
Abstract
Background:
Premature ejaculation (PE) is a common sexual disorder in male that negatively impacts their quality of life (QoL). The study aimed to evaluate the association of QoL with its four domains among patients with PE.
Methods:
It was a cross-sectional study conducted from November 2021 to October 2022 among patients above 18 years of age who fulfilled the diagnostic criteria of PE, attending the outpatient department of Psychiatry of Bangabandhu Sheikh Mujib Medical University (BSMMU). Patients who complained of PE were questioned with the Premature Ejaculation Diagnostic Tool (PEDT), and those who scored >11 in PEDT were interviewed with a Socio-Demographic Questionnaire, Bengali Version of Patient Health Questionnaire (PHQ-9) and World Health Organization Quality of Life Scale brief version (WHOQOL-BREF).
Result:
Among 140 participants who came for treatment of PE 122 (87.1%) had possible PE (PEDT score > 11) Among the four domains, the social relationship domain (11.23 ± 2.2) had the lowest mean score followed by psychological (12.25 ± 2.7), environmental (13.05 ± 2.22) and physical health (13.99 ± 2.6) domain. A total of 38 (31.1%) had mild, 32 (26.2%) had moderate, 11 (9%) had moderate severe and 7 (5.7%) had severe depression among the patients with PE. The study suggests that the QoL among the patients with PE is low. Illiteracy, living in a suburban area, smoking and inactive lifestyles, having previous physical illness and depression are the factors that are significantly associated with poor quality of life among the patients.
Introduction
Premature ejaculation (PE) is the most prevalent male sexual disorder, and the global prevalence of PE is estimated to be between 20% and 40%. 1 According to the International Society for Sexual medicine (ISSM) PE should include three aspects: (a) short intravaginal ejaculation latency time (IELT), (b) poor ejaculatory control and (c) negative sexual consequences in both patient and partner, for example, anxiety, depression, or decreased sexual desire. 2 An Egyptian study showed PE has a significant negative impact on patients and their partners, both individually and as a couple. There was a significant difference in some domains of the QoL of PE patients, such as feeling less like a man, embarrassment, guilt and rejecting partners. 3
Along with various social impacts, PE leads to significant negative psychological impacts in men, which affects their female partners as well. They suffer a lot in establishing new relationships. 4 It further leads to psychological burdens such as frustration, dissatisfaction, feeling of incompetence and depression. 5 A range of studies have shown depression is strongly associated with PE, proving their bidirectional relationship and having mutual pathophysiology. 6 The study also revealed that men suffering from PE tend to have lower levels of intimacy between couple compare to those men not having PE. The interpersonal distress deriving from PE may affect relationship with partner, self-esteem as well as self-confidence. 7 Thus, it hampers the social, emotional and intellectual aspects of their life. 8 Subjects with PE compared to non-PE had noticeably lower mean scores for perceived control over personal distress and difficulties related to ejaculation. 9 Many reviews have noted significant medical co-morbidities, along with psychiatric co-morbidities associated with PE. A Malaysian study discovered hypertension and diabetes mellitus as striking medical co-morbidities with PE. 10 Despite the significant prevalence and remarkable impact of PE on men’s quality of life (QoL), no prior study in Bangladesh has explicitly researched this issue in a tertiary-level hospital. Also, Bangladesh is a tradition-bound country. People view sex education and sexual activity as taboo to share and seek help. 11 So, drawing attention to a constructive approach to sexual health and highlighting its benefits should be acknowledged as a core component of an effort to improve overall health and well-being for all. 12
Methodology
Study Design and Participants
This cross-sectional study was conducted in the Department of Psychiatry from November 2021 to October 2022. Data were collected from the Outpatient Department of Psychiatry of Bangabandhu Sheikh Mujib Medical University (BSMMU).
All the participants who complained of PE above the age of 18 years were questioned with PEDT and whose score was >11 were included in the study. However, participants who did not provide verbal consent, who chose to withdraw their consent and whose PEDT score was ≤11 were excluded from the study. Following these inclusion and exclusion criteria 122 participants were finally included in this study.
