
Abstract
Background:
Female sexual dysfunction (FSD) is a highly prevalent health problem but is often paid less attention, moreso in developing countries. There are many factors responsible for dysfunction such as disturbed sleep and mental health problems. However, it is largely understudied.
Aims and objective:
The aim of the present study was to observe the relationship between sleep and sexual functioning and to observe the relationship between mental health problems (depression and anxiety), sleep and sexual functioning.
Method:
A cross-sectional study was conducted in a tertiary health care center in India. Seventy adult female patients who were visiting Department of OBGY, OPD for any ailment, were sexually active and consenting for the study were included. The participants were evaluated on sleep, sexual activity, depression and anxiety by Pittsburgh Sleep Quality Index, Female sexual functioning index (FSFI), Beck’s depression inventory and Beck’s anxiety inventory, respectively.
Result:
The mean age of the sample was 33.5 (SD 6.2) years. Only 4% of the participants (n = 3) reported moderate to severe depression. Thirty percent of the participants (n = 21) reported mild anxiety symptoms. The median sleep latency of the participants was 42 (10,180) minutes. The mean subjective total sleep time was 356.6 (SD 60.3) minutes. 27.1% of the participants (n = 19) reported Global PSQI scores >5 suggesting sleep disturbance. Ten percent of the participants (n = 7) reported mild to moderate sexual dysfunction, 55.7% of the participants reported mild sexual dysfunction. A significant positive correlation was observed between hours of sleep and sexual satisfaction.
Conclusion:
A healthy sleep is necessary for good sexual functioning. The sexual functioning is also affected by mental health problems such as depression and anxiety in females.
Introduction
Female sexual dysfunction (FSD) is defined as a persistent or recurring decrease in sexual desire, persistent or recurring decrease in sexual arousal, dyspareunia and a difficulty in or inability to achieve an orgasm. 1 The report of the International Consensus Development Conference on FSD has classified it into four disorders: designated desire disorders (DD), arousal disorders (AD), orgasmic disorders (OD) and pain disorders (PD). Although FSD is a highly prevalent health problem affecting 25%-63% of women, information with regard to its prevalence is still scarce in international literature. 2
Sexuality is an important and complex domain. Sexual dysfunction is a taboo subject in many countries including India and it negatively affects quality of life. It is also often responsible for psychopathological disturbances. These problems are often not volunteered as they may affect reproduction and can cause marital conflict, familial discord, separation and divorce.
There are multiple etiologies for FSD. Various factors such as medical illness, psychiatric illness, and relationship conflicts have been identified previously have been identified previously.3-6
Sleep is an evolutionarily conserved process that occupies approximately one-third of a human’s and is important for rest and recovery of various biological functions. 7 Good quality sleep is essential for general health and well-being. Sleep is influenced by multiple factors and is considered a public health problem.8-11 It negatively affects immune system and increases risk of cancer, chronic diseases and mental health problems.10,12-18 Sleep quality has been observed to be worse in women than men which makes them susceptible to a worse quality of life. It has been observed that women consume various medications to improve the same.19-26
Though initially studied as early as the 1960s, the intersection of sleep and sexual functioning has not been paid much attention. The literature on sleep and female sexuality is limited to a modest number of studies on rapid eye movement (REM) sleep and nocturnal vaginal vasocongestion from the 1960s through the mid-1980s. 27 However, they have not been able to identify clear role of REM sleep in human sexual response. It has been observed that chronic REM sleep deprivation in laboratory animals leads to hypersexuality.28,29 More recently, the research has shifted to the roles of hormones in sexual function and sleep, and sleep-disordered breathing (e.g., obstructive sleep apnea) as a risk factor for sexual problems.30-32
In a recent review by Andersen and colleagues, it was reported that neuroendocrine reproductive control activity may mediate the influence of sleep on human sexual response. Sufficient levels of testosterone, progesterone, and estrogen have been identified as important for healthy sexual functioning in women. It is also reported that in females androgen levels are increased by sleep and vice versa. 33 Thus, sleep loss or deprivation can lead to impaired sexual function which might be mediated by deficient androgen levels. Considering the complexity and role of various factors in sleep and sexual dysfunction, there is a dire need to understand their relationship. India, despite being a country where “Kamasutra” (by Vatsyayana) took birth, is lacking much in sexuality-related literature. There are very few studies on sexual dysfunction in females from India and to our knowledge, none on the relationship between sleep and sexuality in Indian females. So, the primary aim of our study was to observe the relationship between sleep and sexual functioning. The second aim of our study was to observe the relationship between mental health problems (depression and anxiety), sleep and sexual functioning.
