
Abstract
Background:
Sexual dysfunction (SD) among male psychiatric patients is common and may be the result of various bio- psycho-social factors. This study aimed to assess the proportion of men with depression and/or anxiety disorders having SD and evaluate its association with sociodemographic and clinical variables.
Methods:
This cross-sectional study conducted from November 2018 to June 2020 included 100 men attending the psychiatry outpatient department of a tertiary care hospital. Sociodemographic and clinical variables, including diagnosis based on International Classification of Diseases 10th Revision criteria, were assessed. Sexual functioning was measured by the Change in Sexual Functioning Questionnaire-Male Version (CSFQ-M).
Results:
In the study, sexual pleasure dysfunction, sexual desire dysfunction, sexual desire/interest dysfunction, sexual arousal/erection dysfunction, and sexual orgasmic dysfunction were 71%, 71%, 66%, 68%, and 73%, respectively. Pearson correlation between Hamilton Depression Rating Scale score and sexual desire/interest component of CSFQ-M was r = 0.209 (P = .008). Correlation between Hamilton Anxiety Rating Scale score and sexual desire/frequency component was r = 0.095 (P = .012), sexual desire/interest component yielded r = 0.114 (P = .029) and sexual arousal/erection component yielded r = 0.134 (P = .052).
Conclusions:
Certain areas of sexual functioning are impacted by depression and/or anxiety disorders symptoms. The hypothesis that those with depression and/or anxiety would have lesser overall sexual functioning is supported in some areas by the results. Clinicians should be vigilant of this association and should plan treatment to enhance compliance and outcome.
Introduction
According to World Health Organization, mental health is “a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community.” 1 In some studies, Indian population is compared with Western population in respect to depression and it was found that somatic symptoms like insomnia, anxiety, suicidal ideations, and genital symptoms are more common in Indian subjects whereas depersonalization, paranoid, and obsession symptoms are less frequent. 2 Depression is characterized by loss of interest, reduction in energy, lowered self-esteem, inability to experience pleasure, irritability, and social withdrawal which may impair the ability to form and maintain intimate relationships. It is very rare that these symptoms don’t create any problem in sexual relationships. 3 Sexual dysfunction (SD) and depression are very common conditions that are age-related and mostly chronic. 4 In world, around 43% of women and 31% of men are affected by SD. 5 As with erectile dysfunction (ED), the incidence of depression increases with age. Several studies have shown that there is a strong relationship between ED and psychological conditions such as stress, anxiety, depression, and dissatisfaction. 6 Loss of sexual desire may be more common than disorder of arousal and orgasm, but specificity of SD varies in incidence. Disorders of sexual function are common among men of all ages, ethnicities, and cultural backgrounds. 7 Desire, libido, pleasure, sexual life, intercourse, erection, ejaculation, orgasm, and happiness are the several aspects of complex male sexuality. 8 Similarly, anxiety is the common pathway by which social, psychological, biological, and moral factors converge to impair the sexual response. The neurobiological expression of anxiety is complicated, but it mainly involves release of adrenergic substances epinephrine and norepinephrine. 9 Anxiety disorders predispose suffering individuals to SD. 10 Sexual problems among men were associated with anxiety and medical problems, whereas for women SD is mostly associated with marital difficulties. In particular, higher rates of SD have been found in individuals suffering from phobia, panic disorder, generalized anxiety disorder (GAD), and obsessive-compulsive disorder (OCD) than in general population. Sexual avoidance may also be caused by ED in males affected with panic disorder. 11
