
Abstract
Over the past few decades, quality of life (QOL) has become an important concept in medical research and treatment practice in general. Different reasons are given for this development. First, newly invented medical techniques, though useful, often are at the same time (very) expensive. In times where financial resources are scarce and health-care professionals are made financially accountable for their decisions, outcome measures such as QOL can be of use in making choices in treatment policies. Second, evaluation of new drugs and treatments not only requires insight into outcome measures such as reduction of symptoms and occurrence of possible sideeffects, but also into the impact they have on the QOL of patients involved. Third, although developments in terms of diagnostics and treatments have produced a decline in mortality and morbidity rates accompanied by a prolongation of life, they have, nonetheless, often failed to achieve a restitutio ad integrum. This means that patients have to live, and come to terms, with long-lasting disabilities and handicaps. A consequence of this is that the use of the concept of QOL is growing, as classical medical endpoints, such as morbidity and mortality, not fully represent the potential outcomes of medical interventions [1–3].
The reasons mentioned above for the increasing interest in QOL can also be applied to the field of psychiatry. In addition to this, the fundamental change in Western mental health-care systems from institutionalized care to community care should be mentioned, as this development led to an increase in the interest in the effects of mental disorders on aspects of everyday life, QOL being one of the main outcome measures [4].
From the 1980s onwards, many instruments have been developed for the assessment of functioning in daily life. Although these instruments often are labelled as general ‘quality of life’ measures, strictly speaking, they assess health status. In health status research, the aim is to assess functioning itself (e.g. with questions like ‘Can you work for eight hours?’). In contrast, QOL research focuses on the personal evaluation of functioning (e.g. ‘Are you satisfied with your working capacity?’). Thus, while health status assesses peoples functioning, QOL concerns peoples evaluation of functioning.
The body of knowledge on the relationship between QOL and psychiatric disorders is growing. Several studies have demonstrated that the presence of psychopathology is negatively related to subjective experienced QOL. For instance, according to Schneier [5], ‘the anxiety disorders seem to impair QOL through the distress of anxiety itself, the avoidance behaviour related to anxiety, and the stigma attached to having emotional problems’. With regard to the QOL of schizophrenic patients, Bobes and González [6] concluded that ‘several studies have con- firmed the intuitive idea that patients with severe chronic mental illness have an impoverished quality of life, compared with that of the general population and other physically ill patients’. Simon [7] noted: ‘Abundant evidence demonstrates a strong cross-sectional association between depression and decrements in self-reported functional status or quality of life’.
In spite of the available results of studies such as mentioned above, understanding the complex relationship between psychopathology and QOL still remains diffi- cult owing to three reasons. First, according to the literature, QOL should be assessed in a comprehensive, culturally sensitive and subjective way, paying attention to the relative importance of its various facets [8–14]. However, in many studies QOL has not been assessed according to all these principles. Second, the assessment of both QOL and psychiatric disorders is often hampered by an overlap in content between symptoms and QOL measures [15]. Third, with regard to the field of psychiatry, numerous studies on QOL mainly concentrated on exclusively selected study populations [e.g. [5–7,16,17], hampering the applicability of the results in daily practice.
It can be expected that patients with (severe) psychiatric disorders use health-care facilities in an intense way during a long period of their life. At present, the costs for (newly developed) psychiatric treatments (e.g. drugs, psychotherapies, specialized clinical care) are high, while at the same time the financial means are limited. In determining cost-effectiveness of psychiatric treatment policies and in utility studies, an outcome measure such as QOL can be of great value, the more so as, apart from alleviation of symptoms, improvement of QOL is an important goal of treatment. For QOL to be useful as an outcome measure, the relationship between mental disorders and QOL should be determined in a profound way, while avoiding the limitations of earlier research mentioned above. Therefore, the aim of the present study was to get more and new insights into the relationship between QOL and psychopathology in such a manner. In accordance with the results of prior studies, it was hypothesized that QOL would be negatively related to the presence and the severity of psychopathology.
