. Determining the course of this causality can be challenging, as couples may be at different stages of relationship satisfaction and may have varying definitions of differing definitions of intimacy, satisfaction, and sexual health. 23
Research indicates that addressing both relationship and sexual issues simultaneously may lead to more promising long-term outcomes compared to treating them distinctly. While most studies in this area are observational rather than randomized controlled trials, they consistently highlight a strong interdependence between relationship quality and sexual functioning.
Love and intimacy are vital for sexual and relational satisfaction and should be assessed and addressed during couples therapy. Emotional closeness is frequently associated with enhanced sexual pleasure and a more fulfilling partnership. Therefore, clinical interventions that target sexual dysfunction in isolation, without addressing underlying relational dynamics, may be insufficient for achieving lasting improvements.
Female Orgasmic Dysfunction
DSM-5 24 and other important diagnostic criteria systems are now agreeing to the fact that failure to experience orgasm during intercourse in the absence of additional clitoral stimulation is not considered an illness.25,26 This may be a normal variation in sexual functioning due to inadequate sexual stimulation. Although due to less stringent criteria and inclusion of lack of knowledge as part of the diagnostic category, ICD-11 can diagnose women in the above situation as having orgasmic dysfunction.
The second most frequently reported women’s sexual problem is Female Orgasmic Disorder (FOD) or Anorgasmia. The condition is characterized by the lack, delay, rarity, or significant decrease in intensity of orgasm in at least 75% of sexual experiences. This must persist for a minimum of 6 months and cause distress. FOD has subtypes, such as primary and secondary anorgasmia. It impacts up to 28% of women in the US and up to 46% in various Asian countries. 27 In DSM-5 Female Sexual Interest/Arousal Disorder (FSIAD) is the sexual dysfunction which is diagnosed when there is ‘reduced or no interest in sexual activity, few or no thought about sex, decreased sexual arousal or pleasure during sexual activity, no or reduced arousal response to different sexual cues (visual, written or verbal cues), infrequent or initiation in sexual relationship and reduced sensation in the genitals’ for the period of six months and at least 75% of time. The conceptualization of female orgasm has evolved significantly over time. In early psychoanalytic theory, notably that of Sigmund Freud, vaginal orgasm was viewed as the hallmark of “mature” female sexuality, while clitoral stimulation was dismissed as infantile or deviant. This pathologizing view has since been refuted by sex researchers, including Alfred Kinsey, William Masters, and Virginia Johnson, who demonstrated that orgasms are psychologically and physiologically identical regardless of the mode of stimulation. 28 Shere Hite’s seminal work, The Hite Report, challenged dominant assumptions about female sexuality by collecting the narratives of hundreds of women through detailed questionnaires. Her findings emphasized the diversity of orgasmic experiences and the importance of self-exploration and non- penetrative stimulation. 18
To date, pharmacological treatments—including granisetron, bupropion, and sildenafil—have not demonstrated efficacy beyond placebo in enhancing orgasmic function in women with FOD. Cognitive-Behavioral Therapy (CBT) for anorgasmia has been shown to effectively alter attitudes, reduce anxiety, and address sexually-related thoughts. Additionally, behavioral techniques 29 such as directed masturbation, sensate focus, and systematic desensitization, along with sex education, 30 communication skills training, and Kegel exercises, have also been successful in treating this disorder.
