
Abstract
Background:
Sexual dysfunction in female with depressive disorder is highly prevalent and strikingly understudied. Epidemiological and clinical studies have shown association between depression and impairments of sexual function. Despite high prevalence, there are limited studies regarding the prevalence of sexual dysfunction among female with depressive disorder in Nepal.
Aims:
This study was conducted to find out the prevalence of sexual dysfunction in female with depressive disorder in Nepal, their association with treatment status, and the level of psychological distress caused by it.
Methods:
A descriptive cross-sectional study was carried out among female with depression at Tribhuvan University Teaching Hospital, Nepal. The participants were grouped as drug naïve and under medication. Data were collected using semi-structured proforma, Beck Depression Inventory, Kessler 6+ Psychological Distress Scale, and Female Sexual Function Index. Data were tabulated and analyzed using Statistical Package for Social Sciences version 23.
Results:
The prevalence of sexual dysfunction was 58.82%, being 60.78% in drug-naïve cases and 56.86% in females suffering from depression and receiving medications. This study showed statistically significant association between sexual dysfunction and psychological distress but not with age, duration of marriage, number of children, occupational, and financial status.
Conclusions:
The study reported high prevalence of sexual dysfunction among female with depression. All domains of sexual function were affected and showed significant association with psychological distress. Therefore, assessment of sexual dysfunction in every female with depression is required to address the problem timely and efficiently.
Introduction
Sexual disorders are extremely common, but still underrecognized in clinical practice and often underdiagnosed. The most frequently reported sexual dysfunctions in female are lack of sexual desire, decreased arousal, decreased lubrication, and delayed orgasm.1–3
Depression leads to emotional and physical problems which impact biological functions such as sleep, appetite, and libido. Anhedonia in depression can also predictably affect libido. Likewise, loss of libido itself can be the presenting complaint of depression and loss of libido may precede depression. 2
Study suggests existence of complex and bidirectional relationship between sexual dysfunction and depression. 4 Sexual dysfunction and depression are highly comorbid which is estimated to be around 70% to 80% in various studies. Comparative studies reveal higher sexual dysfunction in individuals with depression than in general population and depression severely affects all phases of sexual functioning. 5
The reported incidence of sexual dysfunction depends on several factors such as the enquiry method, people’s perceptions of their sexual satisfaction, their willingness to discuss problems, awareness of sexual concerns, and medical care access. 6
Though the prevalence of sexual dysfunction is high among female with depressive disorder, there are limited studies. Also, the studies show marked differences in prevalence by self-reporting and active questioning. Antidepressant medications can also induce sexual dysfunction as adverse effect. 7 This study aims to find out the burden of sexual dysfunction which is significantly underreported by women and overlooked by clinician in women with depressive disorder in Nepal.
Methods
Women visiting outpatient department of department of psychiatry and mental health who were diagnosed to be suffering from depression according to ICD-10 were assessed for 1 year from December 2019 to November 2020. All female patients attending the psychiatry outpatient department, fulfilling inclusion criteria, and willing to participate were included and women with medical comorbidities, psychoactive substance use, and not willing to participate were excluded. Ethical clearance was obtained from the Institutional Review Committee. Total 102 individuals participated in the study, among them 51 were receiving treatment and the remaining were drug naïve. Informed consent was obtained from each participant. The semi-structured pro forma was filled with adequate information including age, marital status, education, religion, occupation, occupation of husband, type of family, age at marriage, duration of marriage, number of living children, age at first child birth, age at last child birth, history of psychoactive substance use in husband, past history, family history of psychiatric disorders, history of substance use, and use of medication following rating scales were used.
