
Abstract
Aim:
This study aimed to investigate the prevalence of sexual dysfunction in individuals with epilepsy and its impact on overall quality of life.
Methods:
One hundred and twenty patients diagnosed with epilepsy and 50 healthy controls were assessed on Changes in Sexual Functioning Questionnaire Short-Form (CSFQ-14) to estimate the prevalence of sexual dysfunction. Epilepsy patients were additionally evaluated for psychiatric morbidity using structured diagnostic interview.
Results:
On CSFQ-14, 97.5% of epilepsy patients experienced sexual dysfunction, surpassing controls. CSFQ’s suggested cutoff norms revealed prevalence of impaired pleasure/arousal (97.5%) to be the most common dysfunction, followed by reduced desire (93.33%), orgasm dysfunction (89.16%), painful erection (61.7%), and painful orgasm (30%). Compared to healthy subjects, epilepsy patients displayed significantly higher prevalence of sexual dysfunction across all domains (P < .001). Patients with psychiatric morbidity had significantly higher prevalence of sexual dysfunction, when compared to those without psychiatric morbidity. Overall, the presence of sexual dysfunction had a significant negative impact on the quality of life.
Conclusion:
The present study suggests a very high prevalence of sexual dysfunction in epilepsy patients and emphasizes the need for holistic care in epilepsy patients. Healthcare providers must recognize and address sexual dysfunction to enhance the overall quality of life of patients with epilepsy.
Introduction
Epilepsy is characterized by recurrent epileptic seizures and afflicts approximately 50 million individuals globally.1,2 Beyond the physical seizures, epilepsy poses formidable challenges to emotional, behavioral, social, and cognitive well- being, significantly impacting the overall quality of life (QoL) for those living with the condition. Patients with epilepsy may confront psychiatric comorbidities that further exacerbate the burden on their mental health and daily life. Additionally, societal stigmatization of epilepsy further compounds the challenges faced by those experiencing recurrent seizures. 3
Amidst the multifaceted impact of epilepsy, an often-overlooked aspect demanding meticulous attention is its association with sexual dysfunction. Both epilepsy itself and antiepileptic drugs (AEDs) prescribed for its management can significantly affect the hormone levels, potentially compromising sexual function. In women with epilepsy, AEDs can perturb the metabolism of endogenous sex hormones, resulting in diminished levels of estrogens and androgens. 4 Moreover, sexual activity itself may potentially trigger seizures, further compounding the complexities. 5
AEDs can significantly influence sexual functioning in people with epilepsy (PWE), with enzyme-inducing drugs like carbamazepine and phenytoin adversely affecting sex hormone levels and precipitating sexual dysfunction. 6 In contrast, novel non-enzyme-inducing AEDs generally pose a diminished risk of inducing sexual dysfunction. 7
Apart from the direct effects of epilepsy and AEDs, comorbid psychiatric morbidities, such as depression and anxiety, are acknowledged contributors to sexual dysfunctions in PWE. 8 Psychosocial factors, including stigma, social isolation, and anxiety concerning seizures during sexual activity, wield substantial influence over sexual dysfunction. 9
In terms of prevalence of sexual dysfunction among PWE, in one of the earliest descriptions that emerged in 1954 reported prevalence of hyposexuality (grossed reduced interest in all aspects of sexual life) to be 72% among patients with complex partial seizures. 10 Later studies that relied on different scales have estimated the prevalence of sexual dysfunction among females to range from 10% to 75% and among men to range from 3% to 60%. Studies that have compared the prevalence of sexual dysfunction among PWE with healthy controls suggest that prevalence of sexual dysfunction among PWE is about 1.5 to 2 times than that seen in healthy controls. Among men, erectile dysfunction is reported to be the most common abnormality, whereas among women, the most common affected domains include reduced sexual desire and arousal. However, it is important to note that available literature on sexual dysfunction among PWE is limited and the studies have been limited to small sample size studies (< 100 PWE) and have used different scales to assess the sexual dysfunction. 11 There is limited data from developing countries. Further, many studies have not evaluated the impact of psychological factors like depression on the prevalence of sexual dysfunction.