Data Collection Tools
A semi-structured questionnaire ‘Quality of Life among men with Premature Ejaculation’ was used to measure socio-demographic and other related variables. The Bengali-validated instrument Premature Ejaculation Diagnostic Tool (PEDT) was used to identify PE. The PEDT is a diagnostic instrument for PE which contains five questions to assess ejaculation control, Frequency of PE, ejaculation with minimal sexual stimulation, distress and interpersonal difficulty. The total score ranges from 2 to 22. A total score >11 is suggestive of PE, where score ranging 9–11 are probable and score below 9 is considered as absence of PE. PEDT has been translated in Bangla and reliability and validity was tested. Cronbach’s Alpha was used to test internal consistency and it was 0.827 which indicate a good reliability. Test- retest correlation was measured by spearman rho; significant association was observed between two tests with Sperman’s rho value for total score was 0.87. Intraclass correlation coefficient was calculated as 0.943. The study’s construct validity was evaluated using Exploratory Factor Analysis, and the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was found to be 0.77.
13
Patient Health Questionnaire (PHQ-9) is a 09 items Likert scale and it was used in this study to measure the severity of depression.
14
Finally World Health Organization Quality of Life Scale, brief version (WHOQOL BREF
Procedure of Data Collection
The study approval was obtained from the BSMMU Institutional Review Board. Participants were informed about the purpose, method and outcome of the study. Informed written consent was taken from the participants before data collection. PEDT was applied to all participants who complained of PE; those who scored >11 were diagnosed with PE and sociodemographic data were collected from them by using the semi-structured questionnaire to