The Beck Depression Inventory
It is a 21-item, self-report rating inventory that measures characteristic attitudes and symptoms of depression. 8 It has sensitivity (87%) and specificity (79%). It was translated to Nepali language, and validation of the tool was studied in 2002. 9 Individuals rating themselves on scores of 0 to 9 indicate minimal depression, 10 to 18 indicate mild depression, 19 to 29 indicate moderate depression, and 30 to 63 indicate severe depression. 10
Female Sexual Function Index (FSFI-19)
FSFI is a brief, multidimensional, self-reported instrument, used to assess the key domains of sexual function in females. It assesses 6 domains of sexual function: desire, physical arousal-sensation, physical arousal-lubrication, orgasm, satisfaction, and pain. It consists of 19 questions with a score of each domain ranging from 0 to 5 of total scores 2 to 36. Scoring is done by summation of each domain score. The sum of each domain score is first multiplied by a domain factor ratio (0.6 for desire, 0.3 for arousal, 0.3 for lubrication, 0.4 for orgasm, 0.4 for satisfaction, and 0.4 for pain) in order to place all domain totals on a more comparable scale, and then subsequently summed to derive a total FSFI score. 11
Sensitivity and specificity of the test were 0.93 and 0.94, respectively. Score 26.55 was taken as cutoff for sexual dysfunction. 12 The individual domain scores and total score of the FSFI were recorded. FSFI was translated into Nepali using the guideline. 13
Kessler-6+