Methodology
The study was a cross-sectional observational study and was conducted in a tertiary health care center in India. The primary aim of the study was to assess the prevalence of sexual dysfunction and sleep problems in adult females and to observe the correlation between sleep problems and sexual dysfunction. The secondary aim of the study was to assess prevalence of depression and anxiety in our participants and its correlation with sexual and sleep problems. We included 70 adult female patients who were visiting the Department of OBGY, OPD for any ailment and were sexually active. Patients who did not give consent, suffering from any other psychiatric illness or having any serious/debilitating illness hampering interview were excluded from the study.
Data Collecting Tools
Statistical Analysis
Data were analysed using SPSS software. The continuous variables were expressed as mean and standard deviation. The correlation between different variables was calculated by Pearson’s correlation. Statistical significance was denoted at the 0.05 level.
Results
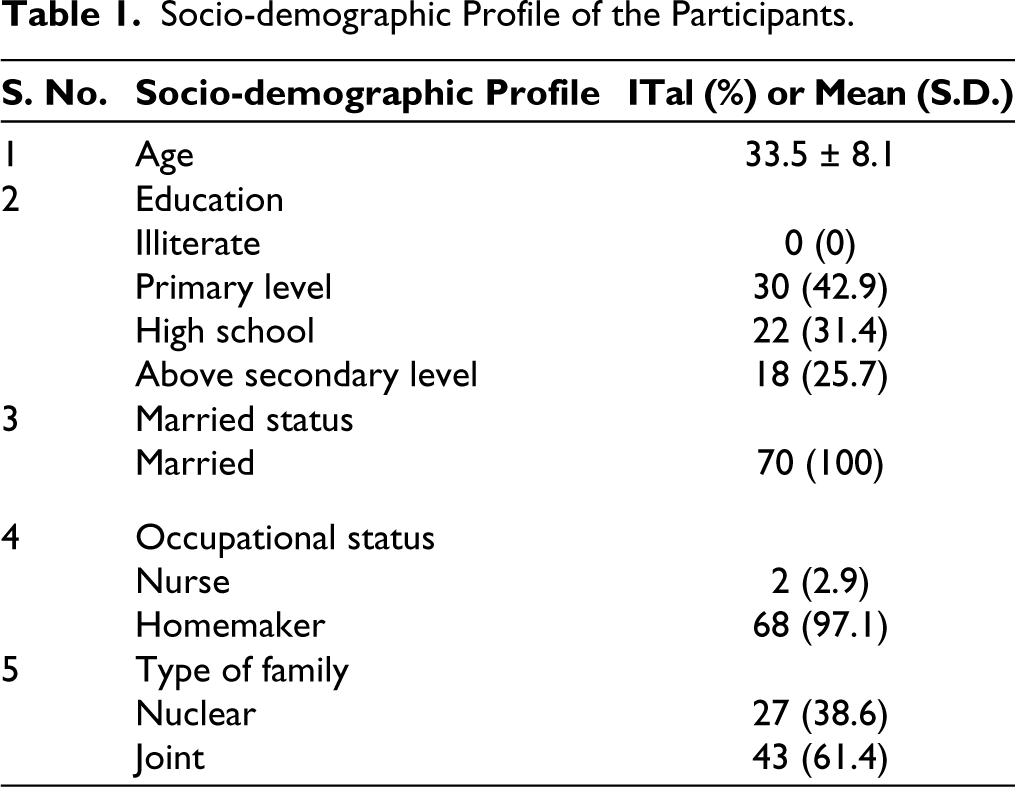
The mean age of 70 participants was 33.5 (SD 6.2) years. All the participants were married. Most of them were homemakers and two of them were working as nursing staff. All of them have received basic education and few were college graduates. The detailed socio-demographic profile is given in (Table 1).
