
Abstract
Abstract
Background: Depression causes emotional and physical disturbances which impacts biological functions such as sleep, appetite, libido, and disinterest in sexual function. Since discussing sexual problems is considered a taboo, there is limited data available concerning the prevalence of sexual dysfunction in women with depression and its response to treatment.
Aim: To assess the prevalence of sexual dysfunction in females with depressive disorder and the effects of treatment.
Material and Methods: A total of 53 females with recurrent depression and age and sex matched normal control group were included in the study with their informed consent. All the subjects were assessed with the Hamilton Rating Scale for Depression (HAM-D), Arizona sexual experience scale (ASEX), and female sexual functioning index (FSFI), which were re-administered after 6 weeks of treatment.
Results: There was a significant difference in the HAM-D, ASEX, and FSFI scores between index and control groups at baseline. There was a significant correlation between the scores of HAM-D, ASEX, and FSFI before treatment. The correlation between the HAM-D and ASEX scores after treatment was not significant. A significant correlation was found between the HAM-D scores and the scores of arousal, lubrication, orgasm, satisfaction, pain, total domains of FSFI after treatment. No correlation was found between the HAM-D scores and desire domain score of FSFI after treatment.
Conclusion: Women with depression have a high prevalence of sexual dysfunction. A highly significant improvement in depression and sexual functioning was observed at the end of 6 weeks of antidepressant therapy. Despite the improvement in sexual dysfunctions, the individual domains of sexual functions were not comparable to the normal subjects at the end of 6 weeks suggesting the need for longer treatment.
Keywords
Introduction
Human sexual functioning can be described as the characteristic of the way individuals feel and convey themselves. It encompasses biological, erogenous, emotional, social, or spiritual feelings and behaviors of humans. Good sexual functioning is an essential constituent of life and is important for sustaining a gratifying relationship among two people sharing intimacy. Thus, sexual health can be considered a crucial part of physical and mental well-being. The incidence of sexual problems in females is reported to be 43% and 31% in males. 1 Sexual dysfunction in females can be categorized into the following types: hypoactive sexual desire disorder, female sexual arousal disorder, female orgasm disorder, and pain disorders. 1 Amongst them, the most commonly seen are the hypoactive sexual desire disorder and sexual arousal disorder. 2 It can be argued that the attitude to sexual dysfunctions accepted by the International Classification of Diseases, Tenth Revision (ICD-10) and Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) may not do justice to the diverse and often exceptional means in which male or female patients present with sexual complaints. Other aspects of sexual response are also affected when one part of the sexual cycle is affected. The prognosticators of sexual problems that people suffer from may fluctuate with time, according to “cultural shifts, generational, and societal norms.” 3 Hence, it is important to broaden our minds and look beyond the presenting symptoms and find the diagnosis which fits the patient best.
Depression was found to be the fourth most common cause of disease burden, responsible for 4.4% of total disability-adjusted life years (DALYs) in the year 2000, and it produces the greatest amount of non-fatal burden, responsible for almost 12% of all total years lived with disability worldwide. It is said that depression will be responsible for the largest burden of disease illness by 2020. Depression leads to emotional and physical problems which impact biological functions such as sleep, appetite, diminished libido, and disinterest in sexual function. Zurich cohorts study by Angst et al shows that the prevalence of sexual problems in patients with depression is approximately twice that of the controls. 4 Some of the antidepressants prescribed for the depression may cause problems in sexual functioning and may affect all the stages of the human sexual cycle. 5 Antidepressant-induced sexual problems become a significant concern in the situation of management effectiveness, as antidepressants are useful only as long as the patient takes them regularly. Unbearable adverse effects can be one reason that patients do not take medicines or stop them abruptly. Nonetheless, maximum of the findings from research done on drug-induced sexual dysfunctions have combined numbers for both males and females, except a few.6, 7
The understanding of female sexuality is not at par with that of male sexuality. 8 In the last few decades, research in the field of sexuality has gained momentum all over the world. However, various lacunae remain in our knowledge about sexual dysfunction in spite of advances in treatment of sexual problems. In particular, our information about female sexual dysfunction has constantly lagged behind that of male sexual problems. Studies on the topic of sex are scant in India and whatever research has been done has mostly focused on sexual dysfunction in males. In fact, comparatively, not much is established about sexual behaviors, sexual attitudes, sexual fantasies, and marital functioning of Indian women. Also, there is not much research from India that has assessed the presence of sexual problems in patients who are taking psychotropic medications. While there is a handful of statistics to imply that women have progressive outlook towards sexuality, in countries like ours conversing about sexual problems is largely considered a taboo. Female sexual dysfunction was identified as a significant yet largely un-investigated public health problem. There is very little population-based data available concerning the predictors, prevalence, and consequences of this disorder. Looking from the Indian perspective, the females in India do not talk freely about sexual problems that they face. Cultural and societal views might be responsible for very few women coming forward with problems regarding sexuality. Hence, one finds that various researches have focused on male sexual dysfunction but the same cannot be said for female sexual dysfunction. The studies on sexual dysfunction in women being few, a necessity was felt to explore the attributes of female sexual dysfunctions and its relation to underlying depression and response to treatment. A detailed and comprehensive look into this condition will lead to effective treatment and better enhancement of quality of life. In view of the paucity of Indian studies, the present work was undertaken to study the prevalence of sexual dysfunction in females with recurrent depressive disorder.
