
Abstract
Background:
Sexual dysfunction is one of the major problems associated with the chronic use of alcohol. Sexual dysfunction is also significantly associated with marital adjustment and quality of life.
Aim and Objectives:
To determine the prevalence of sexual dysfunction and its association with marital adjustment and quality of life among persons with alcohol dependence syndrome (ADS) and to compare with the healthy control group.
Materials and Methods:
The present study used a cross-sectional, comparative, and descriptive research design. A purposive sampling technique was used to select the sample of 128 (64 patients with ADS and 64 healthy control persons) between the ages of 21 and 50, from the Department of Addiction Medicine, LGB Regional Institute of Mental Health (LGBRIMH), Tezpur, Assam. Sociodemographic and clinical data sheet, the Arizona Sexual Experience Scale (ASEX), the Severity of Alcohol Dependence Questionnaire (SDAQ), the Alcohol Use Disorders Identification Test (AUDIT), the International Index of Erectile Dysfunction (IIED), and The Drug Abuse Screening Test scales (DAST) were used.
Results:
The study revealed a higher prevalence of sexual dysfunction in the ADS group (64%) compared to the healthy control group (35.9%) (Chi-square = 46.916; p < .001). Marital satisfaction was significantly lower in the ADS group than in the healthy control group (Fisher’s exact test = 76.932; p < .001). Quality of life was also diminished in the ADS group, particularly in the physical (t = −5.310; p <.001), social (t = −4.481; p < .001), and environmental domains (t = −4.250; p < .001). Furthermore, sexual dysfunction exhibited a significant negative correlation with marital adjustment (r = −0.676; p < .01) and all domains of quality of life [physical domain (r = −0.235; p < .001), social domain (r = −0.383; p < .001), and environmental domain (r = −0.383; p < .001)].
Conclusion:
The prevalence of sexual dysfunction and erectile dysfunction was high in persons with alcohol dependence syndrome as compared to the healthy control group and it has a relationship with marital adjustment and quality of life. The findings highlight the importance of screening and evaluating sexual dysfunction in individuals with alcohol dependence. Comprehensive pharmacological and nonpharmacological services are warranted to address the unique needs of this population, promoting both recovery from alcohol dependence and improvement in overall quality of life.
Keywords
Introduction
Sexual dysfunction is a psychological or pathological condition where an individual is not able to perform sexual activities as he or she wishes. There are multiple factors for sexual dysfunction. The most common factors are physiological, psychological, and social. 1 Alcohol dependence syndrome is known to lead to sexual dysfunction. 2 The prevalence of sexual dysfunction was present in 61% of the respondents with persons with alcohol dependence syndrome. 3 Pendharkar et al. 4 found that 58.4% of participants with alcohol dependence syndrome had sexual dysfunction and alcohol use was significantly associated with sexual dysfunction. 4 Sexual dysfunction is comparatively less in a person without a history of alcohol consumption. 4
Alcohol dependence syndrome not only leads to sexual dysfunction but also impacts quality of life and marital adjustment. Many studies showed that sexual dysfunction is associated with the quality of the person and marital adjustment in a person with alcohol dependence syndrome.5-8 Quality of life is significantly associated with the sexual life of a person. 9 Studies show that the quality of life was poor among patients with alcohol use disorder and it was associated with the severity of alcohol dependence quality of life. 10 Alcohol use disorder is quite prevalent among the general population in the northeastern region of India. Sexual dysfunction in persons with alcohol dependence is often unrecognized and not reported by patients in the clinical setting. Moreover, sexual dysfunction can lead to stress and conflict which can further increase the consumption of alcohol and it can lead to dissatisfied marital and poor quality of life. 11 Various studies conducted in India reported sexual dysfunction due to the use of alcohol, but there are few studies that have been reported from northeastern India that are highly insufficient. Further, alcohol dependence, marital satisfaction, quality of life, and sexual functioning have been extensively researched individually, but not concerning each other. Hence, the present study aims to assess the sexual dysfunction, marital adjustment, and quality of life in persons with alcohol dependence syndrome and to compare it with healthy control persons in the hospital settings.