The K-6+ is standardized and validated screening tool for nonspecific psychological distress experienced over the preceding 30 days. It uses 5-point Likert scale. There are 2 types of scoring, one is the Australian method of 1 to 5 as a score and another is 0 to 4 which we are using. The responses range from “none of the time” coded 0 to “all of the time” coded 4. The 6 items are summed to yield a total score between 0 and 24 with cutoff point of 5 ≤ K6 < 13, which indicates score 5 to <13 as moderate mental distress and >13 as severe mental distress.14, 16
The scale has demonstrated excellent internal consistency and reliability (Cronbach’s alpha = 0.89) (Kessler et al., 2002).14, 15
The scale is available in a Nepali version and has been used previously in Nepal as well as in a variety of cultural settings in different parts of the world.16, 17
Data analysis was performed using SPSS v 23.0 statistical software package. Analyses included standard descriptive statistics. Results of descriptive analysis were expressed using mean ± standard deviation, percentage with 95% confidence interval (CI) whenever appropriate. The χ2 test was used to observe association between categorical independent variables and categorical dependent variables and value of P < .05 was considered statistically significant. Strength of association was further determined by binary logistic regression and expressed in terms of P value with 95% CI.
Results
Total 102 participants were included in this study, among them 52 were drug naïve and remaining 52 were taking antidepressants. The mean age of the participants was 35.37 ± 10.34 (standard deviation [SD]) and 74.51% of the participants were in the age group of 26 to 50 years. The mean age at marriage of the participants was 21.2 ± 3.66 years. The sexual dysfunction was highest in age group 51 to 75 years (87.5%). A total of 47.1% of the participants had 2 children. The mean age at first child birth was 22.36 ± 3.41 (SD) years and last child birth was 26.76 ± 3.64 (SD) years.