Physiological, Neural and Hormonal Correlates of Orgasm and Possible Causes of Impairment
It is essential to recognize the critical roles of neurobiology, hormones, emotional context, and individual temperament in shaping sexual behavior and orgasmic response. Human sexual functioning involves both autonomic and voluntary systems and is modulated by an interplay of biological and sociocultural influences. The brain processes sexual information in a way that reflects goal-directed behavior, known as the “sexual pleasure cycle.” Dopaminergic neurons and the reward system play a crucial role in sexual drive and pleasure experience, while limbic forebrain structures are involved in motivational states and emotional processing. 31 Additionally, the cerebral cortex is responsible for conscious awareness during all stages of the human sexual cycle, and sensorimotor cortices are involved in triggering voluntary movements during sexual intercourse. The spinal cord plays a role in physical responses such as penile and clitoral tumescence, vaginal and penile gland lubrication, and rhythmic contraction of perineum muscles. The parasympathetic system is involved in erection and female lubrication, while the sympathetic system is involved in ejaculation and orgasm. Female lubrication occurs due to the interaction between vasoactive intestinal peptide (VIP) and neuropeptide Y, which induces venous vasoconstriction and increases interstitial fluid, resulting in vaginal lubrication. 32 The brain plays a crucial role in sexual motivation, with the reward system triggering motivation and the thalamus relaying erotic stimuli. The hypothalamus coordinates autonomic events in sexual behavior, while the Amygdala gives emotional significance to incoming erotic stimuli. The septal region and prefrontal cortex also play roles in sexual drive, with the insula affecting erectile organ tumescence. 31
Female orgasm difficulty may result from various factors responsible solely or in compound manner. Ethnic religious beliefs can influence the perception of sex as a conjugal duty solely related to reproduction, leading to rejection towards partners who do not align with their desires. Physical and Behavioral factors can also affect lubrication and sensitivity in the genitals, which can be influenced by pelvic nerve and blood vessel lesions, pelvic trauma, or surgical interventions. 33
