
Abstract
This case report of brief research communication utilized single case design aimed at studying the efficacy of online psychoeducation and cognitive behavior therapy (CBT) on female sexual interest/arousal disorder. Arizona Sexual Experience Scale (ASEX) was used for data collection. Findings of the study showed that client’s pretest and posttest results significantly differ after online psychoeducation and CBT; sexual arousal, sex drive (desire), vaginal lubrication, orgasm, and orgasm satisfaction significantly improved. Furthermore, significant improvement in the frequency of sexual relationship was found. Outcome of this study should guide clinical psychologists in the area of intervention for sexual disorder, especially among women. It should also serve as a reference material for women suffering with sexual dysfunction and serve as an encouragement not to die in silence but seek for professional help.
Keywords
Introduction
Adequate sexual satisfaction is an important area of marriage and it is desirable in every marriage. However, for most couples the bedroom is silent due to sexual dysfunction. Individuals suffering from sexual dysfunction are dying in silent. In most situations, individuals suffering from sexual dysfunctions don’t know where to seek for help, thus they die in silence. Sexual dysfunction can be found in the husband, wife, or both couples, although most individuals suffering from sexual dysfunction are not even aware that they have sexual dysfunction.
The difficulty that occurs during the sexual response cycle which prevents the individual from experiencing sexual satisfaction is referred to as sexual dysfunction. 1 A substantial number of Nigerian women are affected by sexual disorder. 2 Among women in university environment in Enugu State Nigeria, female sexual dysfunction is common with those 41 to 50 years having the highest prevalence. 3 Also, Adebusoye et al 4 reported a high prevalence of female sexual dysfunction among married women in Ibadan. Similarly, result of a Nigerian hospital-based cross-sectional descriptive study among females revealed that among 300 participants, 285 (95%) had sexual disorder, 297 (99%) had lubrication and pain disorders, respectively, 276 (92%) had orgasm disorder, 273 (91%) had desire disorder, 267 (89%) had arousal disorder while 258 (86%) had satisfaction disorder. 2 Sexual dysfunctions peculiar to women according to American Psychiatric Association are female orgasmic disorder, female interest/arousal disorder, and genitopelvic pain/penetration disorder. 5 However, for the purpose of this study, the sexual dysfunction of interest is female sexual interest/arousal disorder. 6 Reports show that female sexual interest/arousal disorder deprives intimacy gotten from natural sexual pleasure among humans. 7 Cognitive behavior therapy (CBT) is used to improve undesirable sexual function.
CBT is the mostly used short-term psychological intervention for sexual dysfunction. 8 Earlier, outcome of a study showed that CBT had significant impact among women with sexual dysfunction. 9 After cognitive behavioural consultation in a randomized clinical trial, significant increase in sexual function and behavioural domains were reported. 10 Result of an experimental study among couples in Iran showed that sexual cognitive reconstruction therapy reduced sexual problems among couples. 11 Also, outcome of a randomized clinical trial among Iranian pregnant women showed that after CBT sexual performance improved. 7 Furthermore, participants in an eSense (online CBT) intervention for sexual challenges showed significant pre- and posttest improvement in sexual arousal, desire, satisfaction, and distress. 12
Psychoeducational cognitive-behavioural counselling has been found effective in a clinical trial study among control and intervention groups in improving female sexual function. 13 Sexual functioning of married Iranian couples improved after group psychoeducational therapy. 14 A feasibility study of brief online psychoeducation intervention 15 reported notable pre-post improvements in sexual arousal, desire, and satisfaction among women with sexual interest/arousal disorder. According to Carter et al, 16 psychoeducation had significant effect on sexual functioning. Furthermore, findings by Brotto et al 17 suggest that brief psychoeducation can improve sexual response significantly in the areas of sexual desire, orgasm, arousal, sexual distress, and satisfaction.