Method
Data for this study were derived from a random sample of a general population of Dutch adult psychiatric outpatients. These data were compared with scores of a random sample of the general Dutch population compiled from earlier studies [18]. In addition, comparisons of QOL scores were made within the group of psychiatric outpatients, in order to determine the relationship of psychiatric diseases, personality disorders and comorbidity with QOL. For this reason the group of psychiatric outpatients was subdivided into four subgroups, which are described below.
Psychiatric outpatients: setting and study population
The collection of data from the group of psychiatric outpatients was conducted at GGZ-Midden Brabant, the community mental health centre in Tilburg, the Netherlands. Approval was received from the Medical Ethical Committee of the Southern Netherlands. Participants were outpatients of Dutch ethnic origin, aged 21–50 years. They were referred to the centre in the period from 1 March 2001 till 1 March 2002. Potential participants entered the study through a random selection procedure in which a third of all referrals was selected directly for psychiatric evaluation. After complete description of the study to the participants, written informed consent was obtained. Exclusion criteria were inability to undergo the various verbal and written parts of the investigation protocol (interviews and questionnaires) owing to severe mental illness, illiteracy, dyslexia, mental retardation, problems with sight or hearing and cerebral damage.
Random sample of the general Dutch population: procedure of data collection
The reference population was taken from a pooled data set (n=593) based on Dutch general population studies, collected between 1999 and 2002 at Tilburg University. For the present study, participants aged 21– 50 years were selected. This resulted in a group consisting of 403 persons.
Division of the psychiatric outpatients into subgroups: procedure
The group of psychiatric outpatients was subdivided in the following way.
Participants who did not obtain a diagnosis according to DSM-IV on either Axis I or Axis II after psychiatric evaluation (method of evaluation: see under subheading ‘Instruments’), were placed in the group ‘non-case’ (group A); participants, who were diagnosed with one or more diagnoses, according to DSM-IV on Axis I and/or Axis II after psychiatric evaluation, constituted the group ‘case’ (group B).
Furthermore, the group ‘case’ was subdivided into two subgroups: ‘single axis morbidity’ (group C) and ‘comorbidity’ (group D). Group C consisted of participants with one or more diagnoses, according to DSM-IV classification on either axis I (group C-1) or Axis II (group C-2). The group ‘comorbidity’ contained participants diagnosed with one or more diagnoses, according to DSM-IV classification on both Axis I and Axis II.
Instruments
Participants completed the Dutch version of the WHOQOL-Bref [19], a questionnaire for assessing QOL. In addition, they underwent two semistructured interviews in order to obtain both the Axis-I and Axis-II diagnoses, according to DSM-IV. The interviews were held in two separate sessions: one session for obtaining the Axis-I diagnosis and one for the Axis-II diagnosis. They were administered by two psychiatrists (EDM, FJT) trained and certified at the WHO centre in Groningen, the Netherlands.
The WHOQOL-Bref
In 1991, the World Health Organization (WHO) started a project entitled ‘The assessment of QOL in health care’. The aim was to develop an internationally applicable, cross-culturally comparable, generic and multidimensional instrument for the assessment of QOL. The instrument was developed simultaneously in 15 centres around the world, including the Netherlands (Tilburg University being the Dutch participating centre) [18, 19]. The questionnaire was labelled the World Health Organization Quality of Life assessment instrument (WHOQOL). In this project, QOL was defined as ‘individuals’ perception of their position in life within the context of the culture and value systems in which they live, and in relation to their goals, expectations, standards, and concerns' [20]. The WHOQOL project has resulted in the development of the WHOQOL-100 [19, 21, 22] and, more recently, the WHOQOL-Bref [23]. The WHOQOL-100 allows a comprehensive assessment of QOL, but is sometimes in a practical sense too cumbersome, for example, in large epidemiological studies. Therefore, the WHOQOL-Bref was developed to enable a brief, but accurate, assessment of QOL in routine clinical work, large scale epidemiological studies and clinical trials [23]. It is a generic, multidimensional measure for subjective assessment of QOL, designed for use in a wide spectrum of psychological and physical disorders [14]. The WHOQOLBref comprises one question from each of the 24 facet scales in the WHOQOL-100 that belong to one of the four domains (Physical Health, Psychological Health, Social Relationships and Environment) and two questions from the Overall Quality of Life and General Health facet of the WHOQOL-100. The questions have a 5-point Likert scale. The time of reference is the preceding 2 weeks. In a previous study, domain scores of the WHOQOL-Bref were found to correlate highly with the WHOQOL-100 domain scores. We used the four-factor structure of the WHOQOL-Bref that was also found during development of the WHOQOL-Bref and in an earlier study in a general population of psychiatric outpatients [24]. The WHOQOL-Bref has good reliability, content validity and construct validity [24, 25].