identify the characteristics of the participants. Then, the Bengali Version of PHQ-9 and WHOQOL-BREF were applied to diagnose and evaluate the severity of depression and to assess the QoL among patients with PE, respectively. Data were collected by face-to-face interviews. The researcher read out the questions and marked the answers given by the participants who were not able to read. The participants had the right to stop the interview at any time, even without having to give a reason for stopping it.
Data Analysis
Data was analysed by Statistical Package for Social Science, SPSS (version 22). Frequency (n) and Percent (%) were used for sociodemographic variables (age groups, profession) to show the distribution of participants. Descriptive statistics (Mean ± SD and Min-Max) were used for QoL scores in different domains. One-way ANOVA was used to compare QoL scores across different age groups, professions, education levels, and living places. If P < .05, it means at least one group differs significantly. The effect size was seen by Eta-Squared (η²), indicating the proportion of variance in the dependent variable explained by the independent variable.
Result
In this study, 140 participants reported early ejaculation using PEDT; however, 4.3% of participants had a score of less than 09 (no PE) and 8.6% of participants had a score between 09 and 11 (probable PE). Both of the groups were excluded from the study. Finally, 122 (87.1%) participants with scores >11 were included in this study.
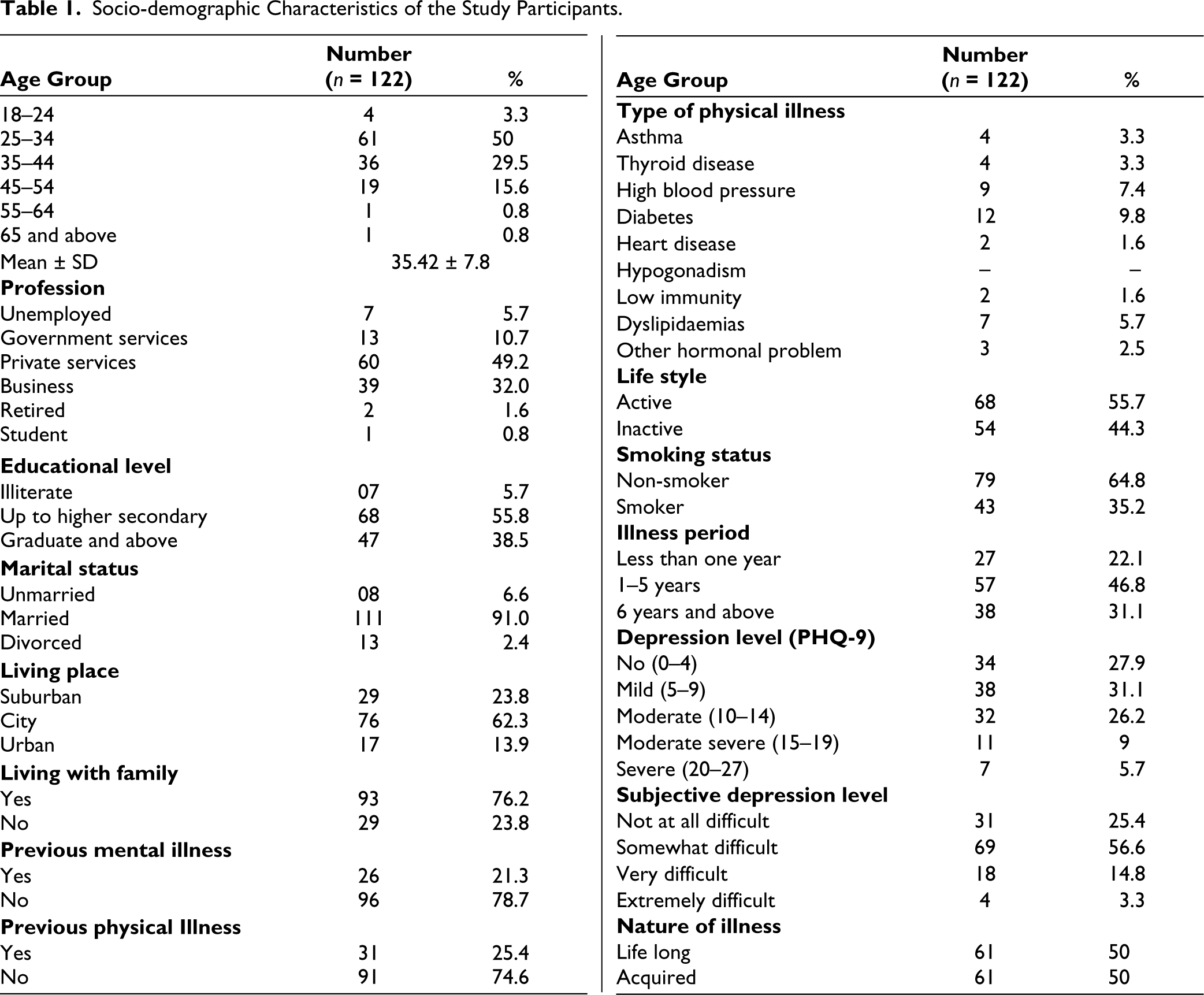
The participants’ ages were stratified in different age categories ranging from 18 to 65+. Most of the study participants were between 25 and 34 years, followed by the age group between 35 and 44 years. The mean age of the participants was 35.42. Most of the respondents were in private service and had studied up to higher secondary (55.8%). The