Happiness in marriage can be attributed to many factors, likewise reasons of marital unhappiness vary. However, normal sexual functioning is a vital factor that contributes to marital happiness in most marriages while sexual dysfunction leads to unhappiness in most marriages. Unfortunately, most individuals suffering from sexual dysfunction are not aware of psychological intervention for sexual dysfunction. Sexual dysfunction has led to marital unhappiness, separation, divorce, and/or infidelity among most couples. While others abuse sexual enhancement drugs, sexual dysfunction is prevalent among couples but not addressed psychologically in most cases. Several studies have been carried out elsewhere on the efficacy of online psychoeducation and CBT on treatment of sexual dysfunction with few or no Nigerian study in this area. Thus, the aforementioned constitute the problem identified in this study. Therefore, this study is aimed at studying the efficacy of online psychoeducation and CBT in the treatment of female sexual interest/arousal disorder in Nigeria utilizing a single case design. Thus, it is hypothesized:
Client’s pretest and posttest results would significantly differ after online psychoeducation and CBT. Frequency of sexual relationship will increase after online psychoeducation and CBT.
Method
Design
In this case report of brief research communication, single case design (pre- and posttest) was employed utilizing mixed design approach (quantitative and qualitative methods). A 25-year-old married woman with sexual-related challenge participated in this study.
Participant/Case Report
A 25-year-old married woman who has been married for the past 4 years participated in this study. Client reported that her sexual challenge got worst after giving birth about a year ago. Client reported that she noticed her sexual challenge since her first sexual experience (premarital) about 6 years ago, the problem persisted even when she got married and got worst after child birth through caesarean section. Furthermore, client reported that the thought of sex takes her off before marriage but she hoped that it will get better after she married but the problem persisted. She explained that “Sometimes I desire sex but in the process during foreplay most times the thought of it leading to sex just turns me off before it gets to anything.” She further explains that she never thought of having sex since she gave birth, although “sometimes my husband attempts but I end up not getting wet despite adequate foreplay, the thought of it leading to sex messes with my head I think.” “After giving birth I think the fear of getting pregnant worsen my situation because of the circumstances around the delivery made me scared of getting pregnant, because my delivery was through caesarean section. But before giving birth I really don’t know what happened, I just got tire of sex and I won’t mind having sex once a month if not once in two or three months.”
Client reported that the following could be the possible causative factors of her challenges, “emotional burden, when something hurts me I hardly talk about it, I just bottle it up, I am scared of not being the person people expect me to be, I don’t want to make a person sad so I just take the pain of both sadness to myself, which literary hurts me, I don’t get to express myself, stress, and feeling sad are other possible factors.” Generally, her challenges relating to her sexual experience include the following: “I find it hard to desire having sex or initiate sex, my husband is not happy with the situation, which has significantly affected me, I can begin the sex process (romance/foreplay) but I don’t get wet and I lost interest before penetration, I enjoy sex but I don’t desire having sex, sometimes in the middle of sex I lost interest.” The following goals were set: “I want an improvement in my sexual interest and arousal, I want to be happy, to be able to make love to my husband without any fear or giving many excuses why we shouldn’t, I want to be able to control my emotions so it doesn’t get the best of me or my relationship, and I want the sexual frequency between me and husband to improve.”
Instruments of Data Collection
Diagnostic and Statistical Manual of Mental Disorders Fifth Edition
Diagnostic and Statistical Manual of Mental Disorders (DSM-5), diagnostic criteria for sexual disorder was utilized in determining client’s sexual disorder. Client meets the diagnostic criteria for female sexual interest/arousal disorder. 5
Arizona Sexual Experience Scale
Arizona Sexual Experience Scale (ASEX), a 5-item sexual experience scale was also used for data collection in this single case design. The scale is a self-rated scale design to assess individuals with sexual dysfunction in 5 different domains which include: sex drive, arousal, vaginal lubrication, orgasm, and satisfaction from orgasm. 18 Analysis of receiver-operator characteristic indicated area under the curve value of 0.929 + 0.029, indicating excellent sensitivity and specificity of the scale in identifying sexual dysfunction. Cronbach alpha of the scale showed internal consistency of (α = 0.905), test-retest reliability of r = 0.801 (for patients), and r = 0.892 (for clients). 18
Ethical Consideration
Institutional ethical clearance was not sought for because participant voluntarily participated in the study as a private client due to her sexual-related challenges. However, the aim and nature of the study was explained to her, and she consented. She was assured that the study posed no harm or danger in any way. Furthermore, she was assured confidentiality, that information provided would be used for research purpose only and her identify shall not in any way be revealed.