A total of 50% participants had completed higher secondary educational level and sexual dysfunction was highest among illiterate group. Prevalence of sexual dysfunction increased with increasing severity of depression and it was 76.19% in individuals with severe depression.
Participants with sexual dysfunction showed severe mental distress (86.67%), which shows positive association between sexual dysfunction and level of psychological mental distress.
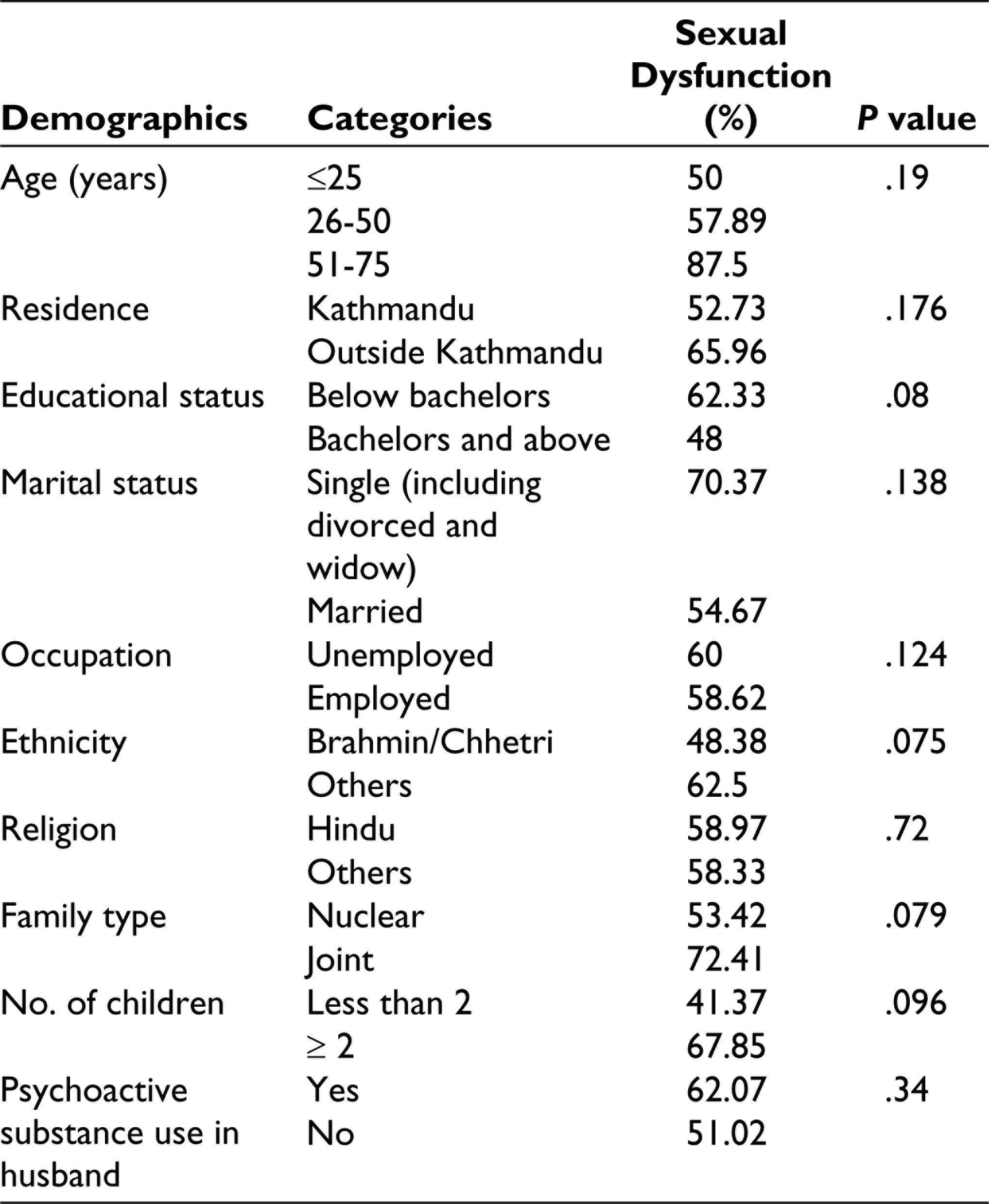
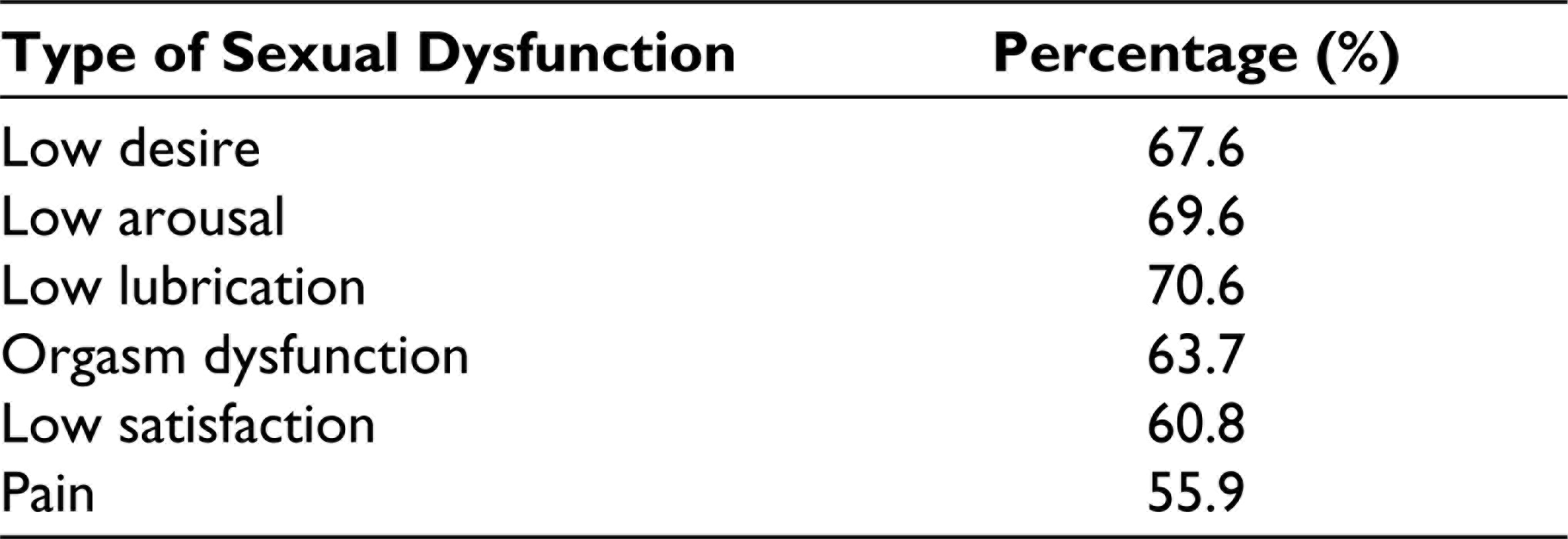
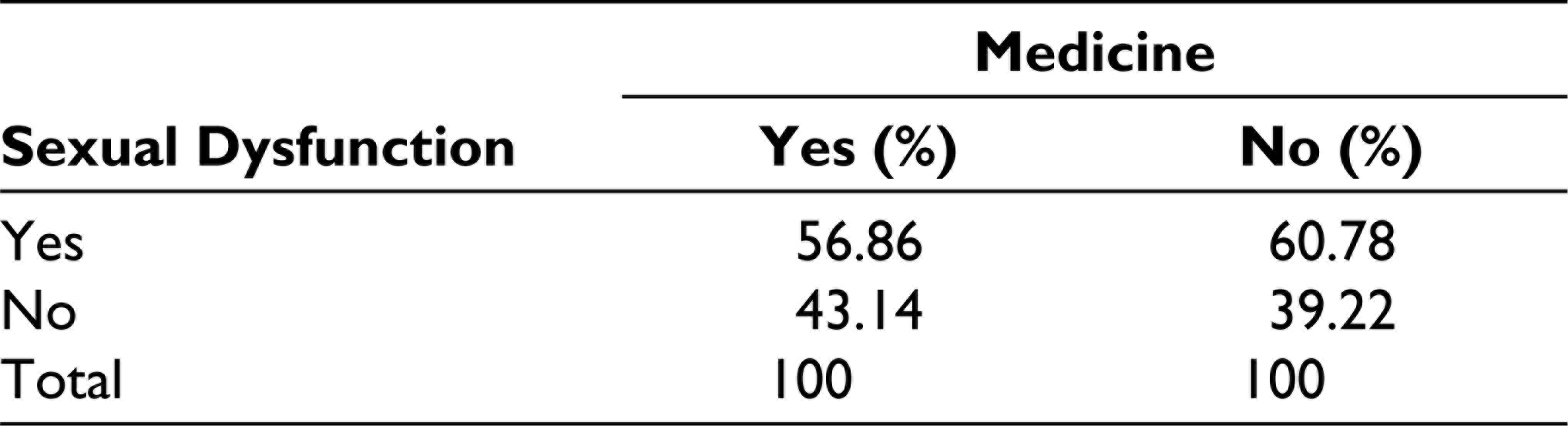
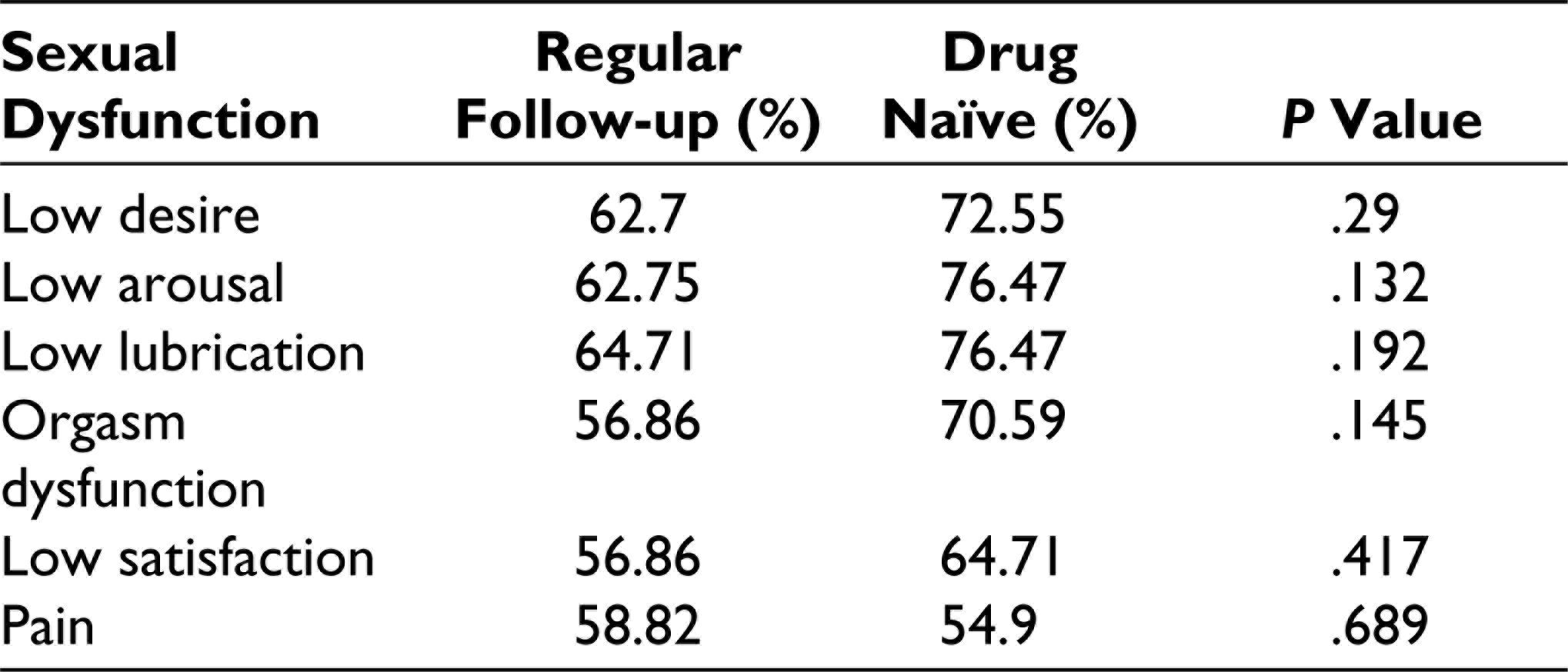
This study finds prevalence of sexual dysfunction to be 58.82%. The prevalence of sexual dysfunction and patient’s demographic profiles is shown in Table 1. As shown in Table 2, low lubrication, low arousal, and low desire were the common patterns of sexual dysfunctions noted in this study. Table 3 shows the association of sexual dysfunction and use of antidepressants in our study. The prevalence of sexual dysfunction was high in drug-naïve cases as compared to cases taking regular antidepressants. Table 4 shows the types of sexual dysfunction in both groups. Table 5 shows high proportional increase in prevalence of sexual dysfunction with severity of depression. Table 6 shows the association between sexual dysfunction and level of psychological distress, which shows increasing level of psychological distress in individual with sexual dysfunction.
Demographic Profiles and Prevalence of Sexual Dysfunction Among Female With Depression
Distribution on the Basis of Types of Sexual Dysfunction