majority were married (91%), 21% had a previous history of mental illness and 25% had a history of physical illness. Among the respondents, 35% were smokers. Diabetes (9.8%) and high blood pressure (7.4%) were the most common types of physical illness. Most of the participants had mild depression (31.1%), while 5.7% of participants were severely depressed. The duration of illness among the majority of the subjective depression expressed by the participants, the situation for most of the PE participants was ‘somewhat difficult’ (55%). Among the respondents, lifelong and acquired PE were equal (Table 1).
Socio-demographic Characteristics of the Study Participants.
The transformed QoL score (4–20) of the participants is shown in Table 2. For the participants with PE, the mean score of the physical domain was 13.99 (highest score of 4 domains), psychological was 12.25, social was 11.23 (lowest score) and environmental was 13.05 (Table 2).
Quality of Life of the Participants.

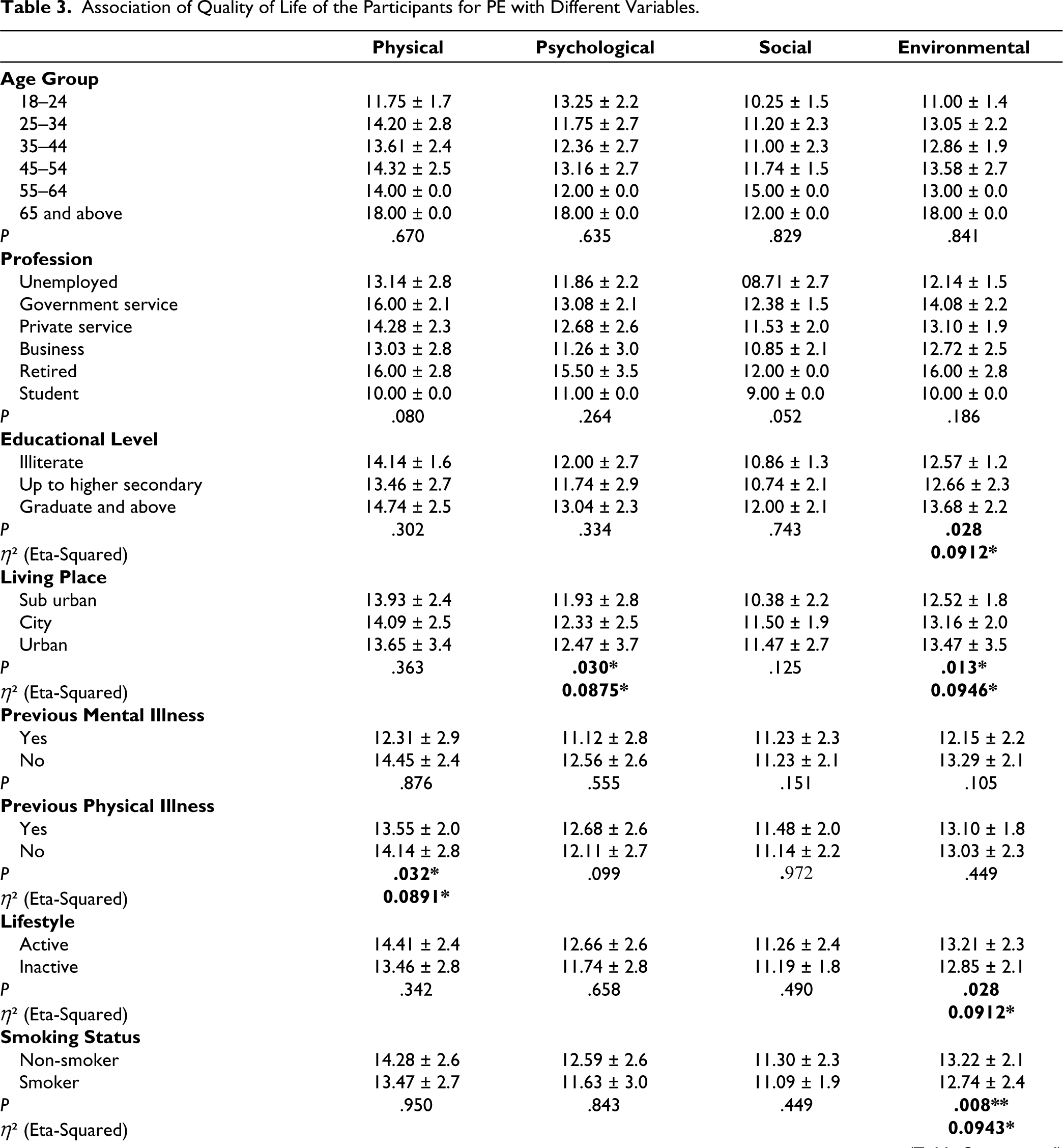
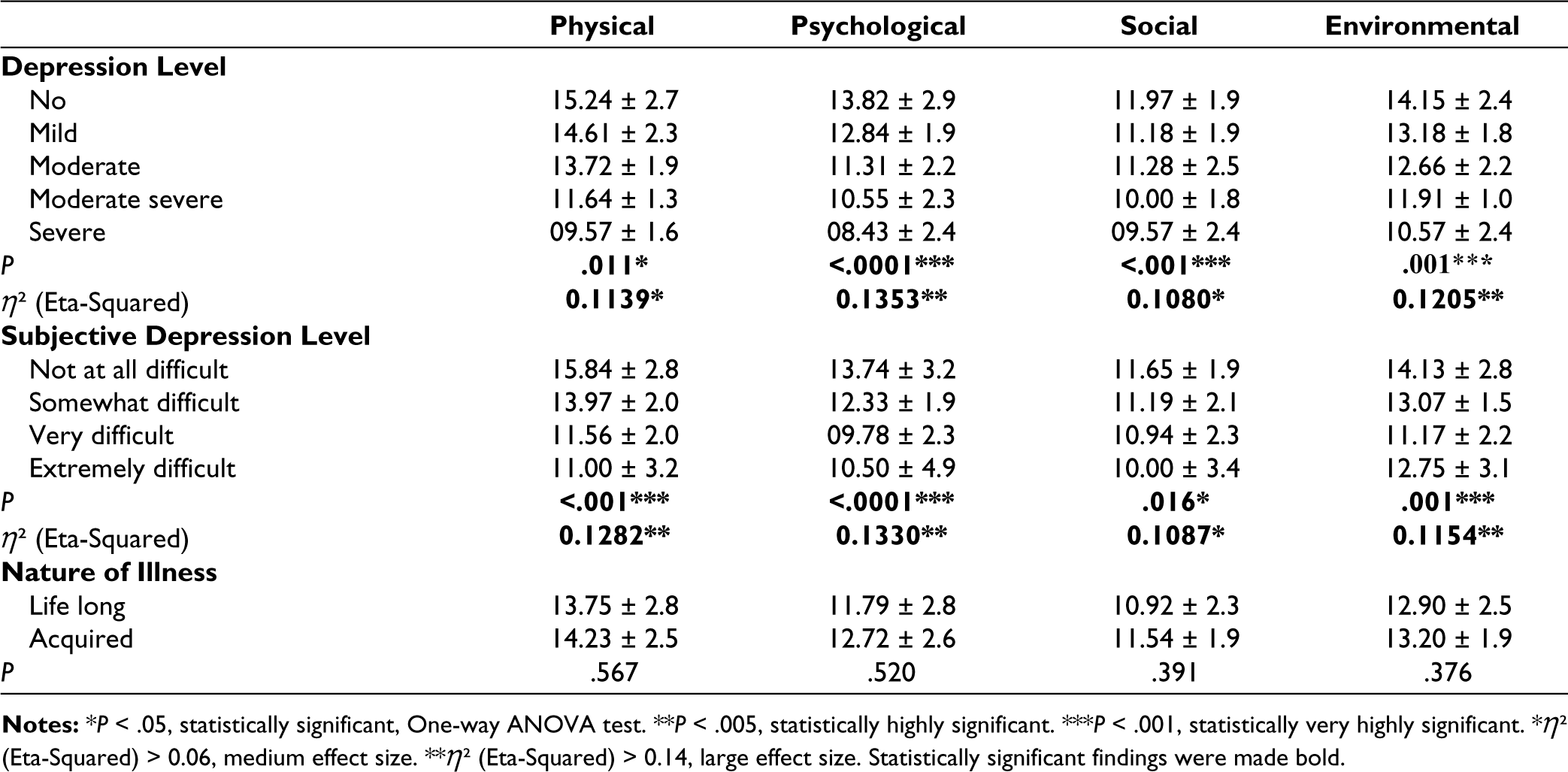
Table 3 shows the association of the four domains of QoL with different variables among PE participants. It was found that the environmental domain of QoL was significantly low among illiterate participants, whereas psychological and environmental domains were significantly low among the participants living in suburban areas. Participants who had previous physical illness scored significantly low in the physical health domain. Participants who had inactive lifestyles and who were smokers had poor QoL in the environmental domain. Participants with severe depression had poor QoL in all four domains, which was statistically very highly significant. All four domains of QoL were also low among participants with ‘very difficult’ subjective depression and ‘extremely difficult’ subjective depression. Marital status, living with family and duration of illness did not show any significant association with QoL of the participants (Table 3).