Materials and Methods
The present study used a cross-sectional, comparative, and descriptive research design. A purposive sampling technique was used to select the sample of 128. A total of 64 consecutive patients of alcohol dependence syndrome and 64 healthy control groups were selected, between the ages of 21 and 50, registered to the Department of Addiction Medicine, LGB Regional Institute of Mental Health (LGBRIMH), Tezpur, Assam. The sample size was calculated as 64 as per G power software, with here Alpha error probability being 0.05, and power (1-Beta error probability) being 0.80. The data was collected from April to November 2022. All the study participants were informed about the purpose of the research study and their written formal consent was obtained before participation. Study participants were informed that all their information would be kept anonymous and confidential, and they were provided with information about the nature and purpose of the research study, the procedure, and the right to withdraw from their study. Ethical clearance was obtained from the Institutional Ethical Committee.
Instruments Used for the Study
Sociodemographic and Clinical Sheet
The researcher developed the self-structured sociodemographic data sheet to assess the sociodemographic characteristics of alcohol dependence syndrome patients and the healthy control group. The variables included in the sheet were age, gender, religion, sex, education, socioeconomic status, types of family, residence, etc.
Arizona Sexual Experiences (ASEX) (McGahuey et al. 12 )
This scale consists of five items, which has been developed for assessing sexual dysfunction. This scale will assess the five domains of sexual function such as sex drive, arousal, and vaginal lubrication (female/penile erection (only for males)), ability to reach orgasm, and satisfaction from orgasm. The scoring is 5-30. A higher score will indicate higher sexual dysfunction. ASEX showed good internal consistency (Cronbach’s alpha’s 0.89 and 0.90) and test–retest reliability (r = 0.88, p < .001). 12
WHOQOL-BREF Scale
This scale was developed by the WHO Quality of Life group in 1995. This scale is consisting of 26 questions. This scale is used to assess the psychological, social, environmental, and physical domains of quality of life. Each individual item of the WHOQOL-BREF is scored from 1 to 5 on a response scale, which is stipulated as a five-point ordinal scale. The scores are transformed on a scale from 0 to 100 to enable comparisons to be made between domains composed of unequal numbers of items. The WHOQOL-BREF had good internal consistency as Cronbach’s alpha coefficient for the overall scale was 0.91. 13
Marital Adjustment Test (MAT)
This scale was developed by Locke and Wallace in 1959. It is a 15-item scale that measures marital satisfaction. This scale is used to assess contentment and communication, Leisure and sociality, Intimacy, and shared Philosophy domains. The maximum score is 158. Score 130-158 is for unusually satisfied, 110-130 for satisfied, 90-110 for average, 70-90 for dissatisfied, and 2-70 for very dissatisfied. MAT’s reliability falls between Cronbach alphas of 0.72 and 0.83. 14
The Severity of Alcohol Dependence Questionnaire
The Severity of Alcohol Dependence Questionnaire was developed by Stockwell, Murphy, and Hodgson in 1983. The total score range is from 0 to 60. Less than 16 score indicates mild alcohol dependence, 16-30 indicates moderate alcohol dependence, and 31 or higher indicates severe alcohol dependence. Cronbach’s alpha reliability coefficient of SADQ was found to be α = 0.914. 15
International Index of Erectile Functioning
The IIEF was developed by Rosen et al. 1997. It is a 15-item scale. It is used to assess the five domains of sexual function, erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall satisfaction. Total scores of 22–25 indicate no erectile dysfunction, 17–21 indicate mild erectile dysfunction, 12–16 indicate mild to moderate erectile dysfunction, 8–11 indicate moderate erectile dysfunction, and 5–7 indicate severe erectile dysfunction. The IIEF score demonstrated adequate internal consistency with a high Cronbach’s alpha of 0.94 in both patient and reference group. 16
AUDIT-10
The Alcohol Use Disorders Identification Test (AUDIT) is a 10-item screening tool developed by the World Health Organization (WHO, 1982) to assess alcohol consumption, drinking behaviors, and alcohol-related problems. AUDIT was developed in 1989 and later on, it was updated in 1992. 17 AUDIT score ranges from 0 to 40. A score of 1–7 suggests low-risk consumption; scores from 8–14 suggest hazardous or harmful alcohol consumption, and a score of 15 or more indicates the likelihood of alcohol dependence according to World Health Organization (WHO) guidelines. Internal reliability for AUDIT Cronbach’s alpha test-retest reliability ranges from 0.64 to 0.92. 17
The Drug Abuse Screen Test (DAST-10)
The drug abuse screen was developed by Harvey Skinner in 1982. This scale is 12 items self-reported scale. It is used to assess drug use behaviors. A score of 0 indicates no problems, a score of 1–2 indicates low level, a score of 3–5 indicates moderate level, a score of 6–8 indicates substantial level, and a score of 9–10 indicates severe level. The DAST-10 has excellent internal consistency reliability (alpha) at 0.95 for the total sample and 0.86 for the drug-use sample. 18
Ethical Considerations
Ethical clearance was obtained from the institutional authorities to carry out the study. Written informed consent was obtained after an explanation of the research. The study was carried out at the Outpatient Department of LGB Regional Institute of Mental Health, Tezpur, Assam in accordance with the principles as enunciated in the Declaration of Helsinki.