Two commonly observed phenomena in Female Orgasmic Dysfunction (FOD) are hyper-arousal and hyper-intention. Following repeated unsatisfying or negative sexual experiences, women may develop anticipatory anxiety—hyper-arousal—characterized by a preoccupation with performance and outcome. This anxious state interferes with natural responsiveness to sexual stimuli. As frustration mounts, hyper-intention emerges: the woman may exert greater conscious effort to achieve orgasm, paradoxically worsening the outcome. This feedback loop of anxiety and forced effort ultimately diminishes arousal and pleasure. 1
Other physiological causes responsible for FOD include breastfeeding, menopause, oral contraceptives, and antihistamine drugs. Stress and anxiety can also influence the orgasmic potential of women. Anxiety can cause distractions during lovemaking, making it difficult for women to reach an orgasm. Additionally, a lack of harmonious communication, a lack of arousal, or mutual respect can also contribute to the orgasmic reaction. Certain medications like antidepressants, antihypertensive and hormonal medicines may have adverse sexual side effects. Overall, understanding these factors can help improve the quality of sexual relationships and overall well-being. 28
Assessment of Female Orgasm Dysfunction
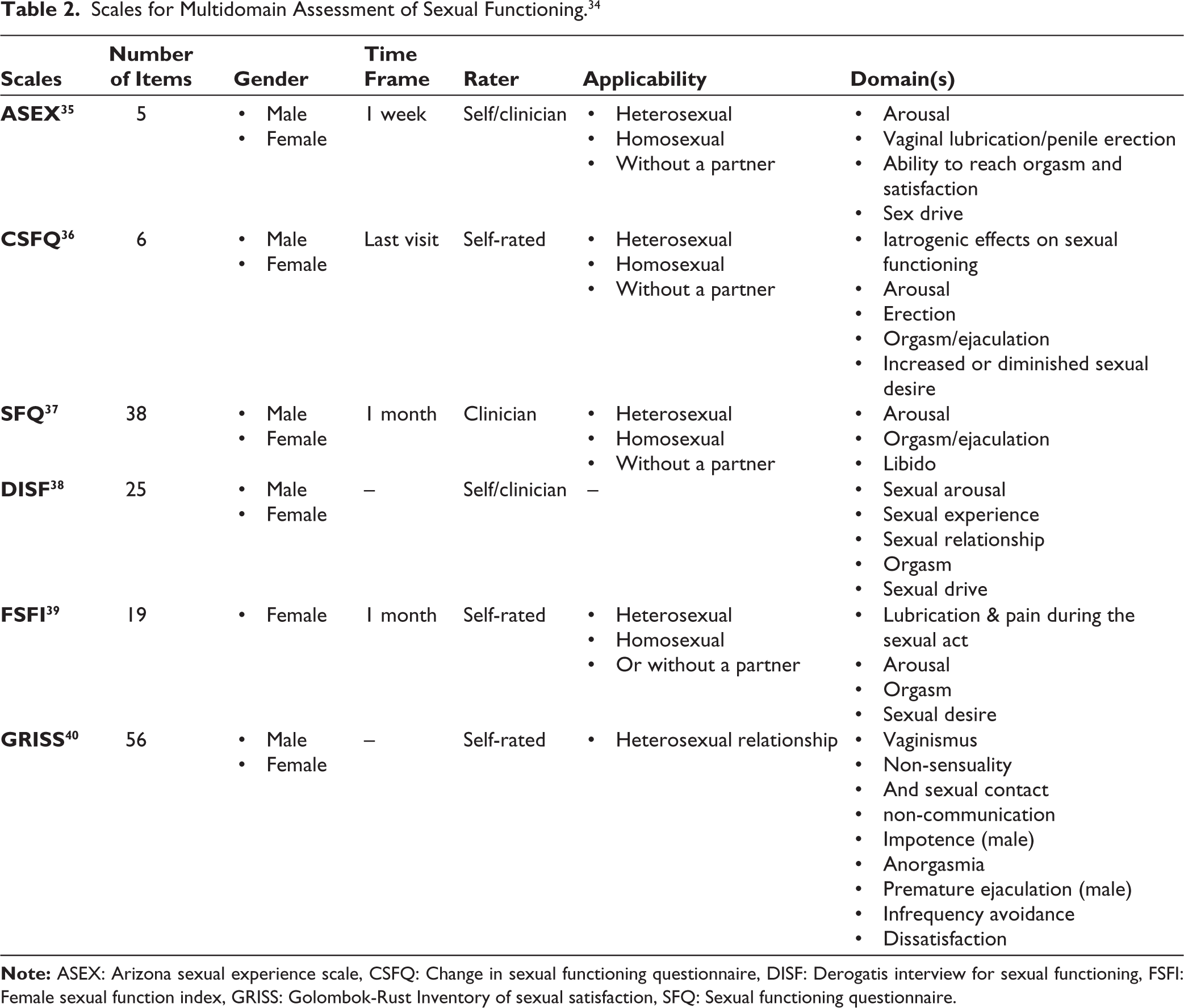
The female presenting with an orgasm problem requires a thorough evaluation. The clinician should clarify the subjects’ presenting complaints and differentiate them from other female sexual difficulties. Onset (lifelong vs. acquired), duration, distress levels, and reasons for seeking consultation require evaluation. Partner-related factors (sexual dysfunctions in partner, attitude, and knowledge, etc.), relationship factors (mutual understanding, intimacy, communication, etc.), individual vulnerability, psychiatric comorbidity, or stressors (guilt, sexual inexperience, history of sexual abuse, body image, etc.), cultural/religious factors (cultural inhibitions, taboos, myths, and cultural norms), and relevant medical factors and medications should be assessed. Clinicians are encouraged to obtain a detailed narrative of a typical sexual encounter, including partnered and solo sexual experiences, to better understand arousal patterns, emotional responses, and orgasmic capacity in different scenarios (Table 2).