The ramifications of sexual dysfunction on overall QoL cannot be underestimated, as it possesses the capacity to permeate various aspects of an individual’s personal and social life. 12 However, there is also lack of data on the impact of sexual dysfunction on QoL. Hence, there is a need to expand the literature in this area. Grasping the ramifications of epilepsy on sexual functioning is quintessential for formulating targeted interventions and support mechanisms to ameliorate the overall QoL. This study aimed to examine the prevalence of sexual dysfunction in individuals with epilepsy and compare it with non-epileptic individuals. An additional aim was to explore the various correlates of sexual dysfunction in patients with epilepsy.
Methodology
This cross-sectional investigation was undertaken at a tertiary care multispecialty teaching hospital. Assessment of sexual dysfunction was part of the larger study that assessed psychiatric morbidity, cognitive impairment, suicidality, sexual dysfunction, stigma, QoL, and side effects of the ongoing medications. This article focuses on sexual dysfunction. Data on prevalence of psychiatric morbidity has already been published. 9
All participants were recruited after procuring their informed consent in writing, and the study received approval from the institute’s ethics committee. Purposive sampling was employed to collect the study cohort. The inclusion criteria necessitated participants to meet the diagnosis of idiopathic epilepsy [as defined by the International League Against Epilepsy (ILAE) and Epilepsy Guidelines Task Force criteria], 13 with a minimum duration of 1 year and an age range of 18-50 years. Patients with severe illness that impeded their ability to cooperate for the interview, those with a history of psychiatric morbidity predating the onset of epilepsy, individuals diagnosed with intellectual disability, and patients presently not on antiepileptic medications were excluded from the recruitment.
The control group was recruited from the caregivers of the patients and the hospital staff. To be included in the study, the control group was required to be aged 18-50 years and free from any diagnosed psychiatric disorder and epilepsy.
All patients with a clinical diagnosis of epilepsy, attending the outpatient services or admitted to the inpatient unit of Department of Neurology, were approached for participation. They were apprised of the study’s nature and a written informed consent was procured.
A self-designed form was employed to gather sociodemographic and clinical profile details. The Changes in Sexual Functioning Questionnaire Short-Form (CSFQ-14) was administered to assess sexual dysfunction. This 14-item self-rated scale assesses sexual functioning across all three phases of the sexual response cycle. Each item is appraised using a 5-point Likert scale, with higher scores connoting heightened frequency or greater enjoyment/pleasure (e.g., 1 = never to 5 = everyday). For two items (item 10, assessing priapism, and item 14, evaluating painful orgasm), elevated sexual functioning corresponds to lower frequency (e.g., 1 = everyday to 5 = never). Items 10 and 14 are included in the total score (after the reverse scoring) but not in any subscale score. Notably, the scale boasts robust construct validity and internal reliability. 14 Psychiatric morbidity was assessed by a psychiatrist using the DSM-IV criteria.
The severity of depression was assessed on Beck Depression Inventory (BDI). 15 Quality of life was assessed by using Quality of life in Epilepsy (QOLIE-31) scale. 16
A descriptive analysis was undertaken utilizing mean, standard deviation (SD), and range for continuous variables. Discontinuous variables were scrutinized via frequency and percentages. Comparisons were done using the Chi-square test, and t-test.