Statistical Analysis
Both descriptive and inferential statistics were used. Analysis was conducted using the SPSS program (Version 23.0; IBM Corporation, Armonk, NY, USA).
Results
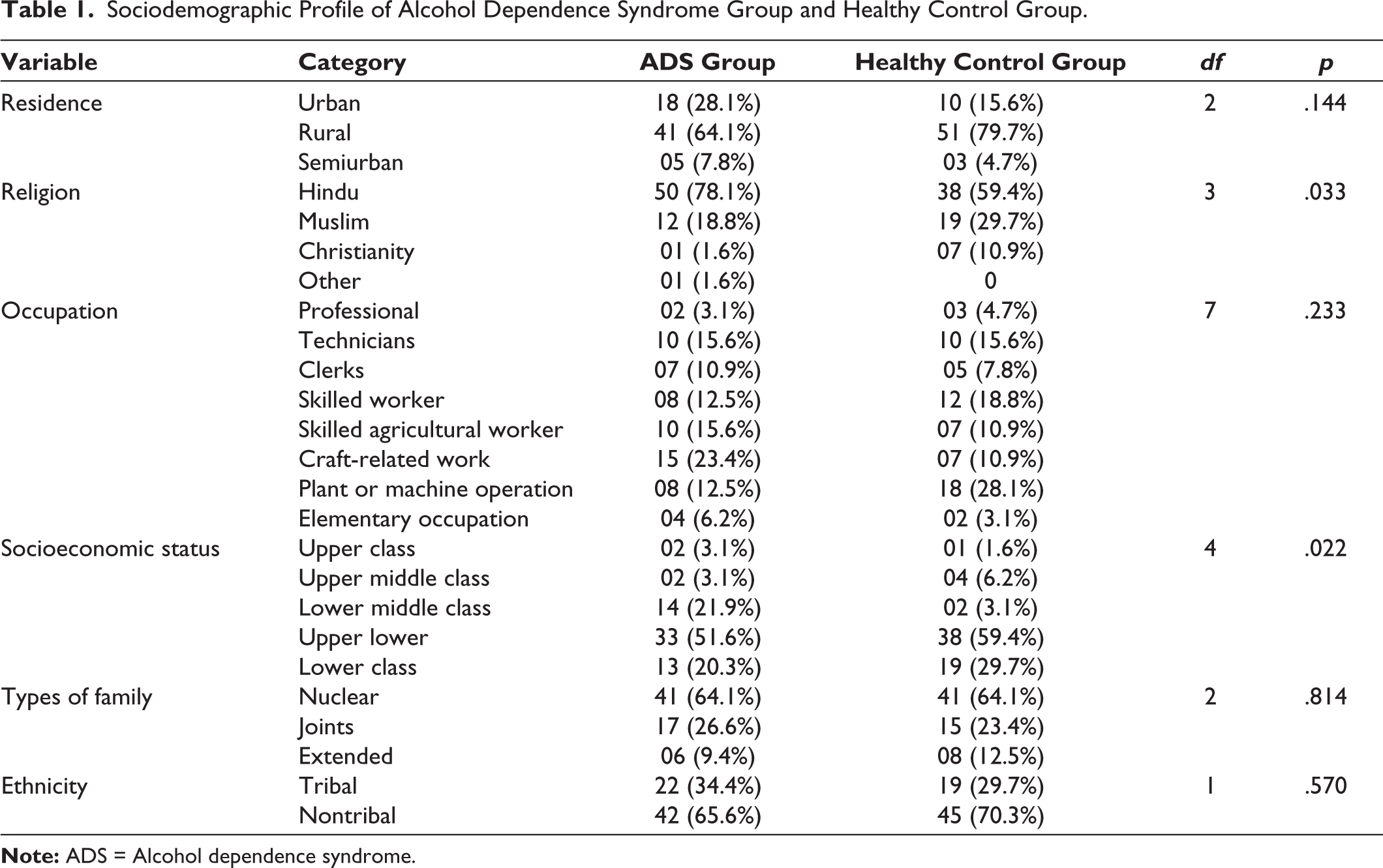
Table 1 shows the sociodemographic profile of the ADS group and the healthy control group. In both groups, majority of the respondents belonged to rural areas. When the chi-square was computed, no significant difference was found between the two groups (p = .144, df = 2). 71.8% of respondents belonged to the Hindu religion in the ADS group and in the healthy control group, 38 (59.4%) respondents belonged to the Hindu religion. When the Fisher exact test was computed, significant difference was found between the two groups in religion (p = .033, df = 3) and socioeconomic status (p = .022, df = 4). In occupation, a significant difference was found in both groups (p = .233, df = 7). When the chi-square was computed, no significant difference was found between the group in ethnicity (p = .570, df = 1) and types of family (p = .814, df = 2). The finding shows that 42.2% (27) of respondents drink Indian-made alcohol and 35.9% of respondents drink foreign-made alcohol.
Sociodemographic Profile of Alcohol Dependence Syndrome Group and Healthy Control Group.
The mean duration of alcohol dependence was 10.37 years (M = 10.37, SD = 6.02). The mean age at first drink was 22.5 years (M = 22.5, SD = 4.0). The finding also shows that the mean age of dependence was 27.71 years (M = 27.71, SD = 4.0). The study’s results indicate that in the ADS group, the average age of spouses was 32.29 years (M = 32.29, SD = 7.47), while in the healthy control group, it was 31.78 years (M = 31.78, SD = 