Material and Methods
This prospective longitudinal study was carried out at a tertiary care hospital and research center attached to a medical college from July 2017 to September 2018. Institutional ethics committee permission was acquired before starting the study. The study sample consisted of consecutive females attending the outpatient department with diagnosis of recurrent depressive disorder (F 33) as per ICD-10 DCR 9 and meeting the inclusion and exclusion criteria. Equal number of age matched female subjects without any past or family history of psychiatric disorder formed the control or index group. A total of 53 females from both the groups were evaluated. The following inclusion and exclusion criteria were fulfilled before the subjects were taken up for the study.
Females diagnosed to have recurrent depressive disorder according to ICD DCR 18 to 45 years of age who were sexually active Not on any psychotropic medication or drug-free for 6 weeks Willing to give consent for the study
Who were not sexually active Patients requiring electroconvulsive therapy Those having any comorbid medical illness
18 to 45 years of age who were sexually active Willing to give consent for the study
Who were not sexually active Those having any other comorbid medical illness Those with past or family history of psychiatric disorder
Methodology
All the patients and people in the control group included in the study were explained about the nature of the study and informed consent was taken. All patients were interviewed in the presence of a female investigator. After that the sociodemographic data was filled up. Thereafter, all the patients and control subjects were administered HAM-D, ASEX, and FSFI. All the patients with depressive disorder were started on conventional lines of treatment. All the patients were re-administered the HAM-D, ASEX, and FSFI at the end of 6 weeks of treatment to assess their depression and sexual functioning. The scales were scored as per the test manual and data entered in an Excel sheet.
Statistical Analysis
The SPSS software package for Windows, version 20.0, was used for statistical analysis. Descriptive statistics: Data summarization was carried out with the help of percentages and summary statistics will be with mean, range, and standard deviation.
Inferential statistics: The frequency data was compared using the chi-square test/Fisher’s exact test, and ordinal data using the Mann-Whitney and Wilcoxon test at 5% significance.
Results
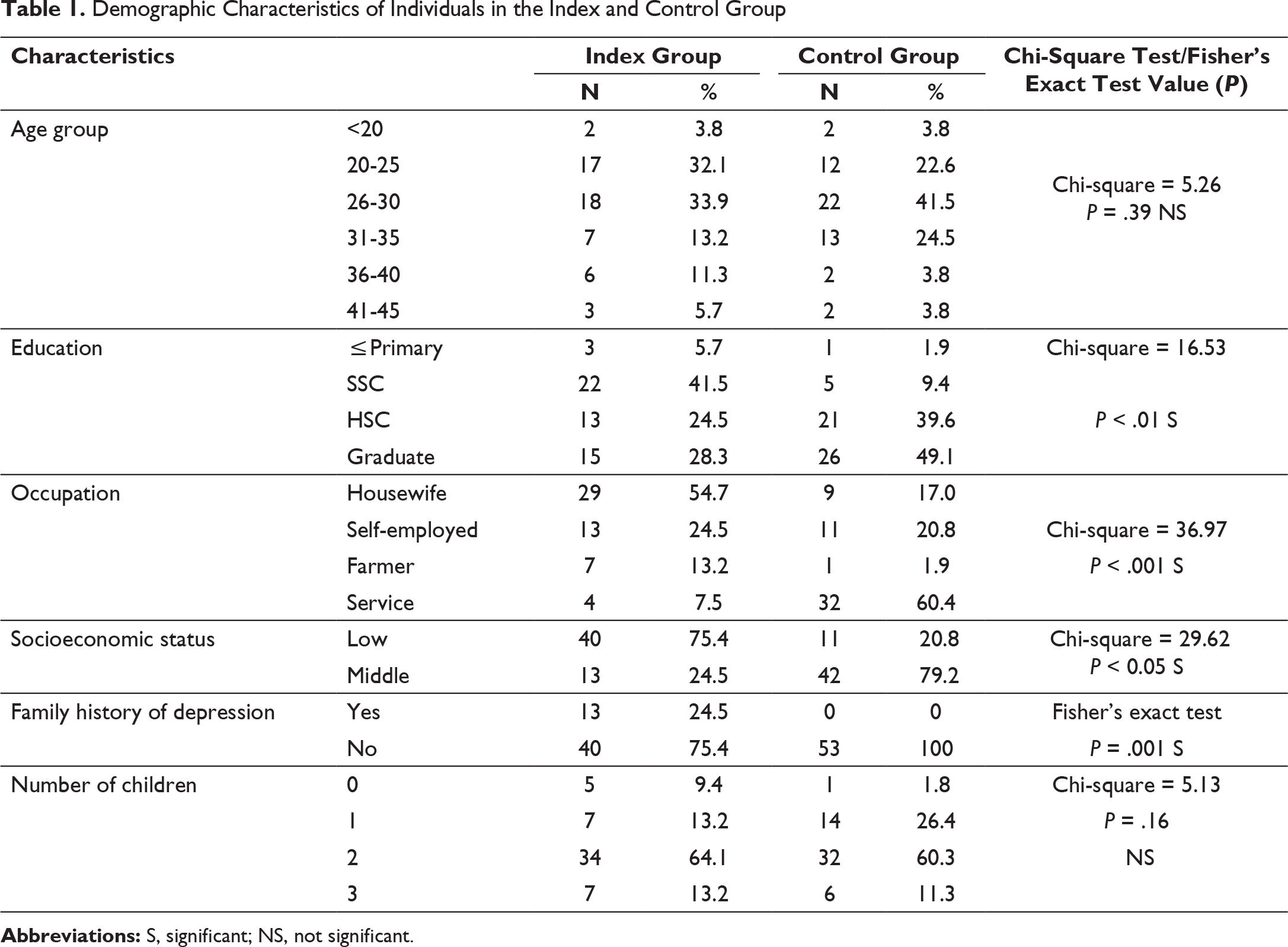