The most common mental disorder in India and across the world which affects almost all the age groups, socioeconomic status, and genders is depression. Major depressive disorder (MDD) was the third leading cause of disability during 2015, and this graph is persistently increasing. 12 The global prevalence of depressive disorder ranges from 3.2% to 4.7%.4, 13 Globally, pooled period prevalence of mood disorder is 5.4% and as per the World Mental Health Survey it ranges from 0.8% to 9.6% across all the countries. 14 Among the psychiatric disorders, anxiety disorders (GSD, panic disorder/agoraphobia, social anxiety disorder, and others) are most prevalent and are associated with a high burden of illness. 15 Generally, in primary care setting they are under recognized and under treated.16–18 Among anxiety disorders, specific phobias are the most prevalent with a percentage of 10.3%, panic disorder have a prevalence of 6% followed by social anxiety disorder at 2.7% and generalized anxiety 2.2%. Women are 1.5 to 2 times more prone to anxiety disorder.19–22 Sexual functioning is a complex process including bio-psycho-social process, along with coordination of the neurological, vascular, and endocrine systems. In addition to the biological factors, the psychosocial factors like societal and religious beliefs, health status, personal experience, ethnicity, sociodemographic conditions, and psychological status of the person/couple play an important role in adequate sexual functioning of a person. If any disturbance occurs in these areas, it can progress to SD. These SDs are either lifelong or acquired and situational or general. “In ICD-10 sexual disorders are placed under the headings of Sexual dysfunction, not caused by organic disorder or diseases (F52) under the broad heading of Behavioral syndromes associated with physiological disturbances and physical disorders.” Sexual dysfunction is most commonly associated with depression, which occurs in about 45 million population in India alone as given by National Mental Health Survey of India in the year 2015. Men experience SDs under the headings of premature ejaculation (21%), ED (5%), and decreased libido (5%). Amongst these categories, decreased sexual desire is most commonly associated with depression, but ED is experienced in up to 25% of depressed male patients.23, 24 Increase in severity of depressive symptoms can cause an impact on a person’s arousability and sexuality and can lead to ED. 25 Besides this, decreased engagement in sexual activity as well as unsatisfactory sexual life can precipitate depression.4, 26 To evaluate SDs in depressed men, Clayton et al 27 incorporated Changes in Sexual Functioning Questionnaire (CSFQ) under the aspects of libido, frequency of sexual desire, sexual pleasure/orgasm, and sexual arousability and found that all were negatively affected by depression. 27 Kendurkar and Kaur 28 used the Psychiatric Diagnostic Screening Questionnaire to include patients with MDD, OCD, GAD, and a healthy group population as control group. They found that the rate of SD was 30% in healthy controls, 76% in MDD subjects, 50% in OCD subjects, and 64% in GAD subjects. Most commonly reported dysfunction among all the categories was low sexual desire. SD was seen more in patients with MDD than with those having OCD and GAD. 28 Thakurta et al 29 included a series of 24 male and 36 female patients with MDD and found that over 33.33% of men and 42% of women reported decreased sexual interest. The ejaculatory or orgasmic difficulties (11–16%) were comparatively less common to reduced levels of arousal (8–22%) and also concluded that women are more affected with SD as compared to men. 29 Turan et al 30 enrolled 78 OCD patients who were sexually active and aged between 18 and 52 years. Prevalence of SD was seen in 65.4% of OCD patients and 28.3% of the control group. Females with OCD (51.2%) presented with major complaint of anorgasmia, whereas hypoactive sexual desire was mostly reported by males with OCD (18.2%). Female OCD patients had higher Arizona Sexual Experiences Scale (ASEX) scores of sexual desire, excitement, vaginal lubrication, orgasm, and orgasmic satisfaction as compared to healthy subjects. 30 Karmakar and Sarkar 31 did a comparative study in which they included 117 sexually active adult drug naïve patients (74 male and 43 female) who were diagnosed with severe depressive episode without psychotic symptoms (as per ICD-10). Their sexual functioning was screened with current CSFQ. They found that 71.6% males and 90.7% females were having SD. Most of the women had orgasmic dysfunction and most of the men had decreased libido and desire. In the end, they concluded that SD highly correlated with depression in both men and women and should be treated appropriately. 31
However, little is known about the role of SD in the life of depressed/anxiety patients. Thus, we conducted this study to explore various psychosexual disorders amongst the male patients diagnosed with depressive and/or anxiety disorders attending psychiatry OPD.