8.30). When the independent t-test was computed, no significant differences were found among the two groups (t = 0.369, p = .713). In the study, the finding shows that the mean duration of marriage was 16.81 years in the ADS group (M = 16.81, SD = 6.83) and the mean duration of marriage was 16.68 years in the healthy control group (M = 16.68, SD = 7.08). When the independent t-test was computed, no significant difference was found between the two groups (t = 0.102, p = .919). In the study, the findings show the mean age at marriage of respondents was 21.28 years (M = 21.28, SD = 4.06) in the ADS group and the mean age at the marriage of the respondents was 20.48 years (M = 20.48, SD = 2.28) in the healthy control group. When the independent t-test was computed, no significant difference was found among the two groups (t = 1.36, p = .174).
In the study, 64.1% of respondents from the ADS group and 6.2% of respondents in the healthy control group had sexual dysfunction. When the Chi-square was computed significant difference was found between the ADS and healthy control group (Chi-square = 46.916; p < .001) (Table 2).
In terms of erectile dysfunction, 35.5% of respondents in the ADS group had mild erectile dysfunction, 23.4% had mild to moderate, and 7.8% had moderate erectile dysfunction. Comparatively, in the healthy control group, 20.3% experienced mild, 12.5% had mild to moderate, and 1.6% had moderate erectile dysfunction. Statistical analysis with the Chi-square test again showed significant differences between the two groups (χ² = 15.874; p < .001) (Table 2).
Sexual Dysfunction, Erectile Function, Marital Adjustment, and Quality of Life Among the ADS Group and Healthy Control Group.