Procedure
This single case design with emphasis on online psychoeducation and CBT lasted for a period of 17 sessions (from third week of December 2021 to third week of April 2022). Session 1 focused on history taking, session 2 psychological assessments (pretest) ASEX was administered to client and DSM-5 diagnostic criteria for female sexual disorder was considered, session 3 general psychoeducation on female sexual dysfunction, session 4 psychoeducation on client’s psychological assessment and diagnosis (with emphasis on female sexual interest/arousal disorder and identifying possible causative factors), session 5 CBT with emphasis on cognitive restructuring in order to address clients sexual disorder causative factors (negative thoughts regarding sexual relationship) and self-monitoring/evaluation of sexual desire and fantasies. Client was also challenged to discuss with her husband issues that borders her in the marriage that also affect her sexual experience. Sessions 6 and 7 focused on cognitive restructuring with emphasis on training client on creating sexual fantasies and desires, session 8 focused on CBT (cognitive restructuring) and psychoeducation with emphasis on challenging clients negative thought process.
After session 8, client was giving assignment to deliberately initiate sexual relationship with her husband and monitor herself with emphasis on how her body responds sexually in relation to sexual fantasies, desire/arousal on a scale of 0 to 10 with 0 no sexual fantasy, desire/arousal and 10 extreme sexual fantasy, and desire/arousal. Client reported scores of 3, and 6 respectively level of sexual fantasy, and desires/arousal. Despite clients level of fantasies and desire/arousal, she could not initiate sexual experience because she was angry with her husband. Session 9 focused on CBT with emphasis on encouraging client to address issues that made her angry with her husband and initiate sexual relationship afterward. Also, sessions 10 and 11 focused on CBT with emphasis on challenging client to initiate sexual relationship with her husband. Session 12 psychological assessment (posttest) ASEX was readministered to client and DSM-5 diagnostic criteria for female sexual interest/arousal disorder was re-evaluated. Sessions 13 focused on evaluating the entire sessions so far and addressing possible issues that were not addressed, client reported having exciting sexual relationship and the frequency has also improved. Session 14 self-evaluation, progress report, and conclusion and sessions 15, 16, and 17 follow-ups on client’s progress report.
Result
Diagnostic Criteria for Female Sexual Interest/Arousal Disorder
Based on DSM-5 diagnostic criteria for female sexual dysfunction, client meets the diagnostic criteria for female sexual interest/arousal disorder, client reported significant lack of sexual interest/arousal, sexual activity, absence of sexual thoughts, and no initiation of sexual activity and unreceptive of partner’s initiation, the sexual difficulty is experienced in approximately 75% to 100% of sexual activity. The sexual disturbance is life-long with moderate evidence of distress in criterion “A” symptoms.
Hypothesis 1
Client’s pretest and posttest results would significantly differ after online psychoeducation and CBT.