Socio-demographic Profile of the Participants.
Sleep Profile
The median Global PSQI score was 4 (0,17). The median sleep latency of the participants was 42 (10,180) minutes. The mean subjective total sleep time was 356.6 (SD 60.3) minutes. The median Beck’s Depression and Anxiety score was 7 (0,22) and 5 (0,15) respectively. 27.1% of the participants (n = 19) reported Global PSQI scores >5 suggesting sleep disturbance.
Female Sexual Functioning Index
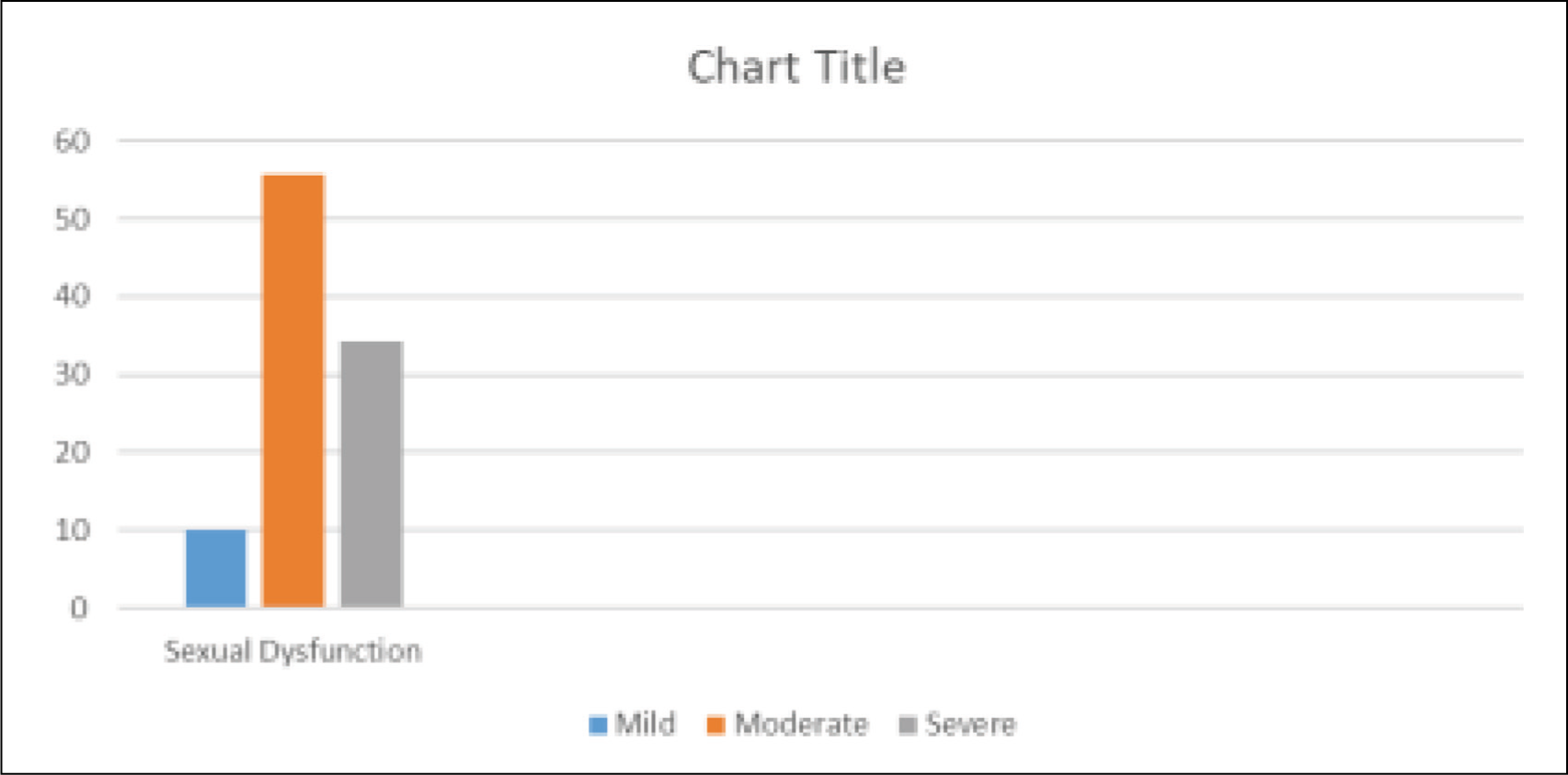
The mean FSFI score was 26 (SD 3.3). The mean score for desire, arousal, lubrication, satisfaction and pain were 2.9 (SD 1.0), 3.5 (SD 0.8), 4.7 (SD 0.7), 3.3 (SD 0.5), 6 (SD 0.7) and 5.3 (SD 1.1), respectively. Ten percent of the participants (n = 7) reported mild to moderate sexual dysfunction, 55.7% of the participants reported mild sexual dysfunction while 34.3% of the participants reported no sexual dysfunction (Figure 1).