DSM-IV, Axis-I diagnosis
For the Axis-I diagnosis, the Schedules for the Clinical Assessment in Neuropsychiatry (SCAN 2.1) were used [26, 27]. The SCAN is a comprehensive semistructured diagnostic interview developed under auspices of the WHO and aimed at the assessment and classification of psychiatric disorders in adults [27, 28]. Most of the studies about the psychometric properties of the SCAN have only examined earlier versions or parts of the current version [29, 30]. Rijnders et al. [31] tested the psychometric properties of the integral SCAN 2.1. Overall reliability was qualified as moderate to substantial and, with regard to the test– retest situation, as fair to moderate. In the standardized situation using videotaped interviews by experts, sensitivity as well as specificity proved to be substantial to almost perfect.
DSM-IV, Axis-II diagnosis
For the Axis-II diagnosis, the Structured Clinical Interview for DSMIV Axis II Personality Disorders (SCID-II, 2.0) [32, 33], Dutch version [34], was used. The SCID-II, 2.0 is a semistructured interview with 140 items, organized by diagnosis, covering the 10 personality disorders included in DSM-IV Axis II and the two personality disorders listed in the DSM-IV Appendix (i.e. diagnoses requiring further study). The instrument provides categorical diagnoses and dimensional scores for each disorder. With regard to the psychometric properties, Maffei et al. [35] investigated the interrater reliability and internal consistency. Interrater reliability was good for categorical diagnoses as well as dimensional diagnoses. Internal consistency for the dimensional scales proved to be satisfactory. The SCID-II interviews also were administered by two psychiatrists (EDM, FJT) and were trained for this specific purpose.
Statistical procedures
For the group of psychiatric outpatients and its subgroups and for the group of healthy controls, mean scores (with standard deviations) were calculated of the domains and the Overall Quality of Life and General Health facet of the WHOQOL-Bref. Differences between groups in these scores were examined using one-tailed independent sample t-tests. A p-value of 0.01 or lower was considered statistically significant. In addition, discriminant analyses were performed in order to investigate if, and to what extent, QOL outcome scores could predict whether participants belonged to the psychiatric outpatient or general Dutch population group and whether they were a case or a non-case. The data were processed using the Statistical Package for the Social Sciences (SPSS, version 10.0 for Windows, SPSS, Chicago, IL, USA).
Results
Psychiatric outpatients: sample characteristics
During the 1-year period, 3892 people (male: 40.4%; female: 59.6%) were referred to the outpatient clinic of the centre. About half of them (n=1559) were potential participants (male: 42.2%; female: 57.8%). The total group that entered the present study after random selection contained 438 participants (male: 42.7%; mean age: 34.7 years, SD=8.3; female: 57.3%; mean age: 32.8 years, SD=8.2). From this group, 28 participants were unable to undergo the research protocol owing to severe psychotic disorder (n=7), major depressive episode (n=9), dyslexia (n=2), mental retardation (n=2) and refusal to participate (n=8; four diagnosed with antisocial personality disorder; four with substance related disorder). Thus, 410 participants completed the test booklet (total response rate: 93.6%; male: 41.2%; mean age: 34.8 years, SD=8.4; female: 58.8%; mean age: 32.5 years, SD=8.2).