Results
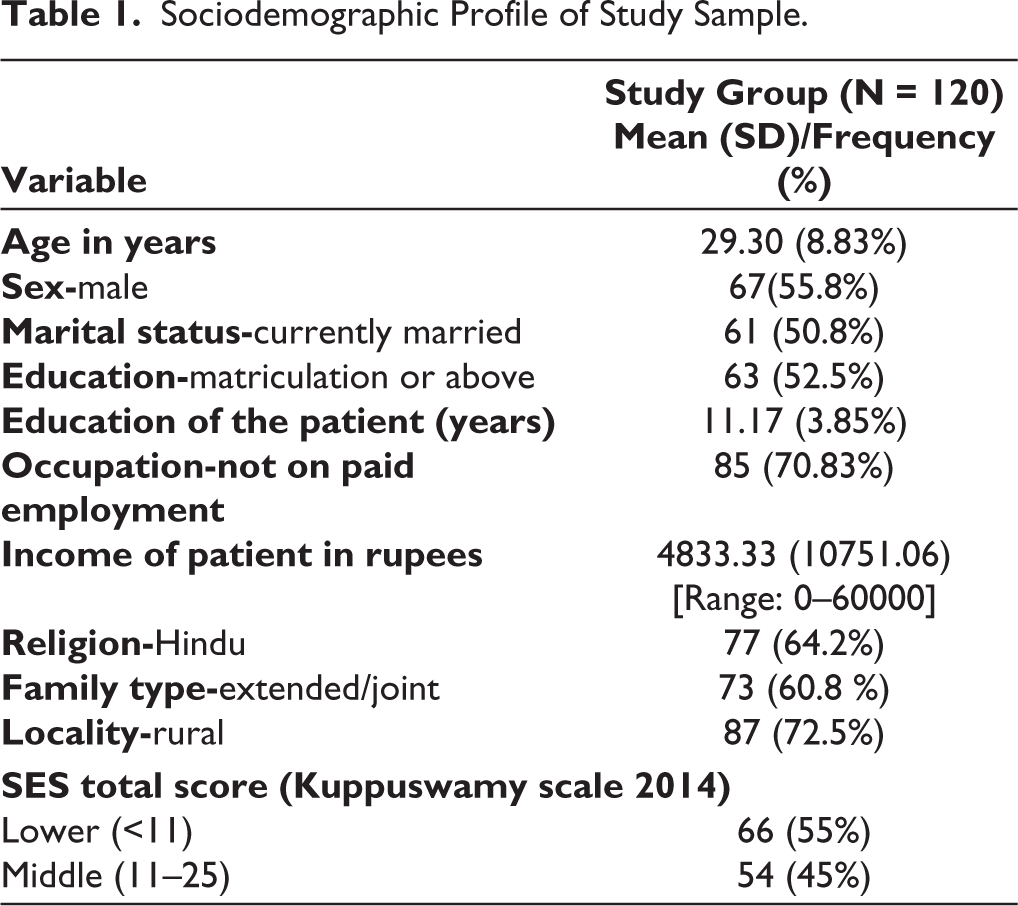
The study included 120 patients with a mean age of 29.3 (SD: 8.83) years. More than half of the study participants were male, married, educated (matriculation or above), not on paid employment, from rural locality, and from a lower socio-economic status (Table 1).
Sociodemographic Profile of Study Sample.
Clinical Profile of Total Study Sample
The mean age of onset of epilepsy was 17.09 (SD-6.9) years, the mean duration of illness was 12 (SD-7.5) years, and the mean duration of treatment at the time of assessment for this study was 10.5 (SD-7.32). The mean number of lifetime episodes of seizures was 71.62 (SD-120.3; median: 1) and the mean number of episodes in the last 6 months was 2.33 (SD-3.81; median 1). Nearly half of the patients were on valproate (49.17%), around one-fourth on levetiracetam (26.7%), and about one-fifth were on phenytoin (22.5%). As per the DSM-IV criteria, 75% of the participants had a lifetime psychiatric diagnosis and 68.3% had current psychiatric diagnosis. A small proportion (15.8%) had at least one current/lifetime diagnosis of substance use disorder (SUD). Depressive disorders were the most common psychiatric diagnosis. The mean BDI score for the whole group was 16.43 (SD: 10.84).