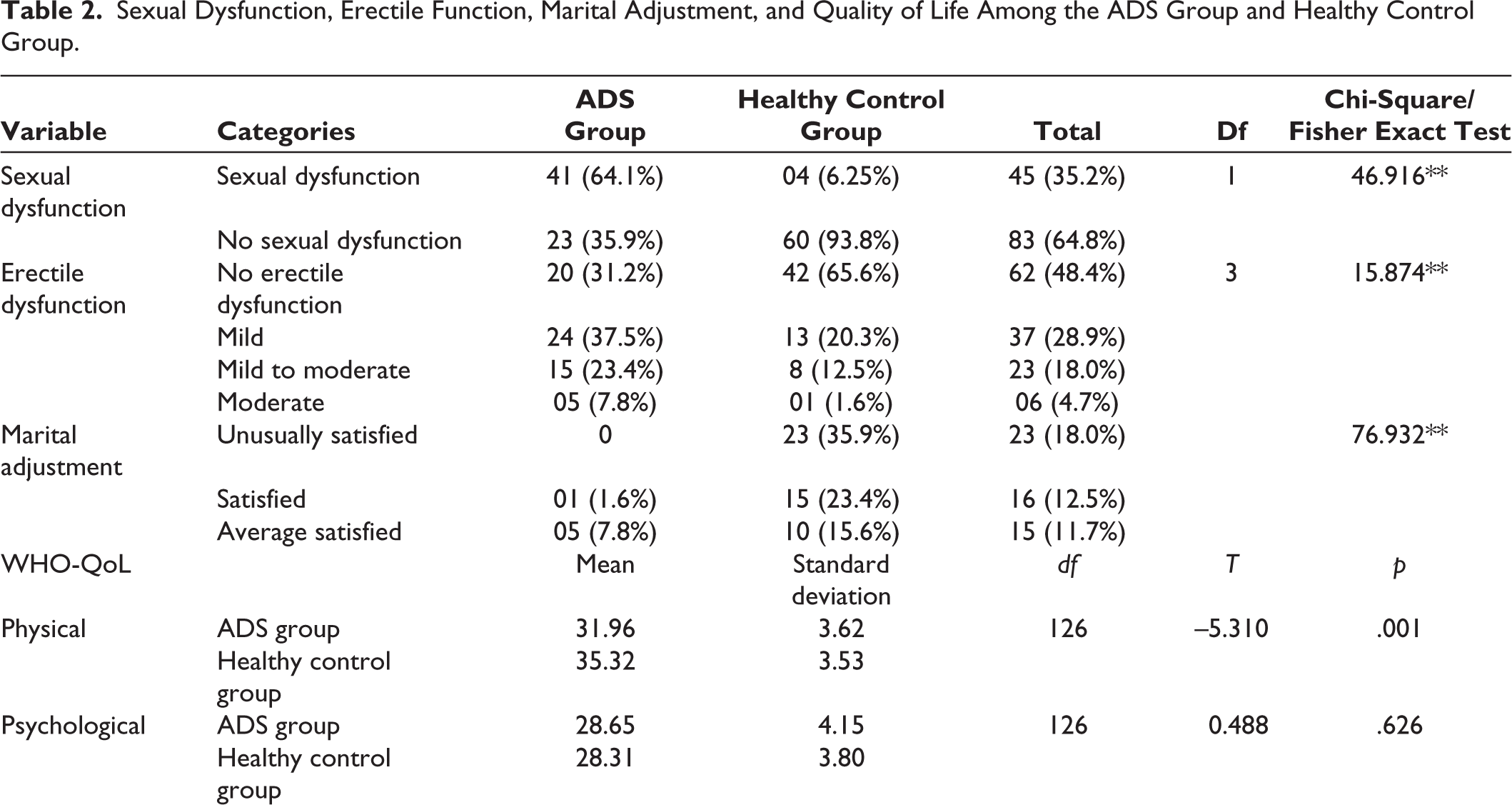
Marital adjustment also varied significantly between the two groups. Only 1.6% of respondents in the ADS group reported being satisfied with their marital adjustment, while a striking 75% were very dissatisfied. In contrast, the healthy control group had 35.9% of respondents reporting unusually high satisfaction, and only 10.9% reported being very dissatisfied. The differences in marital satisfaction between the groups were confirmed as significant using the Fisher’s exact test (Fisher’s exact test = 76.932; p < .001) (Table 2).