From this group, 54 participants (13.2%) were placed in group A, the other 356 participants (86.8%) in group B. Group B was further subdivided into the groups C (n=224) and D (n=132). Finally, group C was subdivided into the groups C1 (n=150) and C2 (n=74).
General Dutch population: sample characteristics
The group ‘general Dutch population’ contained 403 participants of Dutch ethnic origin, aged 21–50 years (male: 22.3%; mean age: 37.5 years, SD=7.6; female 77.7%; mean age: 37.1 years, SD=8.2). The substantial differences in the sex-ratio between the group general Dutch population and the group psychiatric outpatients, could bias comparisons of QOL outcome scores of both groups. To avoid this possible bias, the general Dutch population group was matched for this ratio, prior to analyses. For this purpose, 128 (out of the 313) females were randomly selected for further analyses. The final group general Dutch population contained 218 participants (male 41.3%; mean age: 37.5 years, SD=7.6; female 58.7%; mean age: 37.4 years, SD=8.2).
Psychiatric outpatients versus general Dutch population
The general Dutch population group had significantly (p<0.001) higher scores on all the WHOQOL-Bref domains and on the facet Overall QOL and General Health (see Table 1). The results of the discriminant analyses revealed a correct classification of 78.5% of the psychiatric outpatient group and 83.9% of the general Dutch population group. In total, 80.2% of the participants from the psychiatric outpatient and general Dutch population groups was correctly predicted to belong to those respective groups.
Scores on the WHOQOL-Bref: general Dutch population group versus psychiatric outpatient group
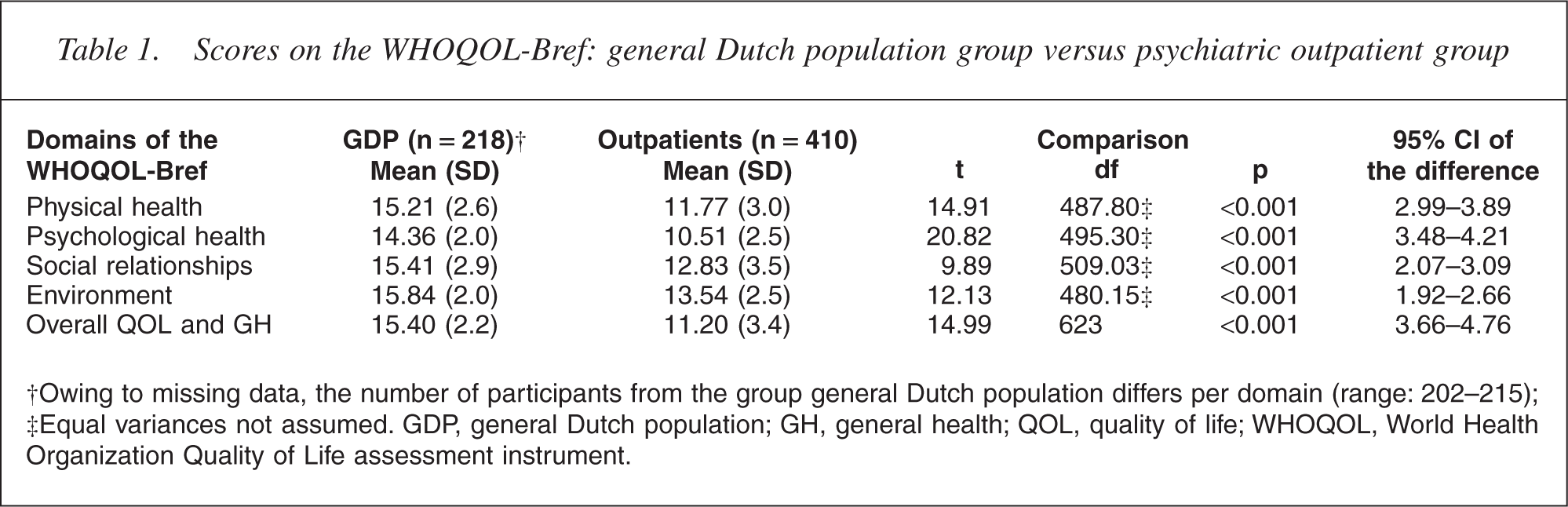
†Owing to missing data, the number of participants from the group general Dutch population differs per domain (range: 202–215);
‡Equal variances not assumed. GDP, general Dutch population; GH, general health; QOL, quality of life; WHOQOL, World Health Organization Quality of Life assessment instrument.