Scales for Multidomain Assessment of Sexual Functioning. 34
Management
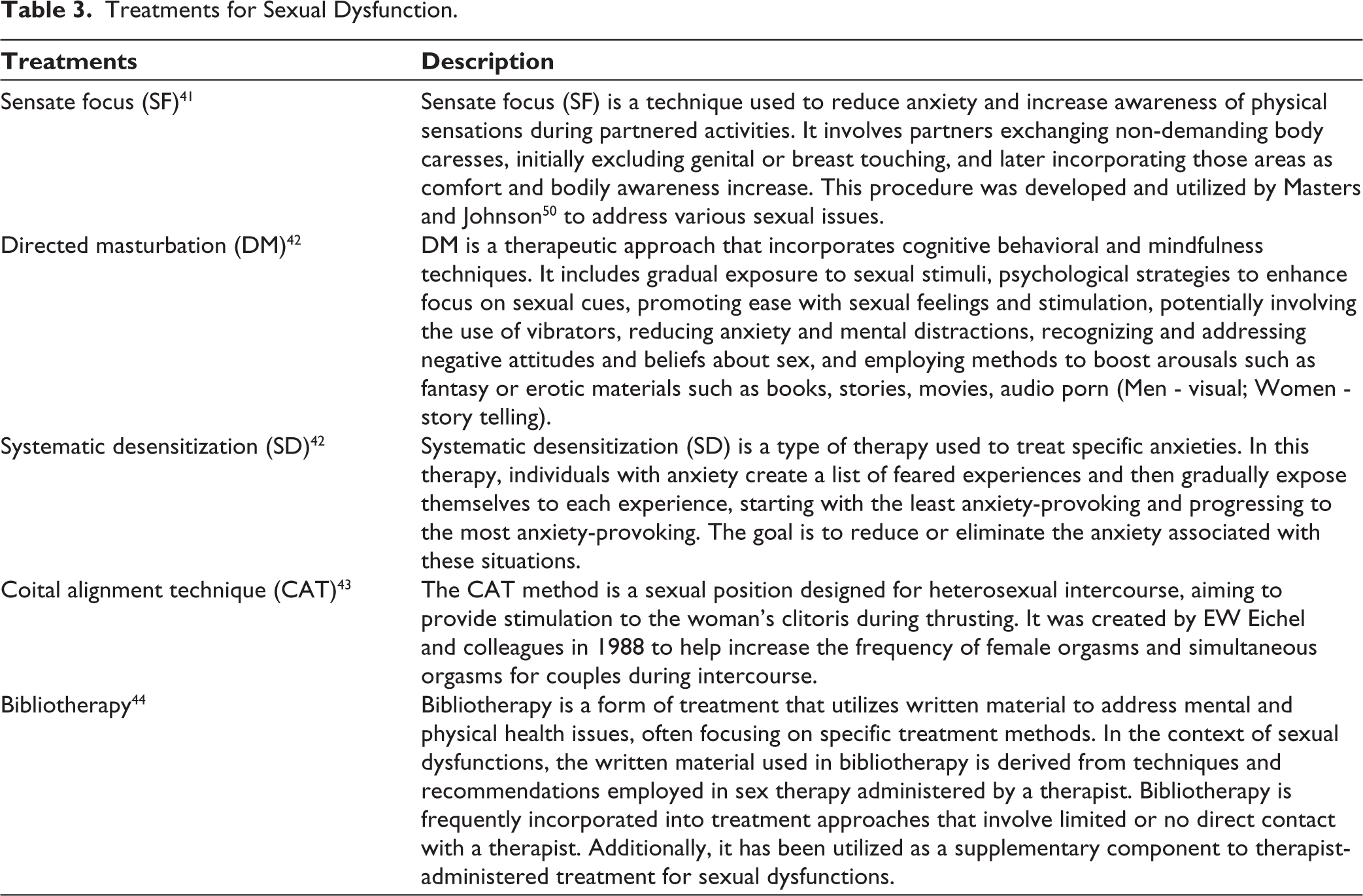
Management of orgasmic concern is related to the type of problems and relevant causative factors as per the assessment. Although a range of interventions has been explored, the treatment of FOD remains limited in scope and, at times, controversial. Non-pharmacological treatment methods include directed masturbation, cognitive-behavioral therapy, systematic desensitization, sex therapy, couple communication training, coital alignment technique (CAT), sensate focus, educational intervention, sexual health model, bibliotherapy, Kegel exercise, hypnotic technique, anxiety reduction techniques, trauma therapy, modelling, orgasm consistency training (OCT), Sex “Aids,” basic counselling, psychotherapeutic interventions for the individual woman and role playing, etc. Non-pharmacological strategies are less likely to cause side effects, and they focus on restoring sexual functioning and enhancing sexual satisfaction beyond symptom reduction. As per available evidence, when conducted in a couple setting, psychological interventions are more effective in reducing the severity of symptoms and improving sexual satisfaction, with a significant effect size. Sex therapy, in addition to sexual skills training, has been the most frequently investigated intervention for female sexual dysfunction, including FOD, over the years. Pharmacological interventions include the use of tibolone, testosterone, sildenafil, bupropion, and estrogens, although evidence for their efficacy remains mixed. However, this article does not aim to provide a detailed review of pharmacological treatments for orgasmic dysfunction (Table 3).