Materials and Methods
After obtaining approval from the Ethics Committee of Netaji Subhash Chandra Bose Subharti Medical College, Swami Vivekanand Subharti University, Meerut and the subjects who gave written informed consent were selected from the outpatient department of psychiatry in Chhatrapati Shivaji Subharti Hospital and Netaji Subhash Chandra Bose Subharti Medical College, Meerut. The study was a cross-sectional observational study for which purposive sampling was done. The study was conducted from November 2018 to June 2020. All male patients suffering from depressive and/or anxiety disorders diagnosed in accordance with ICD-10 diagnostic criteria were selected for study. Additionally, subjects who have been sexually intimate at least once in past 1 year were included in the study. A semi-structured pro forma was filled for each subject, which included sociodemographic details, sexual history, current sexual functioning, and relationship with partner, physical examination, and mental status examination. The cases were assessed for the severity of anxiety and/or depressive disorders symptoms with Hamilton Anxiety Rating Scale (HAM-A) and Hamilton Depression Rating Scale (HAM-D), respectively. Psychosexual dysfunction was assessed with CSFQ for males (CSFQ-M-C). CSFQ was developed by Clayton, McGarvey, Calvet, and Piazza in 1997. The questionnaire is designed for both males and females and lists 14 items. Our study utilized only the part of questionnaire intended for male participants (CSFQ-M-C). It is used to rate severity of their SD by probing sexual desire/frequency score, sexual desire/interest, sexual pleasure, sexual arousal/erection, and sexual orgasm/ejaculation. The scoring of the scale is based on all 14 items.
Patients on any antipsychotic medications for more than 6 months, with major psychotic disorder (eg, schizophrenia), with organic disease (eg, genitourinary disease, trauma to genital area, diabetes mellitus, and hypertension), neurological disorder, suffering from learning disability and/or major language impairment, and with history and/or current use of any psychotropic substance were excluded from the study.
The data so obtained was appropriately compiled and tabulated and thereafter analyzed with chi-square test, Pearson correlation, and its significance was checked with P value at .05.
Results
Table 1 shows that most of the male patients (90%) were Hindu and the remaining (10%) were Muslims, majority of subjects belonged to rural areas (55%), joint family (60%), married (86%), and more than two-third (70%) of the patients belonged to upper-middle class according to the modified Kuppuswamy classification.
Sociodemographic Variables.
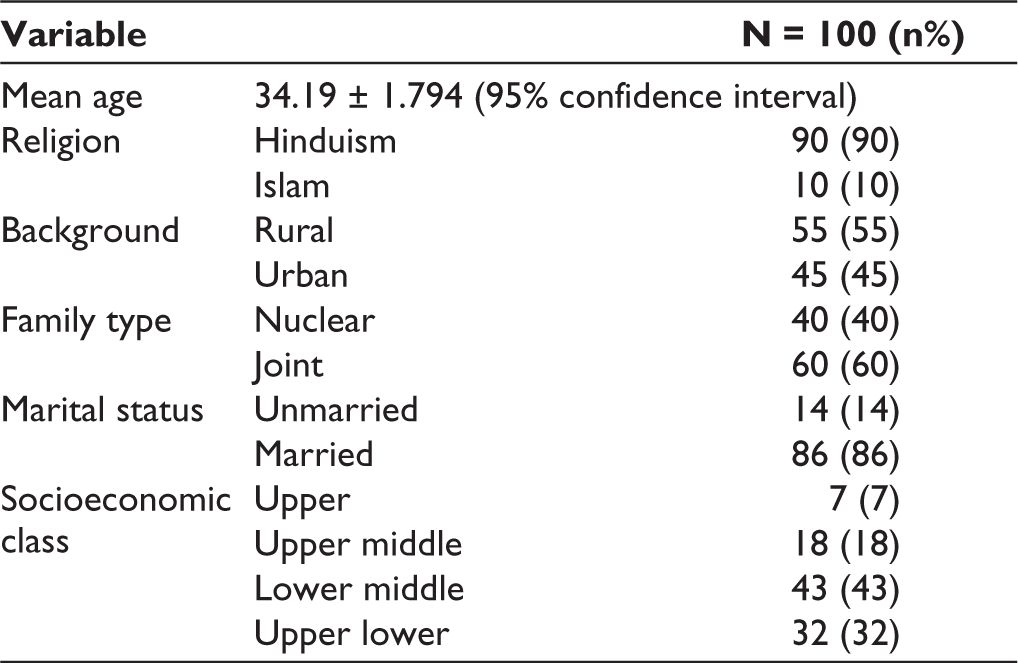
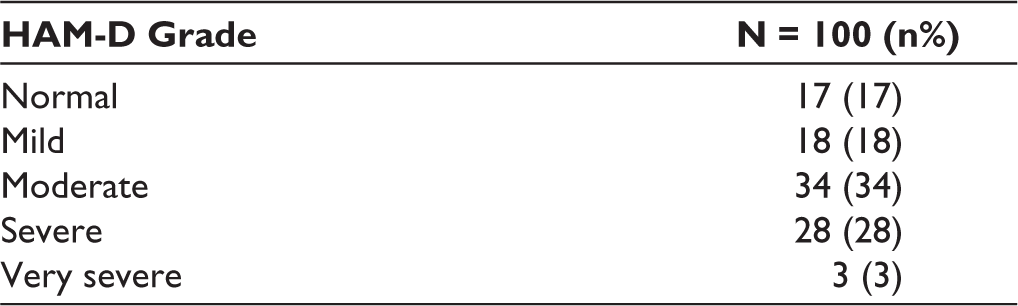
Table 2 shows that majority of the study sample were suffering from moderate depression (34%).