The present study included 53 females with recurrent depressive disorder and an equal number of age matched females were included in the control group. The mean (±SD) age of the sample in index group was 29 years and in control group was 28 years. The age range in the index group was 18 to 45 years and in control group was 18 to 44 years. The commonest age group was 26 to 30 years in the index and control groups. There was no significant difference in the age distribution (Table 1).
Demographic Characteristics of Individuals in the Index and Control Group
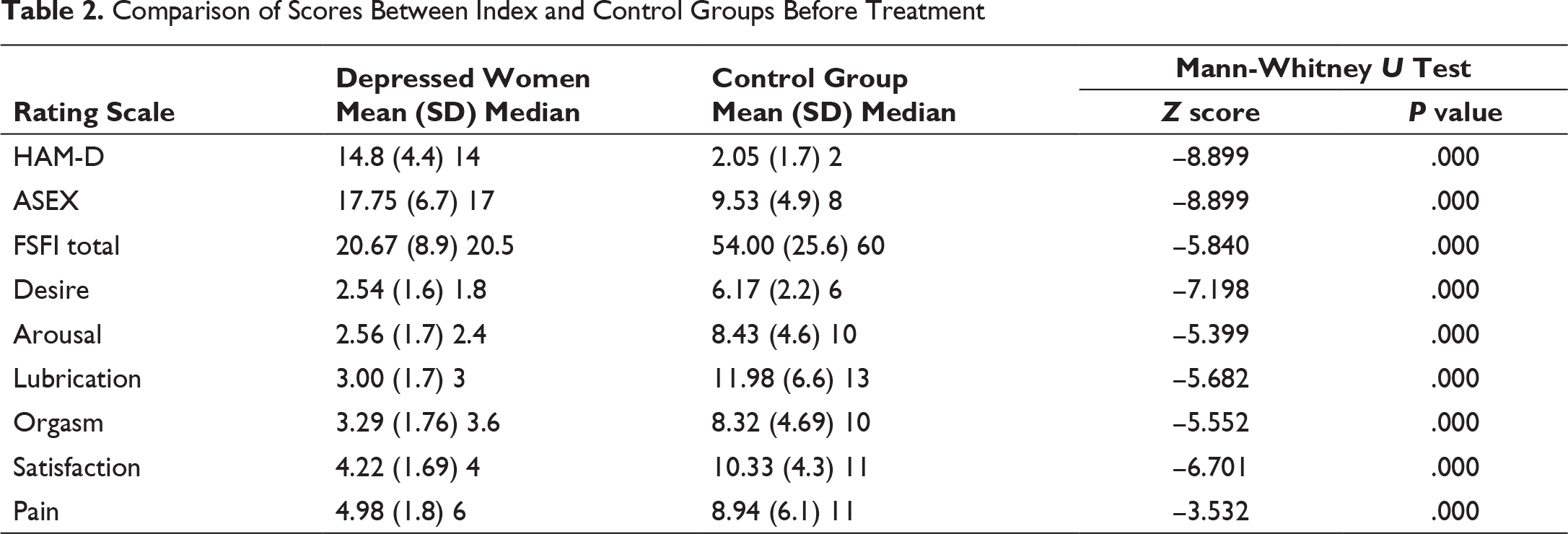
Comparison of Scores Between Index and Control Groups Before Treatment
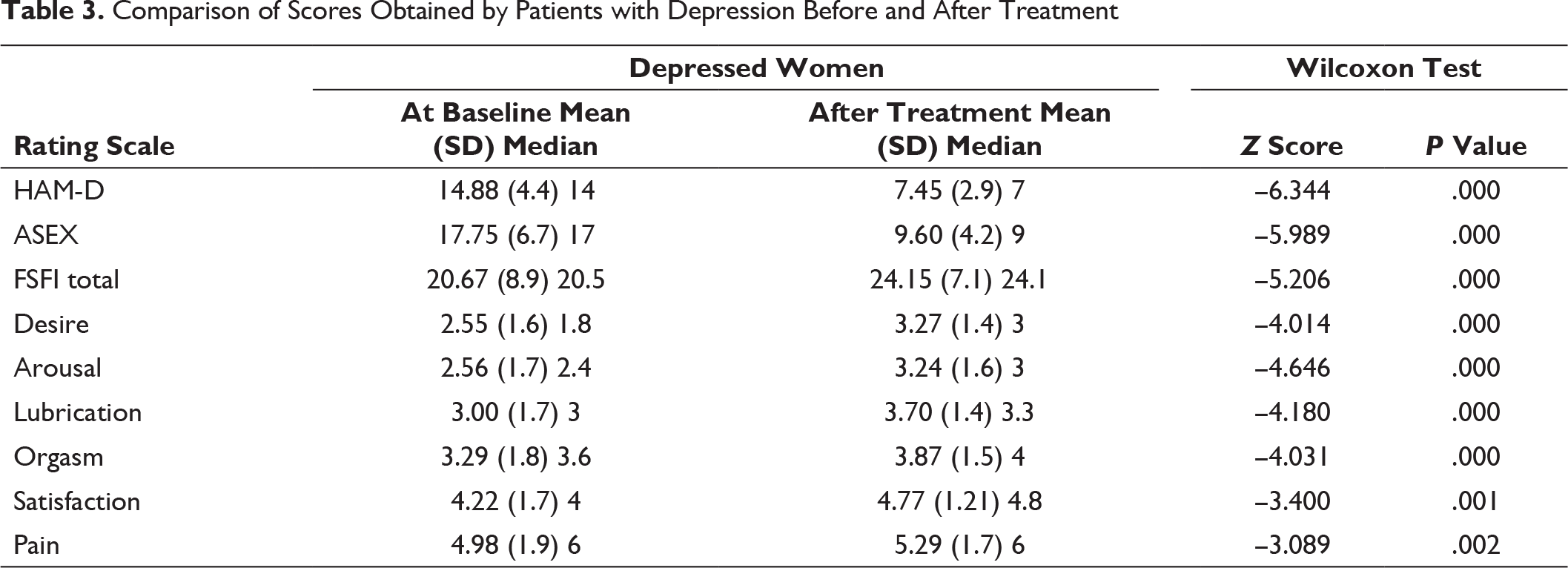
Comparison of Scores Obtained by Patients with Depression Before and After Treatment
Comparison of Scores Between Index and Control Groups After Treatment
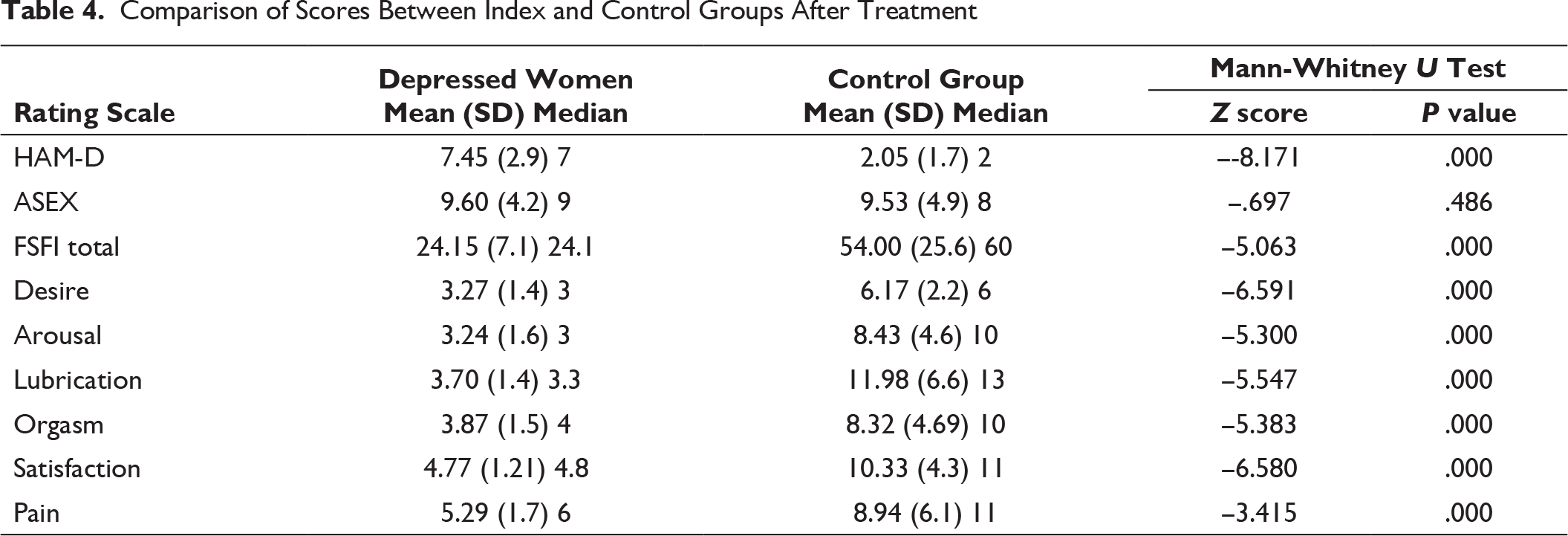
Table Showing the Spearman’s Correlations Between the Scores of HAM-D with ASEX and FSFI (Desire, Arousal, Lubrication, Orgasm, Satisfaction, Pain, Total) in the Index Group Before Treatment
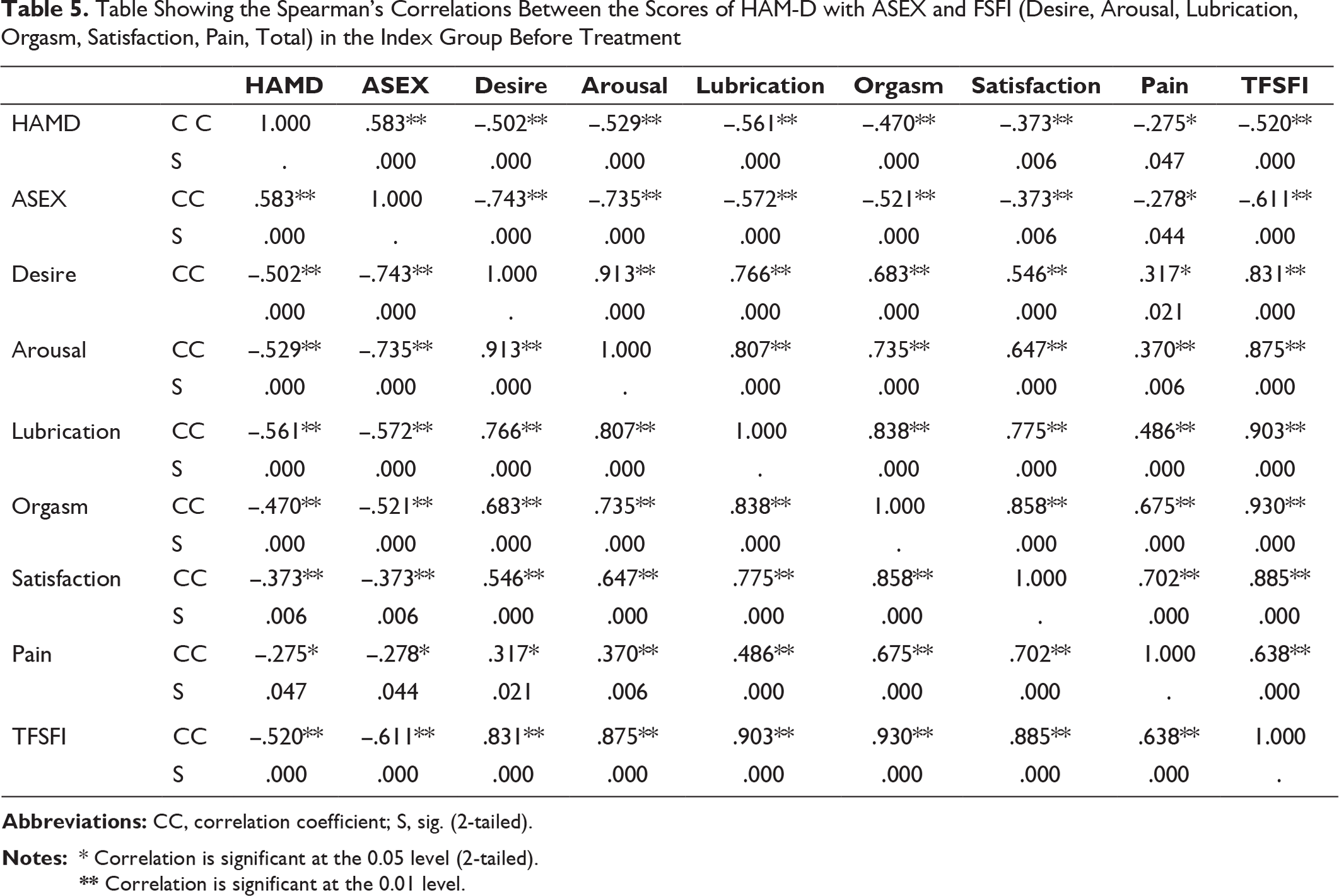
** Correlation is significant at the 0.01 level.
Table Showing the Correlations Between the Scores of HAM-D with ASEX and FSFI in the Index Group After Treatment
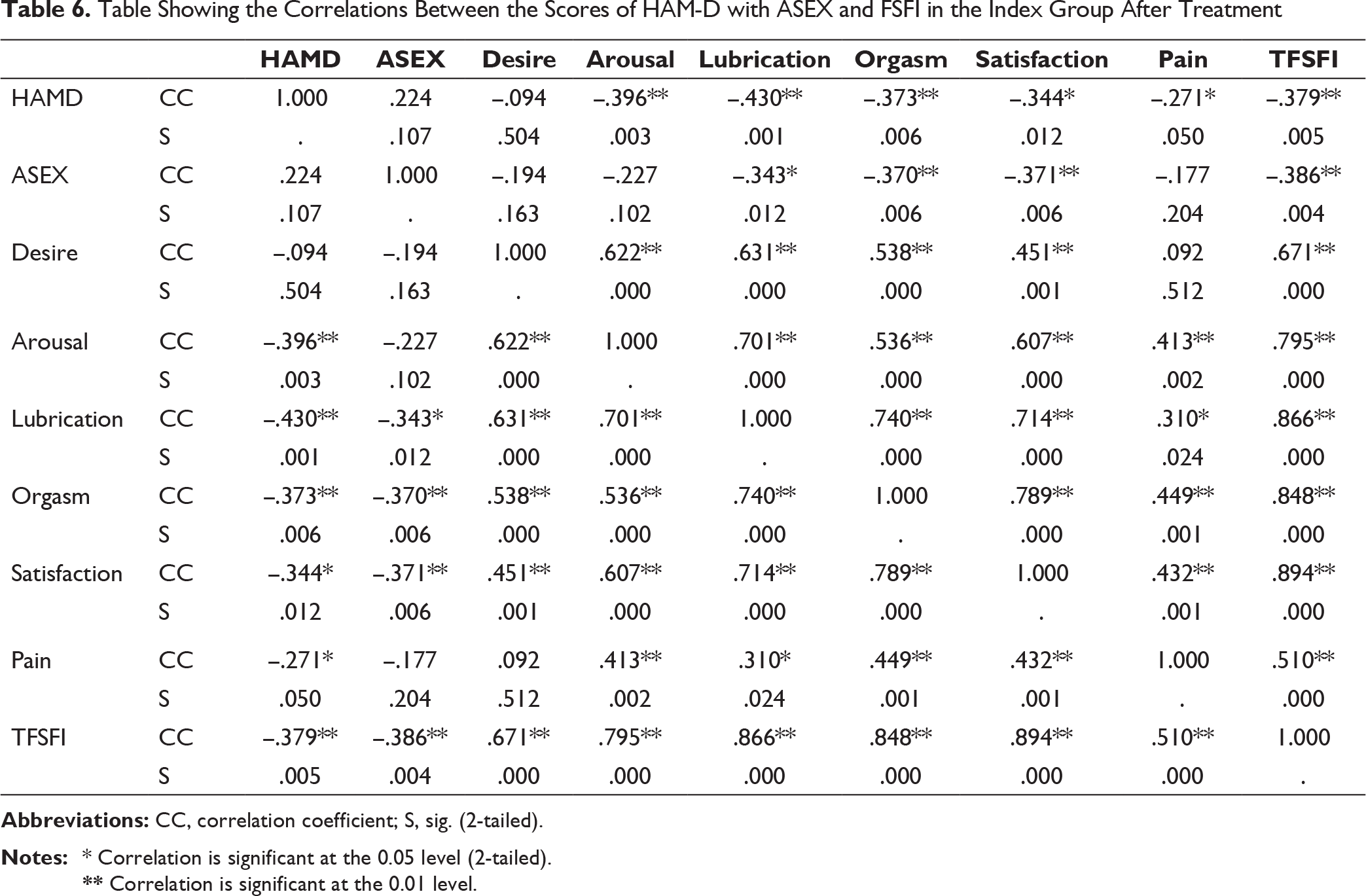
** Correlation is significant at the 0.01 level.
There was a significant difference between the HAM-D, ASES, and FSFI scores in depressed patients before and after treatment (Table 3).