Percentage of Mild, Moderate and Severe Sexual Dysfunction.
Depression and Anxiety
24.3% of the participants (n = 7) reported mild to moderate depression. Around 4% of the participants (n = 3) reported moderate to severe depression. Thirty percent of the participants (n = 21) reported mild anxiety symptoms.
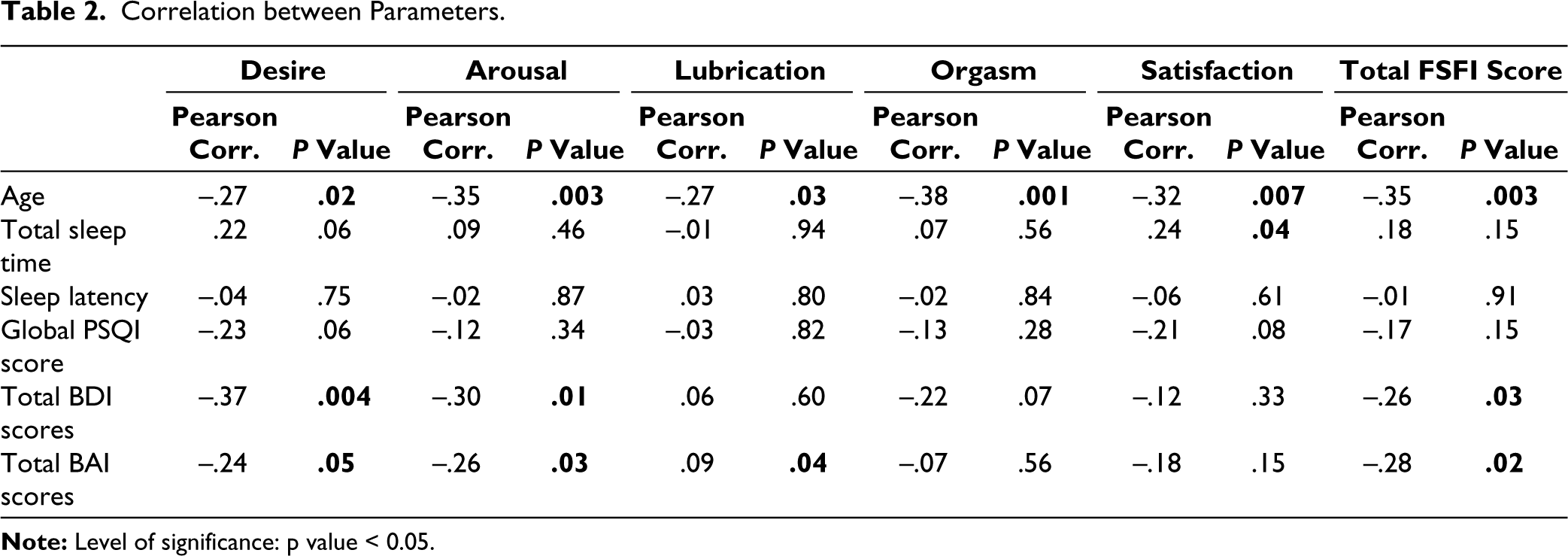
Table 2 shows a correlation between the age of the participants, sleep variables, depression and anxiety with scores on sexual functioning. A significant negative correlation was observed between age and different stages of sexual cycle and total FSFI score. A significant positive correlation was observed between hours of sleep and sexual satisfaction. A significant negative correlation was observed between total BDI scores and scores on desire, arousal and total FSFI scores. Similarly, a significant negative correlation was observed between total BAI scores and scores on desire, arousal, lubrication and total FSFI scores. It was observed that sleep latency has a significant positive correlation with total BDI scores (r = 0.49, P < .001) and total BAI scores (r = 0.40, P = .001) and hours of sleep had a significant negative correlation with total BDI scores (r = −0.31, P = .009) and total BAI scores (r = −0.32, P = .007). Global PSQI scores had a significant positive correlation with total BDI scores (r = 0.49, P < .001) and total BAI scores (r = 0.43, P < .001).