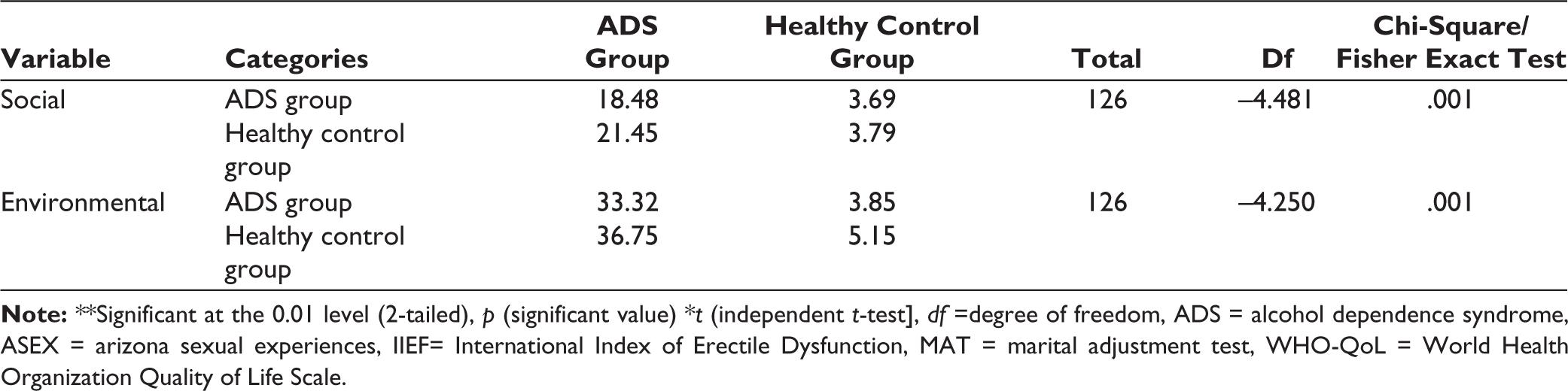
Regarding quality of life, the study used an independent t-test to compare the two groups across various domains. Significant differences were observed in the physical (t = −5.310; p < .001), social (t = −4.481; p < .001), and environmental domains (t = −4.250; p < .001), with the ADS group consistently showing poorer outcomes compared to healthy controls (Table 2).
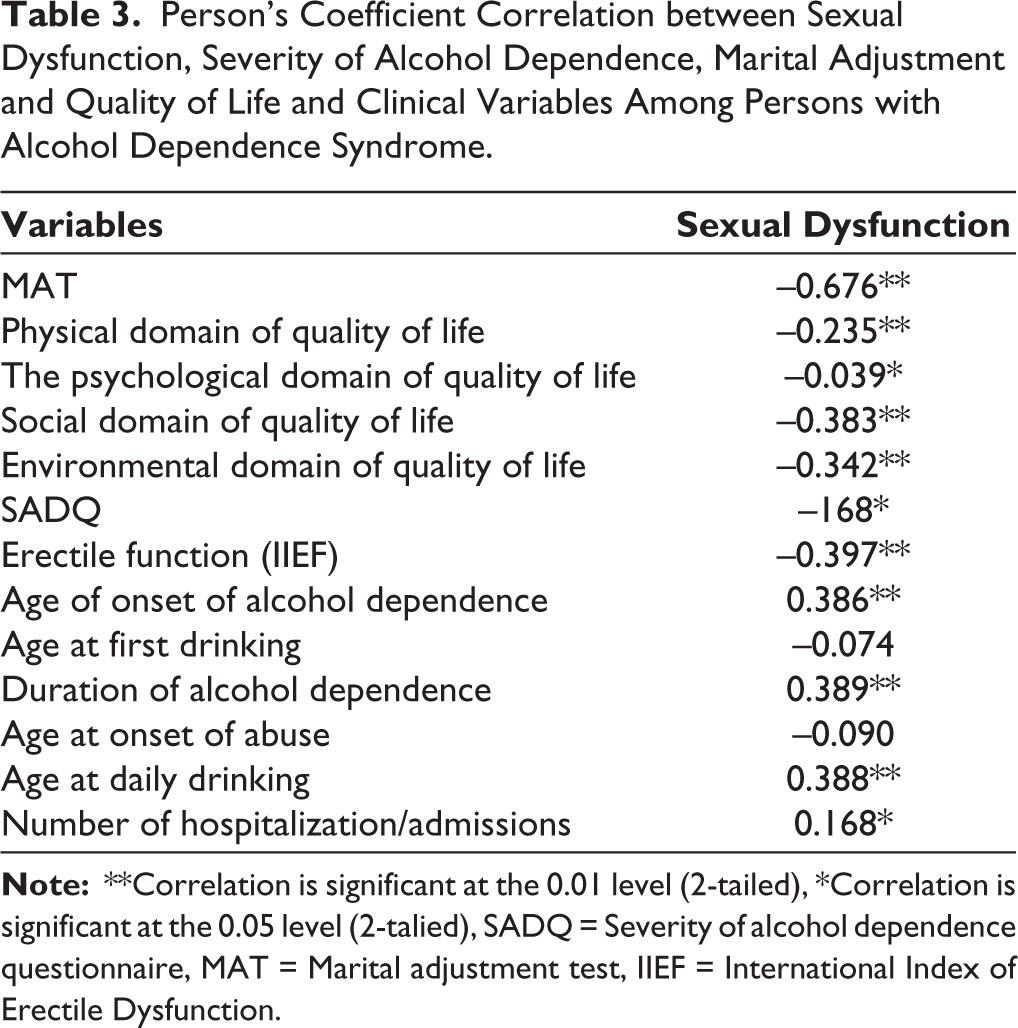
Table 3 displays the correlation between sexual dysfunction, the severity of alcohol, marital adjustment, and quality of life. The result revealed that sexual dysfunction had a significant negative correlation with marital adjustment (r = −676; p < .01). In the study, the finding shows that the sexual dysfunction had a significant negative correlation with erectile dysfunction (r = −0.397; p < .001). The above table also shows that all the domains of quality of life had a significant negative correlation with sexual dysfunction. Table 3 shows that age of onset has a significant positive correlation with sexual dysfunction (r = 0.386, p < .01), a negative correlation with age at first drinking (r = −0.74), significant positive correlation with a duration of alcohol dependence (r = 0.389, p < .01), a negative correlation with age at onset of abuse (r = −0.090), a significant positive correlation with age at daily drinking (r = 0.388, p < .01) and a positive correlation with numbers of admission (r = 168, p < .05).
Person’s Coefficient Correlation between Sexual Dysfunction, Severity of Alcohol Dependence, Marital Adjustment and Quality of Life and Clinical Variables Among Persons with Alcohol Dependence Syndrome.
Discussion
The finding of the study shows that the prevalence of sexual dysfunction in the ADS group was 64.1% and 6.2% of respondents in the healthy control group had sexual dysfunction. The finding shows that 35.5% of the respondents had mild erectile dysfunction, 23.4% of respondents had mild-to-moderate erectile dysfunction and in the healthy control group, 7.8% of respondents had moderate erectile dysfunction in the ADS group and 20.3% of respondents has mild erectile dysfunction, 12.5% respondents had mild-to-moderate erectile dysfunction and 1.6% respondents had moderate erectile dysfunction in the healthy control group. Findings from previous studies also report that sexual dysfunction appears to be common among male patients with alcohol dependence syndrome and the most common being erectile dysfunction and premature ejaculation.5,11,19