Association of Quality of Life of the Participants for PE with Different Variables.
Discussion
Our study aimed to evaluate four domains of QoL using WHOQOL-BREF among men with PE. Out of 140 patients, 18 patients were excluded as they have score £ 11. It indicated that many of the participants were concerned about their sexual problems but did not fulfil the criteria of PE. The mean scores of different domains of WHOQOL-BREF physical health, psychological, social relationships and environmental domains of QoL of participants with PE were 13.99, 12.25, 11.23 and 13.05, respectively, in the present study. In a study done in Kuantan Malaysia among 290 men, the proportion of PE was found 33.9%, and they had lower median scores in all four domains of QOL than those who did not have PE. 19 Another study conducted among the Egyptian population also showed PE negatively affects physiological, psychological, cultural and relationship domains of QoL. 3 Among the patients with OCD, mean standard deviation scores of physical health, psychological, social relationships, and environmental domains were 21.54, 18.17, 7.54 and 24.7, respectively. 17
Reduced self-esteem, psychological distress, shame, guilt, stress, anxiety, interpersonal difficulties and failure-related fear are some detrimental impacts that patients with PE experience. 20
Our study revealed that among the four domains, the social relationship domain was most affected among the participants with PE. Avoidance of sexual intimacy by the patient due to fear of failure and sexual dissatisfaction of the partner can result in relationship difficulties. 21 Along with this, low self-esteem, frustration, depression can cause a lack of social participation and engagement, which can cause poor social relationships.