Treatments for Sexual Dysfunction.
Recent Trend
In the current technology-driven world, although getting assistance regarding sexual problems has become more feasible, it may be misleading at the same time. Despite this progress, open and unapologetic conversations about female sexual pleasure remain limited, especially when compared to discourse around male sexual satisfaction. The clitoris is still not given adequate attention, and numerous people still believe that vaginal orgasms are “normal and usual” orgasms that women experience, despite the evidence that a comparatively small number of women experience orgasms during heterosexual vaginal sex. Campaigns like #myclitcount 45 attempted to initiate the movement to reduce social taboos about sexual pleasure along with sexual and reproductive health. Cultural conversations and attitudes towards female sexuality are changing fast. When counselling couples, clinicians are suggested to give particular attention to the female’s orgasm experiences, 46 to potentially help both partners achieve higher sexual satisfaction.
Influential resources and prescriptive books like Becoming Orgasmic (Heiman and Lopiccolo, 1987), 47 Becoming Cliterate (Mintz, 2017), 48 Come as you are (Emily Nagoski) assist individual to explore their sexual functioning, provide information to enhance sensuality and pleasure while engaging in sexual activities, practice safe sex and help learn how to bring orgasm by pulling together evidence from different background (biology, sociology, linguistics, and sex therapy) into comprehensive, accessible, and prescriptive form of literature. Sex positive podcasts are the emerging industry at the intersection of sexuality, technology, and what it means to be human, in the middle of it all, focusing on sex, technology and wellness.
Websites like OMGyes.com 49 which is an educational website, can be a useful adjunct for females willing to understand the nuances and aspects of orgasm. It has about 20,000 interviews with women (18–95 in age) talking about their sexual pleasure. This educational resource has been developed in collaboration with Indiana University and The Kinsey Institute researchers. Techniques such as tapping, edging, rhythm, and layering are thoroughly illustrated using interactive visuals, data, testimonials, and instructional videos, offering a unique blend of personal narrative and empirical evidence. Other digital platforms catering to women’s erotic experiences include Dipsea that provides audio erotica for females, and Literotica 50 that provides stimulation through words instead of imagery. A site recognized by the mainstream adult industry, Sssh.com, is an independent female erotica site and the first “porn for women” website. Others are Lady Cheeky and X Confessions, created by feminist adult filmmaker Erika Lust. The authors do not endorse the clinical use of these resources but present them here for informational purposes only.
Apps such as Flo 51 offer holistic support for women’s reproductive health, including menstrual tracking, fertility prediction, pregnancy guidance, and menopause management. Future of sex explores sexual intimacy and enhancement through connected sex toys, interactive sex shows, participatory porn, and teledildonic virtual sex worlds. While these are not yet part of standard clinical interventions, clinician awareness of such tools may enhance patient engagement and referral to accurate sources. Although, utility of faster evolving technological tools for clinical purposes is still in the nascent stage, a case-to-case based assessment and recommendations by clinicians can be useful. Some clinicians may be hesitant to incorporate entertainment-based materials into care, but as many patients already seek help online, redirecting them to scientifically accurate, user-friendly platforms can be both practical and empowering. Such modern technology-aligned trends made easy to access are helpful to provide females with sexual knowledge and promote pleasure literacy.