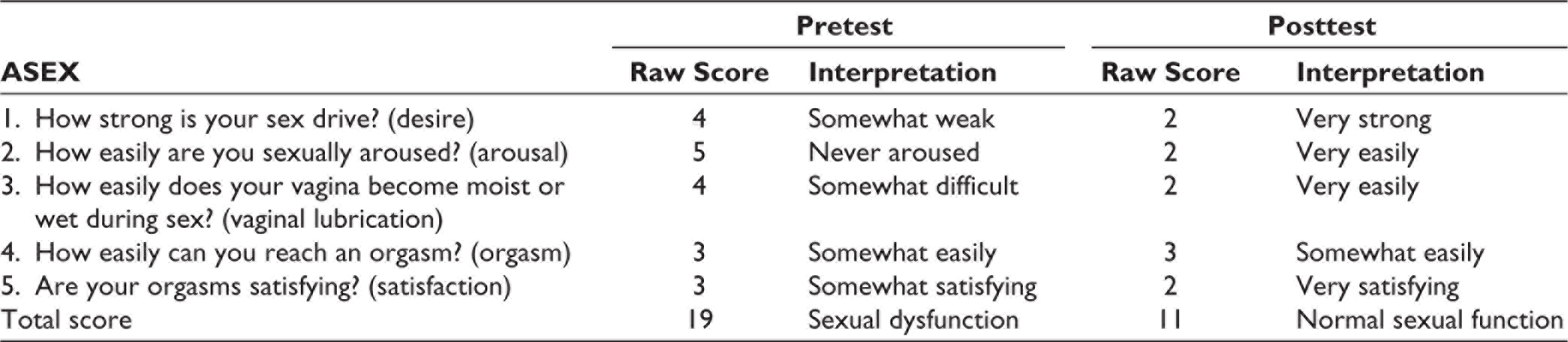
Client’s pretest result (see Table 1) showed that the total score of ≥19 on ASEX indicates sexual dysfunction, clients high score of ≥4 on sex drive (desire), score of ≥5 on sexual arousal, and score of ≥4 on vaginal lubrication indicates that client have significant difficulties in the area of sexual drive, arousal, and vaginal lubrication. While scores of ≥3 on orgasm and orgasm satisfaction subscale indicates that client somewhat easily reached orgasm and somewhat get satisfaction from orgasm. Client’s pretest result is in conformity with client’s DSM-5 diagnosis of female sexual interest/arousal disorder.
At posttest, client did not meet the diagnostic criteria for female sexual interest/arousal disorder based on DSM-5 which is in conformity with client’s scores on ASEX. The total score of ≥11 on ASEX indicates normal sexual functioning. Similarly, client’s low scores of ≥2 on sex drive, arousal, vaginal lubrication, and orgasm satisfaction indicates very strong desire, very easily arousal, very easily vaginal lubrication, and very satisfying orgasm respectively, while score of ≥3 on orgasm subscale indicates somewhat easily achieved orgasm (see Table 1).
Showing Clients Pre- and Posttest Scores on Arizona Sexual Experience Scale
Hypothesis 2
Frequency of sexual relationship will increase after online psychoeducation and CBT.
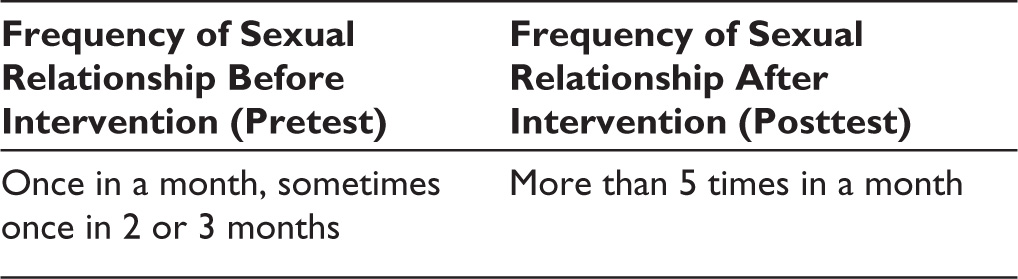
At baseline, client reported that she has sexual relationship with her husband once in a month, while sometimes it’s once in 2 or 3 months (see Table 2). Furthermore, client reported significant improvement in the frequency of sexual relationship with her husband after sessions 11, 12, 13, and 14. Similarly at follow-up, sessions 15, 16, and 17 client’s progress report showed significant improvement in the frequency of sexual relationship with her husband to more than 5 times a month (see Table 2). In response to a follow-up question “any challenge or difficulty at the moment?” during session 15 client responded “no difficulty, all is going on well even the frequency is good.”