Table 3 observes that among the study sample, maximum patients (65%) were having mild anxiety; patients with mild to moderate anxiety were 26% and moderate to severe were 9%.
Distribution of Subjects According to Severity of Depression.
Distribution of Subjects According to Severity of Anxiety.
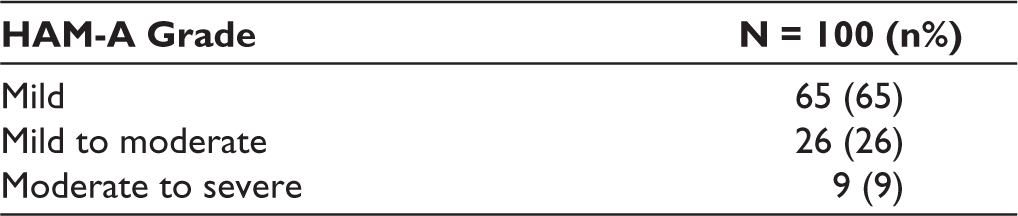
Table 4 shows that in the study sample, sexual pleasure dysfunction, sexual desire dysfunction, sexual desire/interest dysfunction, sexual arousal/erection dysfunction, and sexual orgasmic dysfunction were 71%, 71%, 66%, 68%, and 73%, respectively.
Distribution of Subjects According to Changes in Sexual Functioning Questionnaire.
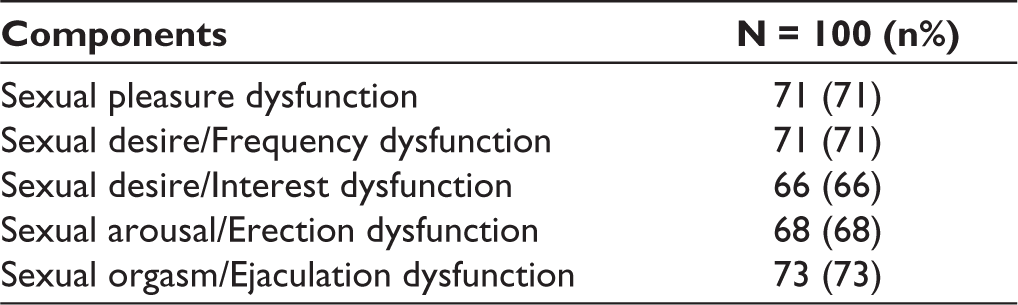
Table 5 depicts that the age group of 30 to 35 years had maximum number of patients, that is, 25%, in which 1% were very severe. Association of depression with age is not significant (P = .954). Hence, these differences observed among the different age groups of quantified depression are merely a chance factor and not because of the true difference in population.
Table 6 shows the Pearson correlation between HAM-D score and sexual desire/interest component of CSFQ-M which yielded r = 0.209 (P = .008). Correlation between HAM-A score and sexual desire/frequency component yielded r = 0.095 (P = .012), sexual desire/interest component yielded r = 0.114 (P = .029), and sexual arousal/erection component yielded r = 0.134 (P = .052).
Association Between Patients Age and Five Components of CSFQ-M Scale.

Pearson Correlation (r) Between HAM-D and HAM-A Scores With Five Components of CSFQ-M Scale.

Conclusions
This study was aimed at studying the occurrence of psychosexual dysfunction in male patients suffering from depression and/or anxiety disorders. The results from the current study indicate decreased sexual interest and sexual function in antidepressant-free men during depressive and/or anxiety episodes.