Prevalence of Sexual Dysfunction in Drug-Naïve and Regular Follow-up Cases
Comparison of Patterns of Sexual Dysfunction in Drug-Naïve and Those Taking Antidepressants
Association Between Severity of Depression and Sexual Dysfunction

Association Between Sexual Dysfunction and Level of Psychological Distress

Discussion
This study was conducted with the objective to determine the prevalence of sexual dysfunction in female suffering from depressive disorder and to identify various factors affecting the prevalence of sexual dysfunction in females.
A major finding of this study was that the prevalence of sexual dysfunction in females suffering from depressive episode was 58.82%. Rates of sexual dysfunction in hospital-based studies from other developing countries, especially those which used the FSFI scale, reported prevalence for female sexual dysfunction ranging from 43% to 69%. Such differences in prevalence might be due to variation in age; social, economic, cultural, and environmental factors; and to various cutoff points for the definition of sexual disorders. 17
In this study, patterns of sexual dysfunction seen were low lubrication in 70.6%, low arousal in 69.6%, low desire in 67.6%, orgasm dysfunction in 63.7%, low satisfaction in 60.8%, and pain in 55.9%. Although the prevalence of other sexual domains dysfunction were high, low satisfaction and pain were less common, perhaps because of low expectations in a culture where women do not enjoy high levels of sexual satisfaction. In a study by Abhivant and Sawant 4 in India, 53% had low lubrication, 51% had orgasmic dysfunction, 49% had pain, and 45% had low desire, arousal, and sexual satisfaction which was less than the types of sexual dysfunction in our study.
