
Abstract
Objective:
In Bangladesh, the factors that contribute to the reduced quality of life were not systematically investigated in long-term stroke survivors, and only a few studies have used preference-based measures to assess the quality of life. We sought to assess the quality of life in stroke survivors who comprise physical health status, psychological state, social relationship, and surrounding environment of the stroke patients.
Methods:
The quality of life among stroke patients was assessed with a semi-structured questionnaire using the validated Bangla Version of the World Health Organization, Quality-of-Life scale among the patients who survived beyond 28 days of first-ever stroke occurrence presenting in the Department of Physical Medicine and Rehabilitation, Bangabandhu Sheikh Mujib Medical University in the period between November 2020 and October 2021.
Results:
Of the 77 patients who were identified as post-stroke patients, the mean score of overall quality of life (as assessed by Q1 and scored in a range of 1–5) was 3.14 ± 1.08. The mean scores of quality of life were highest for the psychological domain (51.18 ± 19.73) followed by environmental (52.08 ± 13.13), social (45.62 ± 22.73), and physical domains (37.18 ± 18.56). According to the classification of the Bangla Version of the World Health Organization, Quality-of-Life, 75.3% had a low physical quality of life, 37.7% had a low psychological quality of life, 53.2% had a low social quality of life, and 53.2% had a moderate environmental quality of life. The average scores for the physical, psychological, social, and environmental domains were notably lower in stroke survivors with comorbid chronic conditions such as hypertension, diabetes, heart disease, asthma or chronic obstructive pulmonary disease, obesity, and ischemic heart disease in comparison to those without such conditions.
Conclusion:
In our study, post-stroke patients with lower quality of life were associated with factors such as female gender, lower level of education, urban dwellers, and chronic diseases.
Introduction
Stroke is the second most common cause of death globally and a significant contributor to disability. 1 Globally, approximately 15 million individuals experience a stroke annually, resulting in 5 million deaths and an additional 5 million individuals left with permanent disabilities. 2 As a sudden occurrence, stroke has an equal impact on both the individual and their family, catching them off guard in terms of coping with the resulting disabilities. 3 The conventional stroke outcome assessments are limited to measuring the neurological impairment and functional disability failing to evaluate the overall influence of the event on a patient’s well-being. 4 Quality of life (QoL) measurements are therefore more relevant to patients’ well-being which also acts as an important index of outcome after a stroke that can facilitate a broader description of the disease and outcomes. 4
The concept of health-related QoL was defined as how well a person functions in their life and his or her perceived well-being in physical, mental, and social domains of health. 4 Previous studies have indicated that the QoL can decline by over 40% following a stroke episode. 5 Consequently, assessing the QoL is regarded as a crucial measure of stroke outcomes. A previous study conducted in a rural region of North Kerala examined the QoL of 40 stroke survivors. Results revealed that only two individuals (5%) were fully independent, while the majority required varying degrees of assistance, with a few being bedridden. 6 Another study identified the key determinants of QoL for stroke patients at the 16-month mark, which included functional status, age, and gender. 7
Furthermore, it has been observed that approximately one in five stroke survivors live for at least 15 years, yet a significant proportion of these long-term survivors experience poor functional, cognitive, and psychological outcomes. 2 Developed countries have made advancements in stroke prevention, acute treatment, and neuro-rehabilitation over the past three decades, resulting in a reduction in the burden of stroke. 8 The overall incidence of stroke in Asia ranges from 116 to 483/100,000 per year. 9 According to the World Health Organization (WHO), Bangladesh stands in the 84th position for mortality rate due to stroke in the world. 10 In Bangladesh, the age and sex-standardized mortality rate of stroke is 54.8 per 100,000, and disability-adjusted life years’ loss is 888.1 per 100,000. 11 The huge burden of stroke patients causes long-term economic impacts on individuals, families, and the country. 10 Despite the high prevalence of stroke survivors, no study on the impact on QoL has been done in Bangladesh. Moreover, the factors that contribute to the reduced QoL were not systematically investigated in long-term stroke survivors, and only very few studies have used preference-based measures to assess QoL. Therefore, this study was designed to assess the QoL among stroke survivors, which can help develop more comprehensive and targeted interventions designed to maximize their recovery and suggest rational health care and rehabilitation planning for a huge number of stroke survivors in our country.