Comparisons within the psychiatric outpatient group
On all aspects of the WHOQOL-Bref significant differences (p<0.001) were found between group A (non-case) and B (case). Group A had the highest scores on all domains and on the Overall QOL and General Health facet (see Table 2). The discriminant analyses revealed that 66.7% of the cases from group A, 71.6% of those from group B and 71.0% of the total of cases from group A plus B were correctly classified. The results of the comparison between persons with a single axis morbidity (group C) and persons with comorbidity (group D) are shown in Table 3. On all domains and the single facet of the WHOQOL-Bref group D had the worst QOL scores (p<0.01). Compared with the subgroup of outpatients with only Axis-II morbidity (group C2), participants diagnosed with only Axis-I morbidity (group C1) scored significantly higher on the domain Environment (p<0.01) (see Table 4).
Scores on the WHOQOL-Bref: case (group B) versus non-case (group A)
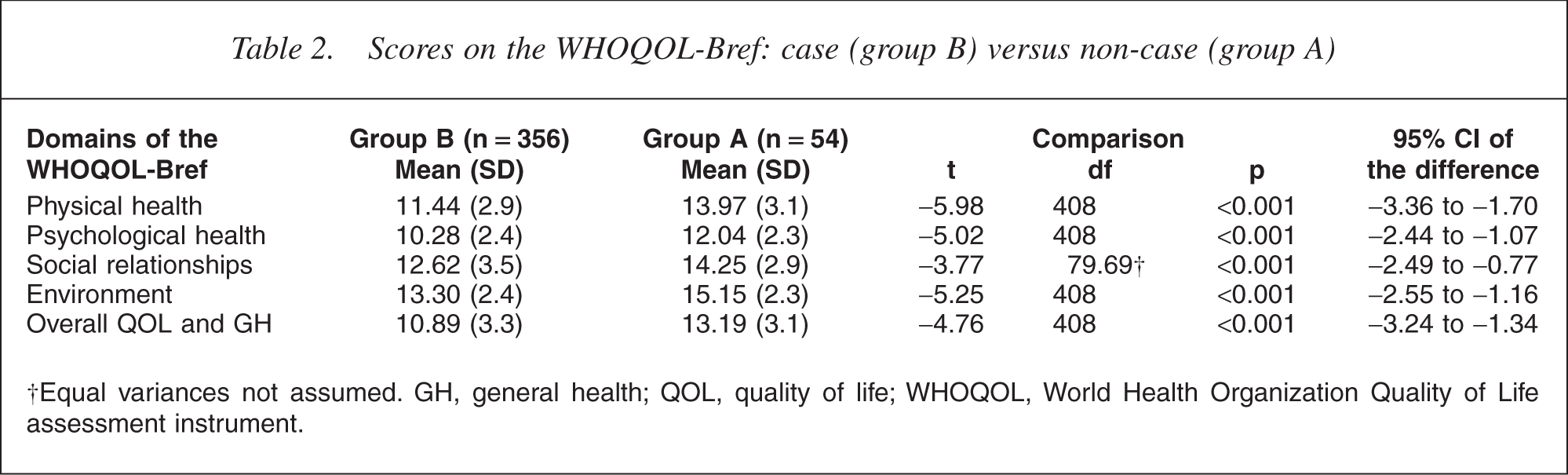
†Equal variances not assumed. GH, general health; QOL, quality of life; WHOQOL, World Health Organization Quality of Life assessment instrument.