Discussion
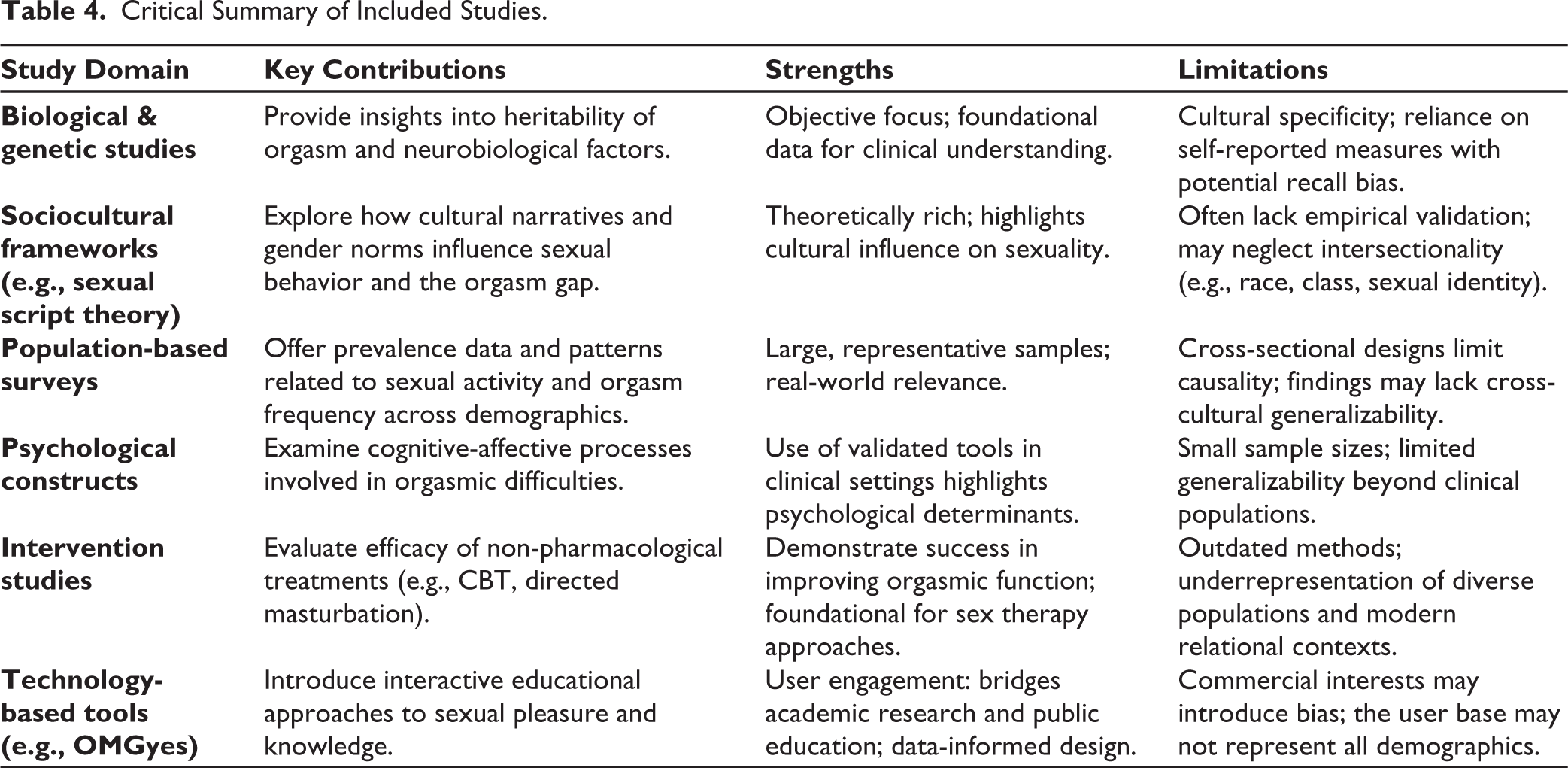
The current body of literature on sexual functioning and the orgasm gap reveals diverse and multifaceted insights (see Table 4). A review of available research highlights both substantive contributions and notable methodological limitations across domains. Biological and genetic studies 7 reviewed here provide invaluable data on the heritability of orgasm but are hindered by cultural specificity and potential recall bias in self-reported measures. Studies exploring sociocultural frameworks like Sexual Script Theory contribute meaningful insights into how cultural narratives shape sexual behaviors, though they often lack empirical support and may overlook the complexities of intersectionality. 19 Population-based surveys 14 benefit from large, representative samples, yet their cultural limitations and cross-sectional designs restrict contributory inferences, hence compromising the reliability of the findings. Furthermore, studies focusing on psychological constructs 12 emphasize the relevance of validated measures in clinical contexts, but their limited sample sizes pose challenges for generalization. Intervention studies have made significant strides in establishing non-pharmacological treatments for orgasmic disorders,30,42 yet they often rely on obsolete methodologies and fail to reflect the diversity of contemporary populations. Lastly, technology-driven initiatives, like by OMGyes in partnership with the Kinsey Institute, present engaging educational tools, although issues related to commercial interests and user demographics may limit their broader applicability. Collectively, this review highlights the necessity of addressing biases, gaps and expanding the inclusivity of research to better inform and understand female sexual health. The study of female orgasm and the orgasm gap involves critical ethical issues related to personal and cultural experiences, particularly concerning participant confidentiality in sensitive sexual health research, and the studies included in the review underscore a commitment to ethical practices in this field.
Critical Summary of Included Studies.
Economic Considerations in Sexual Health