Methods
Instrument
The WHO has developed a quality-of-life measurement instrument, a validated Bangla Version of the World Health Organization, Quality-of-Life (WHOQOL-BREF) scale, which captures the subjective aspects of the QoL. 12 The WHOQOL-BREF is one of the best-known instruments that has been developed for cross-cultural comparisons of QoL which is available in more than 40 languages. 12 It is a multidimensional medical study questionnaire. In the present cross-sectional study, the QoL was assessed with a semi-structured questionnaire using a pre-tested and validated Bangla version of the QoL (WHOQOL) scale. This scale is divided into four domains along with four facets incorporated within the domains. 13 The four-domain score it derives denotes an individualized perception of QoL in each particular domain. Domain scores were scaled in a positive direction and higher scores denote a higher QoL. The mean score of items within each domain was used to calculate the domain score. Mean scores were multiplied by 4 to make domain scores comparable with the scores used in the WHOQOL. 14
Participants and setting
A total of 77 patients with diagnosed stroke (at least 28 days after the occurrence of stroke) who returned for a follow-up at the Department of Physical Medicine and Rehabilitation were enrolled in this study. The inclusion criteria include age more than 18 years, both sexes, first-ever stroke cases who survived more than 28 days of stroke occurrence, and patients willing to participate in the study. On the other hand, transient ischemic attack, comorbid conditions such as known end-stage renal disease, cirrhosis of the liver, cancer, disabilities prior to the occurrence of stroke, inability to speak, dementia, and diagnosed psychiatric disorders were considered as exclusion criteria for the participants. Consent was obtained from each participant who could make decisions and provide informed consent, or from their legally authorized representative if they were unable to make decisions themselves. After enrolment, their details regarding demographic profile such as age, sex, educational status, and monthly income were collected. In addition, risk factors before the strokes and subtypes of strokes were extracted from previous medical records. The following parameters were measured in the general physical examination, blood pressure, heart rate, weight, height, and waist circumference. In the neurological assessment, the presence and severity of limb and face paresis and speech disorders were evaluated. The cross-sectional study was conducted from November 2020 to October 2021. The independent variables include age, sex, occupation, economic status, level of education, residence, and risk factors, whereas the dependent variable includes QoL in stroke survivors.
Study flow chart:

The sample size calculation:
n = (z2 pq)/d2
n = the desired sample size
p = the proportion of the target population estimated to have particular characteristics. The reported prevalence of stroke in Bangladesh is 0·3% 11
q = (1−p) = (1–0.3) = 0.7
z = at 5% level of significance or 95% confidence level, z = 1.96
d = degree of accuracy or acceptable error usually set as 10% (0.1)
So,
n = [(1.96)]2 (0.3) (0.7)/(0.1)2 = 80.67
Statistical analysis
Following data collection, the collected data were assessed for completeness, accuracy, and consistency before analysis was commenced. Data analysis was carried out using SPSS version 26 (IBM Corp., Armonk, NY, USA). Exploratory data analysis was carried out to describe the study population, where categorical variables were summarized using frequency tables. By contrast, continuous variables were summarized using measures of central tendency and dispersion such as mean, median, percentiles, and standard deviation. Qualitative or categorical variables were compared using a chi-square test while an independent Student’s t-test was employed to compare continuous variables. A level of p < 0.05 was considered statistically significant.
Ethical considerations
Ethical approval for this study was obtained from the Internal Review Board of Bangabandhu Sheikh Mujib Medical University (approval no: BSMMU/2021/7953; date: 01 September 2021). Informed written consent was taken from each participant before starting the interview which contains details about the aim and objectives of the study procedure, benefits and risks for the participants, right to refuse to participate or withdraw from the study, confidential handling of data, and the responsible principal investigator’s identity. No compensation was given to the participants for the loss of their time as involved in the body. All participants’ signature was collected before the onset of research. This study does not cause any physical, social, or psychological risk to the participants.