In this study, half of the participants with PE belonged to the age group of 25–34 years and about 30% to 35–44 years with a mean age of 35.42 years. Half of them were in private service, 55.8% studied up to higher secondary level and 91% were married. A study done in Bangladesh among 51 patients suffering from PE showed similar sociodemographic characteristics where 39% of participants belonged to 30–40 years of age with a mean age of 34.8 years, 52.9% were service holders, 41.2% completed their graduation or post-graduation and 80% were married. 13
Among the participants with PE, 21.3% and 25.4% had previous mental and physical illnesses, respectively. Diabetes (9.8%) and high blood pressure (7.4%) were the most common physical illnesses reported by the participants, followed by dyslipidaemia (5.7%), asthma (3.3%), thyroid disease (3.3%). Harun & Ahmed also found hypertension (43.6%) and diabetes mellitus (32.2%) are the two most common co-morbidities of PE. 19 Contrarily, the prevalence of PE was noted higher among patients with diabetes and neurological, neurotransmitter, and psychological dysfunctions, which may be related to both of the conditions. 21 The severity of depression was also measured in this study using PHQ-9, which revealed that 31.1% of participants with PE had mild depression, 29.9% had no depression, 26.2% had moderate depression, 9% had moderately severe depression and 7% had severe depression. The prevalence of depression among patients with PE was 26.78% in a study, and it was mostly related to the duration of the illness. 22 A study done by Nagarale et al. using the Hamilton Depression Rating Scale (HDRS) revealed that there was mild depression, anxiety, reduced self-esteem and impairment in QoL among patients with PE. 23 The relationship between depression and PE is bidirectional. Both of the disorders might have a shared psychopathological basis. 6 Depression can negatively affect sexual function, and PE can also lead to low self-esteem, frustration and depression.
In the present study, half of the participants had lifelong and half had acquired PE. There were no significant differences in any domain of QoL between these two groups. A study done by Ermeç and colleagues showed that among 175 patients with PE, 62 had lifelong and 113 had acquired PE. QOL was also assessed using SF-36 among patients with lifelong PE, acquired PE and the control group without PE, which revealed the QoL in the lifelong and acquired PE groups was lower than the control group. It also showed that physical function, general perception of health, energy, role limitations due to emotional problem subscale of SF-36 were lower in patients with acquired PE than lifelong PE. 4
The association of different sociodemographic variables of the participants with the four domains of QoL was also examined in this study. The environmental domain of QoL was found to be significantly low among illiterate participants and participants living in suburban areas. Lack of a healthy physical environment, sufficient finances to meet daily needs, access to adequate information and health services might have contributed to this. Participants with PE who had previous physical illness scored significantly low in the physical domain of WHOQOL BREF, which can be due to pain, discomfort, fatigue, physical immobility and weakness associated with the physical illness. The present study has examined QoL with PE and depression. Another important finding of the present study was that participants with severe depression had significantly poor QoL in all four domains of WHOQOL BREF but very highly significant in psychological, social and environmental domain. Depression has some direct physiological impacts like—lack of appetite, insomnia, lack of libido, fatigue, which can be the reason for low scores in physical health domain. It also causes low self-esteem, feelings of guilt, and poor concentration, which might have caused poor scores in psychological domain. Lower scores in social relationship domain can be due to lack of social interaction and social withdrawal accompanying severe depression. Participants who were smokers and had inactive lifestyles scored significantly lower in environmental domain of WHOQOL BREF.
This study has some limitations that need to be addressed. First, PE was diagnosed using a diagnostic tool, PEDT. We relied solely on the participants’ responses to the questions rather than doing a complete medical evaluation. Second, this study gave only a snapshot of the condition as it was a cross-sectional study. A longitudinal study can be done to assess the overall QoL of participants with PE. Another major limitation was that the female partners of the participants were not evaluated in this study.
The study suggests the QoL among patients with PE is low. Illiteracy, living in a suburban area, smoking and inactive lifestyles, having previous physical illness and depression are the factors that are significantly associated with poor quality of life among the patients. So, depression and other physical illness should be treated simultaneously while treating patients with PE. In addition, lifestyle modifications like—improving physical activity and reducing smoking can be an integral part of the treatment plan to improve the QoL of patients with PE.
Footnotes
Data Availability
The data supporting this study’s findings are available from the first author (MSA) upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Review Board of Bangabandhu Sheikh Mujib Medical University. Approval ID: No.BSMMU/2021/13013.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study received financial support from the University Grants Committee of Bangabandhu Sheikh Mujib Medical University (BSMMU).
Informed Consent
Informed written consent was taken from the participants before data collection.