This study included 100 subjects, aged between 18 and 50 years. In our study, majority of the patients belonged to 34.19 ± 1.794 years of mean age group. As per census 2011, maximum population was from 18- to 23-year age group during the year 2011, that’s why we obtained maximum patients of age group 30 to 35 years in our study. 32 Another study with similar findings included 41 individuals, including 24 men and 17 women with mean age of 31.5 in men and most study subjects were married. 33
In our study, most of the patients belonged to rural area (55%) and were Hindu (90%) which can be explained by the fact that the tertiary care center where the study was conducted is in closer proximity to rural areas. A study with similar findings included 43 patients with mean age of 33.58 years, with maximum patients belonging to Hinduism religion and were married. 34
In our study, majority of subjects was belonging to joint families (60%). Studies with similar findings conducted on 56 sample size were included between age group of 18 to 45 years, majority of the patients (70%) were married, Hindu, belonged to lower and middle socioeconomic group 35 and were living in joint families with primary or secondary education level. 36
We found that highest percentage of participants that experienced dysfunction in sexual desire/frequency and sexual desire/interest belonged to the age group of 36 to 41 years. Majority of the participants who experienced dysfunction in sexual arousal/erection belonged to the age group of 30 to 35 years. Other age group in which more participants experienced dysfunction than rest was 42 to 47 years (14% in sexual desire/frequency; 15% in sexual desire/interest; 14% in sexual arousal/erection). These findings which are consistent with the results of studies by Laumann et al 37 that lower sexual desire and more erection problems associated with increasing age and by Rao et al that ED was reported to be least in 26 to 30 age group and majority of participants with sexual disorders belonged to the age group of 41 to 60 years. 22
In our study, we used CSFQ-M version of 14 questions. By this sexual assessment tool, we were screening 5 components of sexual function, that is, pleasure, interest, frequency, arousal, and orgasm. Similarly, a study used International Index of Erectile Function tool for SD screening and found that 55% were having sexual desire dysfunction, 76% had ED, 53% had orgasmic dysfunction, and 79% had overall satisfaction dysfunction. 34
In our study, on assessing the relation between anxiety and depression with SD, we found that only 1 component of CSFQ-M scale, that is, sexual desire/frequency has a significant association with depression and 3 components of CSFQ-M, that is, sexual desire/interest, sexual desire frequency, and sexual arousal/erection have positive association with anxiety. A study on MDD, OCD, and GAD patients found that 76% of MDD patients had SD (low desire, inability to sustain penile erection); among OCD patients, 50% was reported SD, and 64% patients with GAD had reported SD. 28
Another study found significant association between major depression and sexual desire, arousal, and orgasm. Arousal/Orgasm problems were more frequent in men with later age of onset of major depression. Both reduced sexual desire and erectile or arousal difficulties were reported in approximately 40% of men while delayed ejaculation was reported by 22% of men. 38
A study conducted to assess the sexual function in depressed, impotent, and healthy men found that depressed men reported diminished frequency of sexual thoughts, decreased sexual activity, diminished pleasure from sexual activity, diminished satisfaction with their sex lives, and a decreased frequency of morning erections. 39
At the end, our findings suggest that certain areas of sexual functioning are impacted by depression and/or anxiety disorders symptoms. The hypothesis that those with depression and/or anxiety would have lesser overall sexual functioning is supported in some areas by the results. One hypothesized reason for this finding may be that these individuals’ constant hyper vigilance and rumination about physiological sensations may distract so much that they rarely respond to sexual stimuli or do not allow themselves to engage in sexual fantasies. Those with comorbid anxiety disorders had less participation in sexual activity and experienced less sexual satisfaction. Despite its limitations, this study has a number of potential implications for the assessment of sexual functioning in depression and/or anxiety disorders patients. The relationship between depression and/or anxiety disorders and SD appears to be well established in the literature. However, although this relationship has found in a number of studies, the relationship appears to be highly variable. It appears to vary according to sample selection, size, sociodemographic factors, and selection of tools.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Review Committee
Netaji Subhash Chandra Bose Subharti Medical College, Swami Vivekanand Subharti University, Meerut vide letter no. SMC/IEC/2018/52/3040 dated November 29, 2018.