Scores on the WHOQOL-Bref: single axis morbidity† (group C) versus comorbidity‡ (group D)
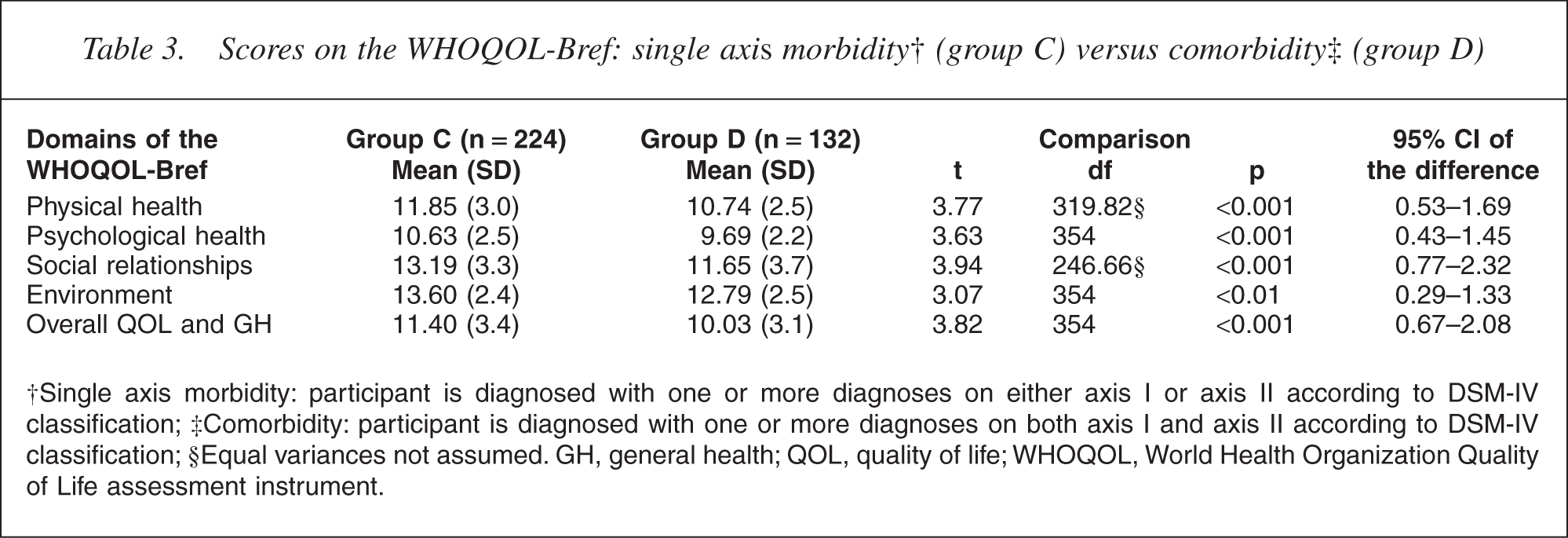
†Single axis morbidity: participant is diagnosed with one or more diagnoses on either axis I or axis II according to DSM-IV classification; ‡Comorbidity: participant is diagnosed with one or more diagnoses on both axis I and axis II according to DSM-IV classification; §Equal variances not assumed. GH, general health; QOL, quality of life; WHOQOL, World Health Organization Quality of Life assessment instrument.