Result
The mean ± standard deviation (SD) age of the persons with stroke was 52.58 ± 11.49 years. The majority of patients with stroke were found in the group 41–50 years (37.7%) followed by 29.9% in the group 51–60 years (Figure 1). According to the classification of WHOQOL-BERF, 75.3% (n = 58) participants had low physical QoL, 37.7% (n = 29) had low psychological QoL, 53.2% (n = 41) had low social QoL, and 53.2% (n = 41) had moderate environmental QoL (Table 1). The mean score of overall QoL (as assessed by Q1 and scored in a range of 1–5) was 3.14 ± 1.08 which was higher than the middle possible score (i.e. score 3) (Table 2). The mean scores of QoL were highest for the psychological domain (51.18 ± 19.73) followed by environmental (52.08 ± 13.13), social (45.62 ± 22.73), and physical domains (37.18 ± 18.56) (Table 2). In the physical domain, QoL was found higher in the ⩽40 years of age group (40.8 ± 20.39), female sex (36.65 ± 19.01), and married persons (38.22 ± 18.97) (Table 3). In this domain, the urban population had significantly higher QoL (41.08 ± 20.22) than the rural (p = 0.017) population (Table 3). In the psychological domain, QoL was found higher in the ⩽40 years of age group (55.10 ± 17.31), male sex (52.21 ± 19.86), married persons (51.84 ± 20.22), and urban population (54.85 ± 20.93) (Table 3). In the social domain, QoL was found higher in the 61–70 years of age group (70.33 ± 2.65; p < 0.001), male sex (46.38 ± 18.52), single person (46.75 ± 43.84), and urban population (46.58 ± 22.69) (Table 3). In addition, in the environmental domain, QoL was found higher in the 61–70 years of age group (66.33 ± 3.16; p < 0.001), male sex (52.50 ± 14.19), and married persons (52.48 ± 12.31) (Table 3). In this domain, the rural population had higher QoL (52.28 ± 10.98) than the urban population. We assessed comorbidity distribution among the patients and observed the following findings: 51.9% of patients had been diagnosed with hypertension (HTN), 26.0% had diabetes mellitus (DM), 19.5% had dyslipidemia, and 18.2% had a history of ischemic heart disease (IHD; Figure 2). The average scores for the physical, psychological, social, and environmental domains were notably lower in stroke survivors with comorbid chronic conditions such as HTN, DM, heart disease, asthma or chronic obstructive pulmonary disease (COPD), obesity, and IHD in comparison to those without such conditions (Table 4).

Distribution of age of the participants (n = 77).
Classification of QoL according to WHOQOL-BERF in different domains (n = 77).

Domain-specific score averages of the study participants (n = 77).

Sociodemographic characteristics and mean of physical social, psychological, and environmental domains of QoL among stroke survivors in the study (n = 77).

p Value measured by one-way analysis of variance.
p Value measured by independent sample t-test.

Distribution of comorbidities among stroke survivors in the study (n = 77).
Comparison of individual domain score by chronic disease status (n = 77).