Correlation between Parameters.
Discussion
Human sexuality is an amalgamation of an individual’s biological constitution, life experiences, knowledge and behavior and can be influenced by various physical, psychological, interpersonal, and cultural factors. In India, discussing about sex, although is still considered taboo but now has gained some attention as there have been some changes in the attitude of people toward sexuality. The expressions and feelings of sexuality are now accepted as natural. The roles of females in India are gradually evolving. However, still, in most parts of the country, Indian females lack independent authority for control of their sexuality or reproduction. 40 Our study is an attempt to bring attention to sexual problems of Indian females and the factors affecting them. The relationships between mental health and sleep, and mental health and sexual function are well-established.41-43 The findings of our study replicate the same. Sleep and sexual functioning share a complex interplay of multiple factors and seem to have evidence of a bi-directional relationship. As both the parameters, sleep and sexual activity have a frequently shared context (bed), distress in one aspect often triggers problems in other aspects. Similar to our study, Seehuus et al., observed a link between sleep and sexual dysfunction that was beyond the shared influence of other mental health factors (Seehuus et al., 2018). 44 Our study supports the fact that with advancing age there is reduction in sexual functioning of females due to various hormonal and physical factors such as dryness of the vagina. Similar findings were reported by other Asian studies.45,46 The report on the Global Burden of Disease estimates the point prevalence of unipolar depressive episodes to be 3.2% for women, and the 1-year prevalence to be 9.5% for women. 47 The population-based study from India on depression shows the prevalence of depression to be 15.1%. 48 The rate of various anxiety disorders is also quite high in Indian females. 49 Sexual dysfunction can both be a cause and effect in patients with depression. Previous literature has shown that FSD is found more commonly in depressed females than in females with no depression. 50 A Study conducted in the United States on Women’s Health Across the Nation (SWAN) also showed recurrent depression to be associated with reduced arousal and pleasure. 51 Both of these disorders have a negative influence on sleep and sexuality. Yet, depressed female patients are very reluctant to talk about sexual dysfunction even when they are in the hospital for the treatment of depression. Our study observed that good sleep promotes sexual satisfaction. The importance of sleep is often overlooked in the modern society. In most Indian families, the sleep of the females is usually less than the male counterparts which has an effect on all the domains of the sexual cycle. This study has some important limitations. First, this study is cross-sectional in nature and is thus unable to describe any causal linkages or pathways. Although these findings support that a correlation exists between measures of sleep disturbance and sexual dysfunction, it cannot speak directly to the mechanism of that connection it has. In addition, the sleep parameters in the study were subjective sleep reports rather than objective. In a sexual relationship, a couple is a unit as there are many factors which play a role, however, we had included only females and not their male counterparts. These findings are best understood as a description of the experience of sexuality and the experience of sleep, as opposed to direct, objective measurements of either. These new findings support a meaningful relationship between depression, anxiety, stress, sleep and sexual function. They further suggest that the relationship between sleep and sex goes beyond the shared mental health correlates, although the nature of that relationship is as of yet uncertain. Future research should explicitly test the possibility of shared psychopathological roots, a shared learned context, or some other mechanism of association. Identifying this mechanism may allow for the development of treatments that can better address these important clinical issues, which so commonly co-occur.
Footnotes
Data Availability
Data can be made available upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
The study was approved by institutional ethics committee of All India Institute of Medical Sciences, Gorakhpur and informed consent was taken from each participant before commencement of the study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.