Mandal and Spoorthy 5 found that the prevalence of sexual dysfunction was high among persons with alcohol dependence and erectile dysfunction was present (26%) as compared to healthy control. Persons with alcohol dependence had a significantly higher degree of sexual dysfunction, poor sexual satisfaction, and low quality of life compared to healthy controls. Rohilla et al. 6 found that more than half of the men (58.6%) with alcohol dependence were found to have sexual dysfunction compared to only one-fifth in the control group (18.5%) and the majority of persons with alcohol dependence had difficulties in erection and arousal. Pendharkar and Grover 4 found that sexual dysfunction was seen in 58.4% of patients in the ADS group, the highest frequency was seen for dysfunction for arousal (57.4%), problems in desire (54.4%), erection (36.6%), satisfaction with orgasm (34.6%), and ability to reach orgasm were least affected (12.87%). In contrast, in control group participants, the prevalence of sexual dysfunction in each domain was also significantly less than that seen in the AD group. 4
Our study findings show that marital adjustment was poor among the ADS group as compared to the healthy control and marital adjustment was better in spouses of normal healthy control as compared to spouses of patients with alcohol dependence. Balaganeshan and Ragupathy,20,21 found poor marital quality of life in spouses of alcohol-dependent patients than controls. A significant difference was found between ADS and the healthy control group in the physical domain, social, and environmental. 22 The finding shows that the ADS group was having poorer quality as compared to the control group. Research findings also suggest that persons with alcohol dependence had poor quality.23-25 Another similar study by Solomon et al. 26 found that the quality of life was poor in the alcohol dependence group compared with the normal population. There was a significant difference between the alcohol dependence syndrome group and the healthy normal group as in the present study.