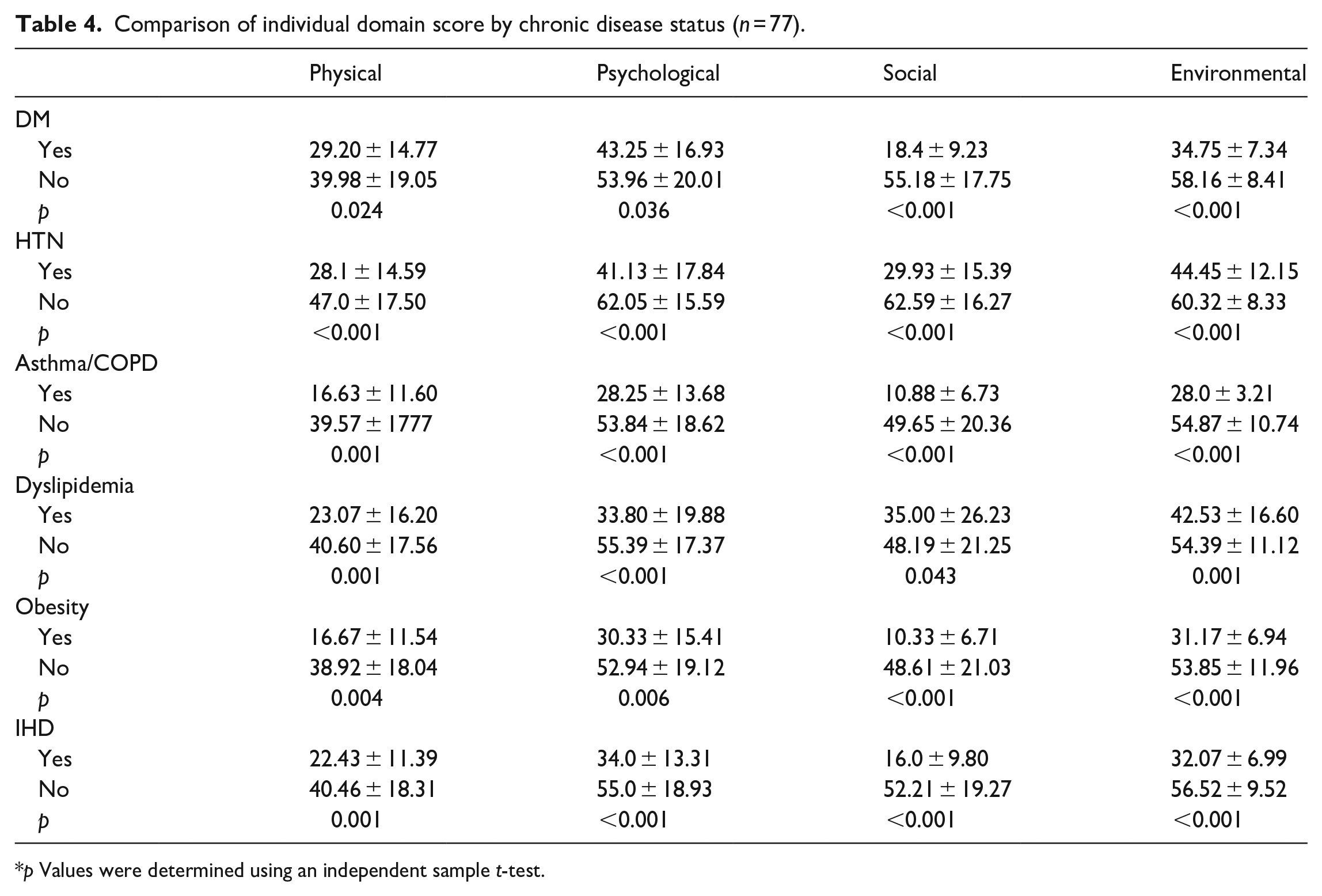
p Values were determined using an independent sample t-test.
Discussion
Stroke is a major chronic illness with morbid outcomes. For better rehabilitation, adequate assessment of the QoL among stroke survivors is instrumental. Despite a growing burden of post-stroke patients, Bangladesh has an insufficiency of research on the post-stroke QoL among them. Our study aimed to find the impact of stroke on domain-specific QoL and hoped to fill the existing gaps in policy. Following the WHOQOL-BERF scale, the overall perception of the participant’s QoL was just above neutral (Q1 3.14 ± 1.08). This trend was also reflected in the four domains of QoL explored in our study. The environmental domain had the highest average score, followed by psychological, social, and physical domains in decreasing order. Our study reveals an overall lower to moderate QoL in the physical, psychological, and social domains when compared to a study conducted in India, where significant improvements were observed in these areas. 15 Contrary to our study, a distinct study conducted in India found that the physical and psychological aspects of QoL were more profoundly affected than domains like social relationships and the environment. 16 Nonetheless, our study findings suggest that participants in our research experienced a comparatively lesser impact in the psychological and environmental domains in comparison to the physical and social domains. 17 The probable reason for this difference is that the majority of our patients were living with family members, relatives, and friends who provided sufficient care for their early recovery and restoration of daily activities. Consequently, emotional changes during stroke were effectively controlled and managed through continuous family support. A structured review study showed that programs that train families in supportive communication techniques have successfully improved patient symptom management and health behaviors. 18 We found that, for physical, psychological, social, and environmental domains, the mean QoL was higher in males than the females. A study conducted in India similarly noted that QoL was better in male stroke patients than in female stroke survivors. 17 The reason for such gender-related alterations in QoL is predictable due to mark dissimilarities in good musculoskeletal systems in males at any age. In our study, we observed that unmarried individuals exhibited lower QoL in the physical, psychological, and environmental domains compared to married patients. These findings align with a Nigerian study, which indicated significantly higher QoL in married participants during various post-stroke follow-ups, in contrast to those who were single, separated, or divorced. However, a Portuguese study shows that divorced survivors had higher average scores on physical, psychological, social, and general dimensions than married or widowed survivors. 19 A general increase in QoL scores in all domains was noted with a higher level of education in all four domains. This finding supports the work of Skevington, who assessed the association of QoL with education in 13 different countries among both sick and healthy people. 20 It was observed that individuals with higher levels of education typically have improved job opportunities and higher income, thereby positively influencing their QoL.20,21 Participants living in urban areas have good physical, social, and psychological domain scores but lower environmental scores than in rural areas which supports a European survey where rural areas have much lower QoL than urban areas. 21 However, high population density and pollution levels in the urban areas might also negatively affect the subjective QoL in these regions. 22