Scores on the WHOQOL-Bref: Axis-I-morbidity† (group C1) versus Axis-II-morbidity‡ (group C2)
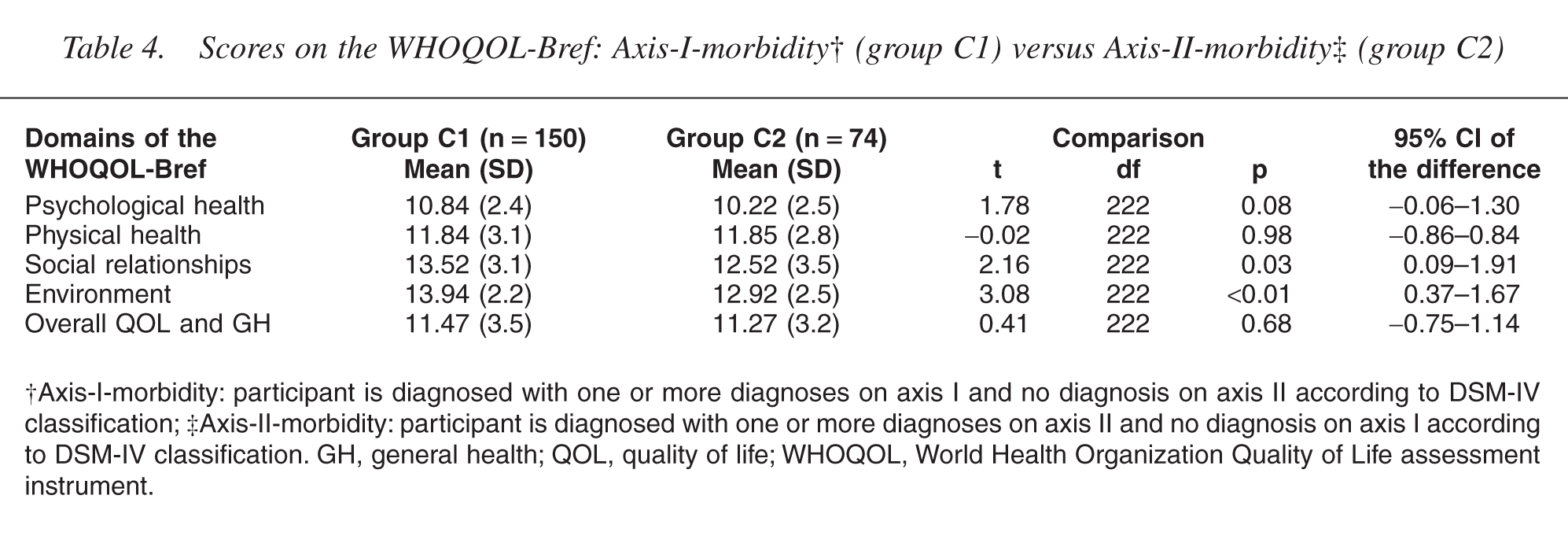
†Axis-I-morbidity: participant is diagnosed with one or more diagnoses on axis I and no diagnosis on axis II according to DSM-IV classification; ‡Axis-II-morbidity: participant is diagnosed with one or more diagnoses on axis II and no diagnosis on axis I according to DSM-IV classification. GH, general health; QOL, quality of life; WHOQOL, World Health Organization Quality of Life assessment instrument.
Discussion
The objective of the present study was to get more and new insights into the relationship between QOL and psychopathology. Limitations of earlier research on this subject, as mentioned in the introduction, were avoided as much as possible. First, QOL was assessed by using the WHOQOL-Bref, a comprehensive, culturally sensitive and subjective measure, which pays attention to the relative importance of the various aspects of QOL and has good psychometric properties. Second, the WHOQOL-Bref has a relatively small overlap in content between symptoms and QOL facets [14, 24]. Third, with regard to the study population, it was decided to take a random (thus not exclusively selected) sample of a general population of adult psychiatric outpatients. WHOQOL-Bref scores of the study population were obtained. These scores were compared with the scores of a sample of the general population. Also, comparisons were made between subgroups of psychiatric outpatients, using Axis I and Axis II morbidity, according to DSM-IV as discriminant variables. It was hypothesized that QOL would be negatively related to the presence as well as the severity of psychopathology. In general, the results of the present study supported this expectation.