In this study, prevalence of sexual dysfunction is 60.78% in females suffering from depressive disorder and not receiving treatment and 56.86% in females suffering from depression and receiving the treatment which was similar to a study which had observed a higher prevalence rate of 86% among depressed patients not receiving antidepressant treatment vs 73% in those taking these medications. 19 In a study by Angst, 19 prevalence of sexual dysfunction was 45% in female suffering from depression but not receiving treatment and 63% in patients suffering from depression who were taking antidepressants which was contradictory to our findings of more prevalence of sexual dysfunction in drug-naïve group than in participants taking antidepressants. 21
In another study by Sathyanarayana Rao et al, 21 prevalence of sexual dysfunction in drug-naïve female suffering from depression was 70.3%, which was slightly higher than the finding in our study. In another study by Abhivant and Sawant, 4 the prevalence of sexual dysfunction among drug-naïve female with depression was 67.34%, which was slightly higher than our finding. As drug-naïve and medication-receiving group were different groups, it could not comment whether the sexual dysfunction in the medicine-receiving group was due to depression or side effects of medication as there was no assessment of sexual dysfunction prior the beginning of antidepressants. So, it would be wise to administer FSFI to assess sexual functioning in every female presenting with depression before the start of antidepressant so that the physician can compare the sexual functioning before and after the treatment and could intervene the antidepressant-induced sexual dysfunction on time.
It should be noted that the sexual disorders found in this study were based on the FSFI questionnaire, but their clinical diagnosis value is limited. 22 It is ideal for women to receive appropriate training and counseling about sex and marriage, and this training should be conveyed in detail. Because of cultural barriers, these kinds of services are not available at present. In contrast with modern societies in which women have more sexual freedom and choice, sexual dysfunctions will likely remain prevalent in our part of world.
Sexual Dysfunction and Severity of Depression
Sexual dysfunction may be the presenting complaint of depression or it may precede depression. Studies from India showed highly significant association between sexual dysfunction and depression. 4 In this study, 53.3% participants had minimal depression (n = 36), followed by 29.4% moderate depression (n = 30), 20.6% severe depression (n = 21), and 14.7% mild depression (n = 15). Sexual dysfunction was more in participants with severe depression (76.19%), followed by mild depression (66.67%), moderate depression (63.33%), and minimal depression (41.67%) suggesting higher prevalence of sexual dysfunction in participants suffering from severe depression which was compatible to other studies.4, 8, 23 However, it shows no statistically significant association between the 2 in this study, while those abovementioned studies had shown the significant association between sexual dysfunction and depression. A review study suggests, existence of complex and bidirectional relationship between sexual dysfunction and depression, and the causal link remain uncertain. 24
Sexual Dysfunction and Psychological Distress
Sexual dysfunction in females is also associated with poor quality of life. The National Health and Social Life Survey in the United States found strong association between low sexual desire, arousal, and pain with decreased physical satisfaction, emotional satisfaction, and overall life satisfaction. 25
In this study, we found majority of the participants with sexual dysfunction had severe mental distress (86.67%), followed by moderate mental distress (77.78%) and no significant distress (37.25%). It also shows the statistically significant association between sexual dysfunction and psychological distress with P value .00. We could not find any previous studies which had studied the relationship between sexual dysfunction and psychological dysfunction in female with depression.
Limitation
As sampling was purposive, actual gravity of situation may differ from current finding. Finding may differ in larger population and the association of various sociodemographic profile may vary. In this study, no age limit was considered, extremes of ages may alter the prevalence of sexual dysfunction in women.
One of the major drawbacks of FSFI is that 15 of its items contain a zero option in the response set to indicate either “no sexual activity” (12 items) or “did not attempt intercourse” (3 items) within the past 4 weeks. However, absence of sexual activity is not necessarily attributable to sexual dysfunction.
Conclusion
The study finds prevalence of sexual dysfunction to be 58.82%, being 60.78% in females suffering from depressive disorder and drug naive and 56.86% in females suffering from depression and receiving antidepressants. The finding was consistent with global finding of high prevalence of sexual dysfunction in females suffering from depressive disorder.4, 18 The study had shown high prevalence of sexual dysfunction in female with higher severity of depression. It also showed higher level of psychological distress in female who suffers from sexual dysfunction.
In this study, female with depressive disorder with advancing age, lower education, and low family income had higher prevalence of sexual dysfunction, however it was statistically not significant. Also, this study had shown no statistical significance of female sexual dysfunction with age at marriage, duration of marriage, number of children, religion, ethnicity, occupation, occupation of husband, husband’s company, and psychoactive substance use in husband. However, this study showed statistically significant association between severity of depression and psychological distress.
Therefore, it would be wise to assess sexual dysfunction in every female presenting with depressive episode before and during medication to address the problem timely and effectively which will in-terms help with antidepressants compliance and decrease the psychological mental distress.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.