One of the important findings of our study was the significant association of chronic diseases with a substantially low QoL in all domains. We investigated how HTN, DM, heart disease, asthma/COPD, dyslipidemia, and obesity impact the QoL of the participants. Our study found that stroke patients with any of these chronic conditions experienced significantly lower scores in all domains of QoL. These findings are consistent with previous studies conducted on various disease processes.23,24,25
The limitations of our study stem from it’s cross-sectional design, which restricts the possibility of long-term follow-ups among the study participants. Furthermore, the data collection was confined to a single tertiary center, thus not capturing a comprehensive representation of the entire country. In addition, the use of consecutive sampling and purposive selection of the study site may introduce selection bias. Therefore, we recommend conducting a multicenter cohort study with a larger sample size for future research. It is important to note that WHOQOL assessments hold significance in cases where disease prognosis involves partial recovery or remission, and treatment focuses more on palliative care rather than curative measures. To enhance the QoL for stroke survivors, it is crucial to implement early rehabilitative measures such as physiotherapy, patient and family counseling, and the adoption of healthy lifestyle practices as early interventions.
Conclusions
This study revealed that stroke survivors experienced compromised QoL across various domains, including physical, psychological, social, and environmental aspects. Factors such as being female, having lower levels of education, residing in urban areas, and having chronic diseases were associated with lower QoL. To enhance the QoL for stroke patients, it is crucial to focus on prevention of disability, early detection, prompt treatment, and effective rehabilitation.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231208604 – Supplemental material for Quality of life of stroke survivors in Bangladesh
Supplemental material, sj-docx-1-smo-10.1177_20503121231208604 for Quality of life of stroke survivors in Bangladesh by Shimu Sarkar, Ayesha Rahman, Nashid Islam, Md Ali Emran and Jheelam Biswas in SAGE Open Medicine
Footnotes
Author contributions
Shimu Sarkar has been involved in conceptualization; Shimu Sarkar and Nashid Islam have been involved in data curation; Ayesha Rahman and Shimu Sarkar have been involved in formal analysis. Shimu Sarkar, Ayesha Rahman, and Md Ali Emran have been involved in the investigation; Ayesha Rahman, Jheelam Biwas, Nashid Islam, and Shimu Sarkar have been involved in methodology; Shimu Sarkar and Md Ali Emran have been involved in project administration; Shimu Sarkar and Ayesha Rahman have been involved in writing the original draft; Ayesha Rahman and Jheelam Biswas have been involved in writing review and editing.
Disclaimer
Assistance in writing was obtained from artificial intelligence software to enhance certain sections of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Internal Review Board of Bangabandhu Sheikh Mujib Medical University BSMMU/2021/7953; date: 01 September 2021.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from each participant who had the ability to make decisions and provide written informed consent, or from their legally authorized representative if they were unable to make decisions themselves.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.