In comparison with the general Dutch population group, the psychiatric outpatient group had worse scores on all domains of the WHOQOL-Bref. Among the psychiatric outpatients, participants with a psychiatric diagnosis, according to DSM-IV (group case) had worse scores on all QOL aspects compared with those without such a classification (group non-case). Within the group case, differences in QOL scores appeared. Participants who had only Axis-I morbidity scored better on the domain Environment, compared with participants who were classified with only diagnoses on Axis II. The worst scores on all domains of the WHOQOL-Bref were obtained by participants with comorbidity. Thus, in accordance with our expectations (i.e. that QOL would be negatively related to the presence as well as the severity of psychopathology), a gradual decrease in QOL scores was found, ranging from the highest QOL scores for the general population and the lowest for the psychiatric outpatients with comorbidity.
The results of the present study are not fully comparable with those of prior studies owing to differences in study population and/or assessment of QOL. Nevertheless, our finding that the presence of psychopathology is negatively related with subjective experienced QOL, is in accordance with earlier research [5–7]. The results of previous studies concerning QOL of patients suffering from mental disorders, in which QOL was assessed using the WHOQOL-100 or the WHOQOL-Bref are also in accordance with the results of the present study. The few existing studies with the WHOQOL-100 among patients with psychiatric disorders almost all focus on depression. For instance, Angermeyer et al. [36] investigated the QOL of patients with a depressive disorder using the WHOQOL-100 1, 4 and 7 months after their discharge from hospital. They found that, compared with patients with persisting depression, the QOL of patients with depression in remission was better. However, the QOL of the latter group still remained slightly worse compared with a random sample of the general population, even 7 months after discharge. Bonicatto et al. [37] used the WHOQOL-100 for the assessment of QOL in a sample of ambulatory depressed patients, who met DSM-IV criteria for current major depression. QOL was found to be significantly poorer compared with healthy persons and individuals with chronic somatic pathologies (i.e. lumbalgia due to benign processes, hypertension treated on an outpatient basis and breast cancer in remission). Skevington and Wright [38] examined changes in QOL in patients with moderate depression who received antidepressant medication. It was concluded that QOL increased significantly in the 8 weeks after the start of the antidepressant medication. Until now, research with the WHOQOL-Bref focused mainly on healthy subjects and patients with somatic disorders [e.g. [39–42]. Studies with the WHOQOL-Bref among patients with psychiatric disorders are scarce and are mainly focused on psychosis, which is associated with poor QOL [43–45].
The present study adds to the body of knowledge about the relationship between QOL and psychopathology. Its surplus values lie in the examination of a general population of psychiatric outpatients, the use of a control group and the extensive diagnostical procedure in which not only Axis I diagnoses but also Axis II diagnoses of the participants were assessed. The study results demonstrate that QOL is not only related to the presence of psychopathology but also to its severity. In particular, the presence of personality disorders was negatively related to subjectively experienced QOL. The assessment of both mental disorders and QOL could be hampered by an overlap in content between symptoms and QOL measures [15]. However, such an overlap is an unlikely explanation for the relations found in the present study, because of the use of the WHOQOL-Bref for the assessment of QOL [14, 24]. The present correlational study cannot determine whether the connection between personality disorders and QOL is a direct causal one, or whether personality disorders lead to certain lifestyles that, in turn, cause poor QOL. However, experimental studies involving mood induction have shown that personality has a direct effect on emotions and, even under controlled circumstances, individuals respond differently to the emotional events in their lives, depending on their personalities [46]. This suggests that the relationship between personality disorders and QOL is a direct causal one.
Quality of life can be used as an outcome measure in assessing the (cost)effectiveness and relative merits of different treatments of psychiatric patients, in health services evaluation and in clinical (psychopharmacological) trials. Moreover, the relationship and the interaction between the doctor and the psychiatric patient may improve, as the psychiatrist's understanding of how the psychiatric disease affects the patient's QOL increases. The implication for using QOL in clinical practice, is that treatment not only should concentrate on an alleviation of psychiatric symptoms, but also should direct towards pathology of personality. If QOL is used as an outcome measure in research and clinical practice in psychiatric medicine, the complex relationship between psychopathology and QOL has to be clarified in a profound way. The present study contributes to this subject by trying to overcome the limitations of earlier research.