There was a significant difference in the HAM-D score between the index and control groups after treatment. There was no significant difference in the ASEX score between the index and control groups after treatment. Thus, the scores are comparable between the index and control groups showing that the patients have improved to near normality. However, there was a significant difference in the FSFI scores between the index and control groups after treatment (Table 4).
There was a significant positive correlation between the scores of HAM-D and ASEX scores in the index group before treatment. There was a significant negative correlation between the scores of HAM-D and all the domains of FSFI (desire, arousal, lubrication, orgasm, satisfaction, pain, total) at baseline in the patients suffering from depression (Table 5).
There was a positive correlation between the HAM-D and ASEX scores after treatment, but it was not significant. There was a significant negative correlation between the scores of HAM-D and arousal, lubrication, orgasm, satisfaction, pain, total domains of FSFI after treatment in the patients suffering from depression. No significant correlation was found between the scores of HAM-D and desire score of FSFI in the index group after treatment (Table 6).
Discussion
The study was carried out at a tertiary care hospital situated in an urban area and the patients had cooperated in the study to the best of their ability. The primary aim of the study was to assess the occurrence of sexual problems in women with recurrent depressive disorder and also to find out the types of sexual dysfunction in them. Later the changes in sexual functioning after treatment with conventional antidepressants were measured and the association between the control group and the index group was analyzed.
Sociodemographic Profile
Comparison of HAM-D, ASEX, and FSFI Scores Between Index and Control Groups Before Treatment
It was found that there was a significant difference in the HAM-D scores when it was compared between index and control groups before starting treatment. This shows that depression was highly prevalent in the index group. When ASEX and FSFI scores were compared between index and control groups before treatment, a significant difference was found. This shows that the patients taken for the study group had clinically significant problems in areas of sexual functioning and depression prior to starting treatment and were very different from their peers in the control group who did not suffer from depression. Previous reports also corroborate our findings wherein they show higher levels of sexual dysfunction in depressed patients as compared to non-depressed patients. 35 Sexual problems and dissatisfaction with sex were commonly associated with depression. There was a significant difference in all the domains of the FSFI scores when a comparison was done between index and control groups before treatment. When all the patients were studied for the domains of sexual functioning, it was found that sexual dysfunction is very prevalent in the index group affecting nearly all areas of sexual functioning.
Comparison of HAM-D, ASEX, and FSFI Scores Before and After Treatment
There was a significant difference in the HAM-D scores before and after treatment in this study. This shows an improvement in their depressive features as is evidenced by the improvement in the scores. This was corroborated by numerous studies which also exhibited an improvement in symptoms of depression after treating with antidepressants.36-38 It was found that a there was a significant difference between the ASEX and FSFI scores before and after treatment in this study. The areas of improvement included a correction in the sex drive, and physiologic and psychological arousal. Hence, we can infer that sexual problems reduced and there was an improvement in the sexual functioning after the patients were treated with antidepressants.