Showing Frequency of Sexual Relationship Before and After Intervention
Discussion
This single case design investigates the efficacy of online psychoeducation and CBT on treatment of female sexual interest/arousal disorder. Findings of the study showed that client’s pretest and posttest results significantly differ after online psychoeducation and CBT. According to McGahuey et al, 18 a total score of ≥19 or any 1 item with individual score of ≥ 5 or any 3 items with individual scores of ≥4 is indication of the presence of clinically diagnosed sexual dysfunction. Client’s pretest result showed the presence of sexual dysfunction. Significantly, client’s posttest result both total scores and individual scores are below the required diagnostic criteria based on ASEX scores for sexual dysfunction to be diagnosed. Furthermore, after online psychoeducation and CBT intervention client did not meet DSM-5 diagnostic criteria for female sexual interest/arousal disorder, client reported improve sexual interest/arousal, and she could initiate sexual activity. Similarly, in a feasibility study, Zippan et al 15 reported improvements in sexual arousal, satisfaction, and desire among women with sexual interest/arousal disorder after online psychoeducation. Furthermore, Babakhani et al 10 in a randomized clinical trial reported that after cognitive behavior consultation, sexual functions significantly increase among control and intervention groups.
Outcome of the second hypothesis significantly showed that frequency of sexual relationship increased after online psychoeducation and CBT. At baseline, client reported that she has sexual relationship with her husband once in a month, while sometimes she had once in 2 or 3 months, but after online psychoeducation and CBT the frequency significantly improved to more than 5 times a month. The following statement “…all is going on well even the frequency is good” attests to the fact that the frequency of sexual relationship between client and her husband significantly improved. Canadian Psychological Association reported that CBT is the most frequently used short-term psychological intervention for sexual dysfunction. 8 Recently Mirzaee et al 13 reported that psychoeducational cognitive behavioural counselling has been found effective in improving female sexual function. CBT had positive impact on sexual dysfunction among women. 9 Among Iranian women, sexual performance improved after CBT. 7 Findings of this research revealed that aside the use of medication in the treatment of sexual dysfunction, psychoeducation and CBT are effective in the management of female sexual arousal/interest disorder and sexual dysfunction in general.
Conclusion
Findings of this single case design revealed that online psychoeducation and CBT is effective in the treatment of female sexual interest/arousal disorder. Clients posttest result showed significant improvement in DSM-5 diagnostic criteria for female sexual interest/arousal disorder and on client’s total ASEX scores and subscale scores. Furthermore, the frequency of sexual relationship monthly significantly improved compared to the frequency at baseline. This study is limited considering that it’s a single case design, which may affect generalization of the study outcome. However, this work contributes to the scientific community in the area of psychological intervention with emphasis on female sexual interest/arousal disorder. Thus, outcome of this study should guide clinical psychologists in the area of intervention for sexual disorder, especially among women. Also, outcome of this study will serve as reference material for women suffering with sexual dysfunction and it will also serve as an encouragement to women suffering from sexual dysfunction not to die in silence but sought for professional help. The author recommends that both women and men suffering from sexual dysfunctions should not die in silence but seek for professional help considering the efficacy of sex therapy in the management of sexual dysfunction. This article is relevant in clinical practice considering the prevalence of sexual dysfunction generally. Thus, those suffering from sexual dysfunction would consider sex therapy as an alternative option rather than just medication with emphasis on sex-focused psychoeducation and CBT taking advantage of online options which implies distance is not a barrier in seeking for help when it comes to sexual dysfunction generally.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.