Economic factors significantly influence the understanding and treatment of female orgasmic dysfunction and sexual functioning, yet they often receive insufficient attention in clinical discussions. Socioeconomic status influences access to resources for sexual health, which also includes therapy, educational content, and medical consultations. Many interventions, such as sex therapy or couple-based approaches, may not be available in low-resource environments or may not be covered by health insurance, further limiting access for marginalized populations. The disparity in accessing digital resources, like OMGYes 48 and Dipsea, that are subscription-based educational platform, can further establish the information gap due to the inability to access by many women from lower-income backgrounds. Addressing these disparities is critical, as sexual satisfaction is vital for overall well-being. Therefore, future public health approaches must prioritize inclusive, affordable, and culturally appropriate sexual health education and services, bridging the gap created by economic inequities.
Conclusion
In conclusion, the existing disparity in orgasm frequency between genders in heterosexual relationships constitutes a multifaceted challenge influenced by a range of factors spanning from biology, psychology, sociology, and interpersonal dynamics. Effectively addressing this issue necessitates a nuanced understanding of the mechanisms underlying sexual behavior and responses in both men and women. Moving forward, healthcare professionals should heighten their familiarity with available strategies for perfecting the orgasm gap and offering meaningful support to individuals impacted by this issue. Furthermore, forthcoming research endeavors should prioritize the development of targeted interventions aimed at reducing the orgasm gap and augmenting sexual satisfaction and overall well-being for individuals in heterosexual relationships. By diligently probing and comprehending the multitude of factors impacting sexual functionality and satisfaction, we can aspire to cultivate a more equitable and gratifying sexual experience for all individuals. Acknowledging the significance of this issue and sustaining efforts to narrow the orgasm gap through research, education, and clinical interventions are pivotal steps in fostering positive change.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not required for this study in accordance with institutional requirements.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was not required as no identifiable personal data or human/animal subjects were involved.