Comparison of HAM-D, ASEX, and FSFI Scores Between Index and Control Groups After Treatment
When a comparison was done in the HAM-D scores between index and control groups after 6 weeks of treatment with antidepressants, a statistically significant difference was found. Hence, we can infer that though improvement in depression was observed on follow-up but the patients were not comparable to normal subjects. This suggests that there is further scope for improvement and longer treatment might lead to even more improvement. There was no significant difference in the ASEX scores between index and control groups after 6 weeks of treatment. Hence, the sexual functioning improved so much so that it was comparable to those of the control group. It was observed that there was a significant difference in the FSFI scores between index and control groups after 6 weeks of treatment with antidepressants. This indicates that even though the patients showed improvement in their sexual functioning after treatment, the individual domains of sexual functions were not comparable to their peers who were not suffering from any depression or mental illness when FSFI was used. This could be because ASEX assesses sexual dysfunction and FSFI assesses the individual dimensions of sexual functions. Hence, it shows that there is scope for further improvement in their depressive features and that their sexual problems may take more time to decrease if treatment is given for longer periods of time. This emphasizes the need for treating depression for optimal periods of time along with monitoring of the sexual dysfunctions.
Correlations Between the Scores of HAM-D, ASEX, FSFI (Desire, Arousal, Lubrication, Orgasm, Satisfaction, Pain, Total) in the Index Group Before Treatment
There was a noteworthy positive correlation between the scores of HAM-D and ASEX scores in the index group before treatment. There was a considerable negative correlation between the scores of HAM-D and all the domains of FSFI comprising of domains of desire, arousal, lubrication, orgasm, satisfaction, and pain and also the total score at baseline in the patients suffering from depression. It has been found in other studies also that depression often leads to difficulty in sexual arousal, amongst other sexual dysfunctions. 39 Hence, this throws light on the fact that we should be extremely vigilant with females presenting to our clinics with depression and should regularly ask them for sexual problems as they may not tell it themselves even if the problem is present. Indian women being reticent about sex would not have reported problems in all these areas unless being enquired about the same. Depressive disorders and its consequences on sexual functions hinder the quality of life and hence should be evaluated so that the approach treats all the underlying problems. Assessing the sexual problems and dealing with them effectively will give rise to accurate treatment and an overall better improvement of the patients.
Correlations Between the Scores of HAM-D, ASEX, FSFI (Desire, Arousal, Lubrication, Orgasm, Satisfaction, Pain, Total) in the Index Group After Treatment
There was a positive correlation between the scores of HAM-D and ASEX scores after treatment but it was not significant. There was a significant negative correlation between the scores of HAM-D and domains of FSFI including arousal, lubrication, orgasm, satisfaction, pain and also total FSFI score after treatment in the patients suffering from depression. No significant correlation was found between the scores of HAM-D and desire score of FSFI in the index group after treatment. Thus, we can infer that the overall sexual functions definitely improved after 6 weeks of treatment with conventional antidepressants with a reduction in depression. However, residual effect on sexual functioning still remains in the domains of arousal, lubrication, orgasm, satisfaction, and pain. This shows that as depression improves, sexual functioning also improves which has been corroborated in many earlier studies40-43 which showed that females with depressive disorders have more sexual dysfunctions at baseline and that there is recovery of sexual functions after treatment with conventional antidepressants.
Limitations
This study had certain limitations. The cases of the sample belonged to a tertiary care center and did not reflect the prevalence in the general population. The sample size was modest. A larger sample would throw more light on the extent of problem in general population.
The sample was matched for age but not for other parameters such as education and occupation which could have affected understanding and reporting sexual problems. A sample matched for education and occupation would give more information
Conclusion
Women with depression have a high prevalence of sexual dysfunction. There was a high association between depression and sexual dysfunctions in females with a strong relationship in almost all the areas of sexual functioning (i.e., desire, arousal, lubrication, orgasm, satisfaction, and pain) with lubrication being maximally affected. A highly significant improvement in depression and sexual functioning was seen from the baseline at the end of 6 weeks of antidepressant therapy. Though the improvement was seen in sexual dysfunctions, the individual domains of sexual functions were not comparable to the normal subjects at the end of 6 weeks suggesting a need for a longer treatment.
Clinical Implications
This study helps us to know the high prevalence of sexual dysfunction in depressed females before starting the treatment, emphasizing on inquiring about sexual dysfunction in depressed patients, especially females. It emphasizes the need for awareness about the various aspects of sexuality and the need for education for early detection and treatment of sexual dysfunction in depressed females. Since the patients may not come up with this particular problem on their own, it is extremely important to ask about sexual problems in depressed females and treat them accordingly so that the patients improve maximally.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.