Our study findings show that sexual dysfunction had a significant negative correlation with marital adjustment and also show that all the domains of quality of life had a significant negative correlation with sexual dysfunction. A similar study by Solomon et al. 26 found that the physical, psychological, and environmental domain of quality of life had a positive correlation with the duration of alcohol dependence and the study also revealed that social relationship domain of quality of life had a negative correlation with alcohol dependence. A study conducted by Rohilla et al. 6 found that male persons with alcohol dependence had significantly lowered MAT scores than the control group. Marital adjustments had a large negative correlation with the severity of alcohol dependence and sexual dysfunction (ASEX).
The finding of the study shows that age of onset has a significant positive correlation with sexual dysfunction, a significant negative with duration of alcohol dependence, a negative correlation with age at onset of abuse, a significant positive correlation with age at daily drinking, and positive correlation with numbers of admission. Studies show that the total scores on ASEX were positively correlated with the duration of alcohol use and dependence. 6 A similar study by Prabhakaran et al. 11 found that sexual dysfunction had a positive correlation with age at first drink followed by a duration of alcohol dependence, the severity of alcohol dependence, the amount of alcohol consumed per day, and had a negative correlation with age of the patient. 11
Limitations of the Study
However, certain limitations were also identified like sample size was small; a larger sample size would be required for better generalization of the results. We used a nonrandomized sampling technique in this study. The present study was cross-sectional. The cross-sectional nature of our study shows an association rather than a causal relationship. Sexual dysfunction in individuals with alcohol dependence syndrome (ADS) is a multifaceted issue influenced by a range of physiological, psychological, and social factors.27,28 Other psychosocial elements (psychological distress, interpersonal relationship issues, and broader social influences) which may be additional contributory factors for sexual dysfunction in alcohol dependence syndrome, were not explored in the current study.
Clinical Implication
Sexual dysfunction in alcohol-dependent patients had a deleterious effect on marital functioning and also affected the quality of life. The findings of the study will help us to better understand of sexual dysfunction of the person with alcohol dependence syndrome. Therefore, psychosocial intervention could be planned for the person with alcohol dependence syndrome to address these issues. Due to limited research work in this area, sexual dysfunctions in alcohol-dependent patients are often neglected and unexplored in routine clinical practice. Moreover, this study also enlightens the need to regularly assess sexual function in alcohol dependence syndrome (ADS) patients in all the settings of treatment. Planning and implementing newer alcohol policies and regulations can be recommended based on findings from such studies. Sensitization programs at schools and colleges highlighting this aspect, as well as interventional programs and treatment effectiveness studies, comparing the various methods to correct alcohol-induced sexual dysfunction, can be done.
Conclusion
The evidence indicates that individuals with alcohol dependence syndrome experience higher rates of sexual and erectile dysfunction when compared to healthy controls. These dysfunctions, alongside poor marital adjustment, are intricately linked to the severity of alcohol dependence and further correlate with diminished quality of life across physical, psychological, social, and environmental dimensions. Given these findings, it is imperative to incorporate routine screening and evaluation of sexual dysfunction in the management of alcohol dependence. Additionally, addressing these issues requires the implementation of comprehensive and tailored psychosocial services that aim to enhance the quality of life and improve the overall health outcomes for individuals struggling with alcohol dependence and its concurrent sexual dysfunctions.
Footnotes
Acknowledgements
Appreciation is extended to the participants who participated in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was reviewed and approved by the Institutional Ethics Committee (IEC), LGBRIMH, Tezpur, Assam, India.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participants were thoroughly informed about the purpose of the study and provided their consent to participate.