QoL as Assessed on Epilepsy QoL Scale
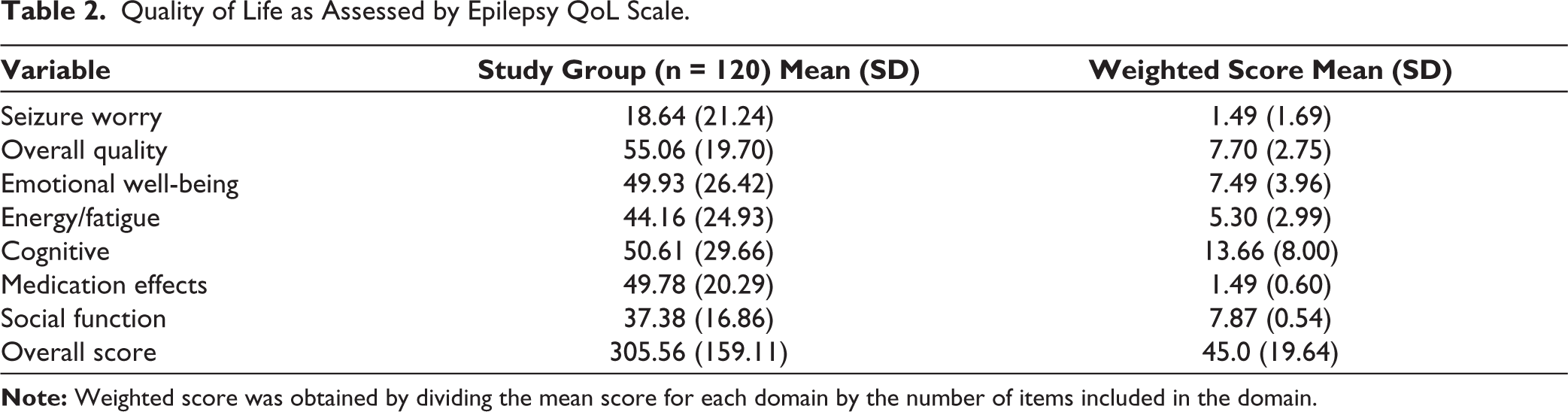
The mean quality of life score was highest for the overall QoL, and this was followed by the domains of cognitive impairment, emotional well-being, medication side effects, social function, and the least score was noted for the domain of seizure worry (Table 2).
Quality of Life as Assessed by Epilepsy QoL Scale.
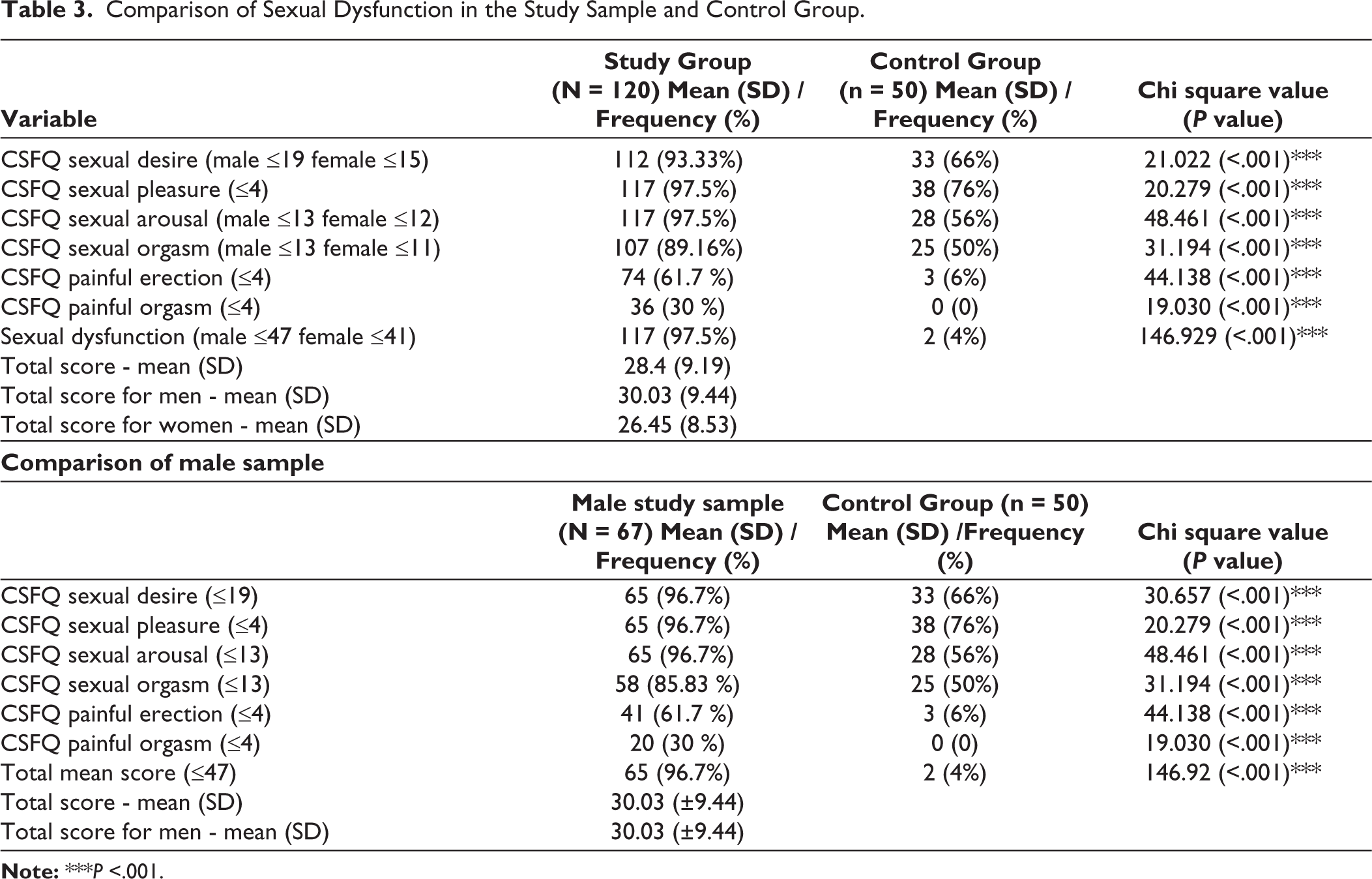
ON CSFQ-14, 97.5% of patients experienced sexual dysfunction, surpassing controls. CSFQ’s suggested cutoff norms revealed prevalence of impaired pleasure/arousal (97.5%) to be the most common dysfunction, followed by reduced desire (93.33%), orgasm dysfunction (89.16%), painful erection (61.7%), and painful orgasm (30%). Compared to healthy subjects, epilepsy patients displayed significantly higher prevalence of sexual dysfunction across all domains (P < .001). As the control group comprised only male patients, to ensure comparability, data of male patients and the control group were analyzed separately and the same differences persisted between the two groups (Table 3).
Comparison of Sexual Dysfunction in the Study Sample and Control Group.
When the impact of psychiatric diagnosis was evaluated on the prevalence of sexual dysfunction, no significant difference was noted on prevalence of sexual dysfunction among those with or without lifetime psychiatric diagnosis. When a similar comparison was done for those with current psychiatric disorder and those without lifetime psychiatric diagnosis, those with current psychiatric diagnosis had significantly higher prevalence of dysfunction in the domains of desire and orgasm (Table 4). Similar differences were noted when those with substance use disorders were excluded from the group with current substance use disorder. When comparison was made for those with current depression and those without lifetime psychiatric diagnosis, those with current depression had significantly higher prevalence of dysfunction in the domains of desire and orgasm. However, when the mean scores were compared, those with psychiatric diagnosis (lifetime and current) had significantly lower CSFQ total score (Table 4).
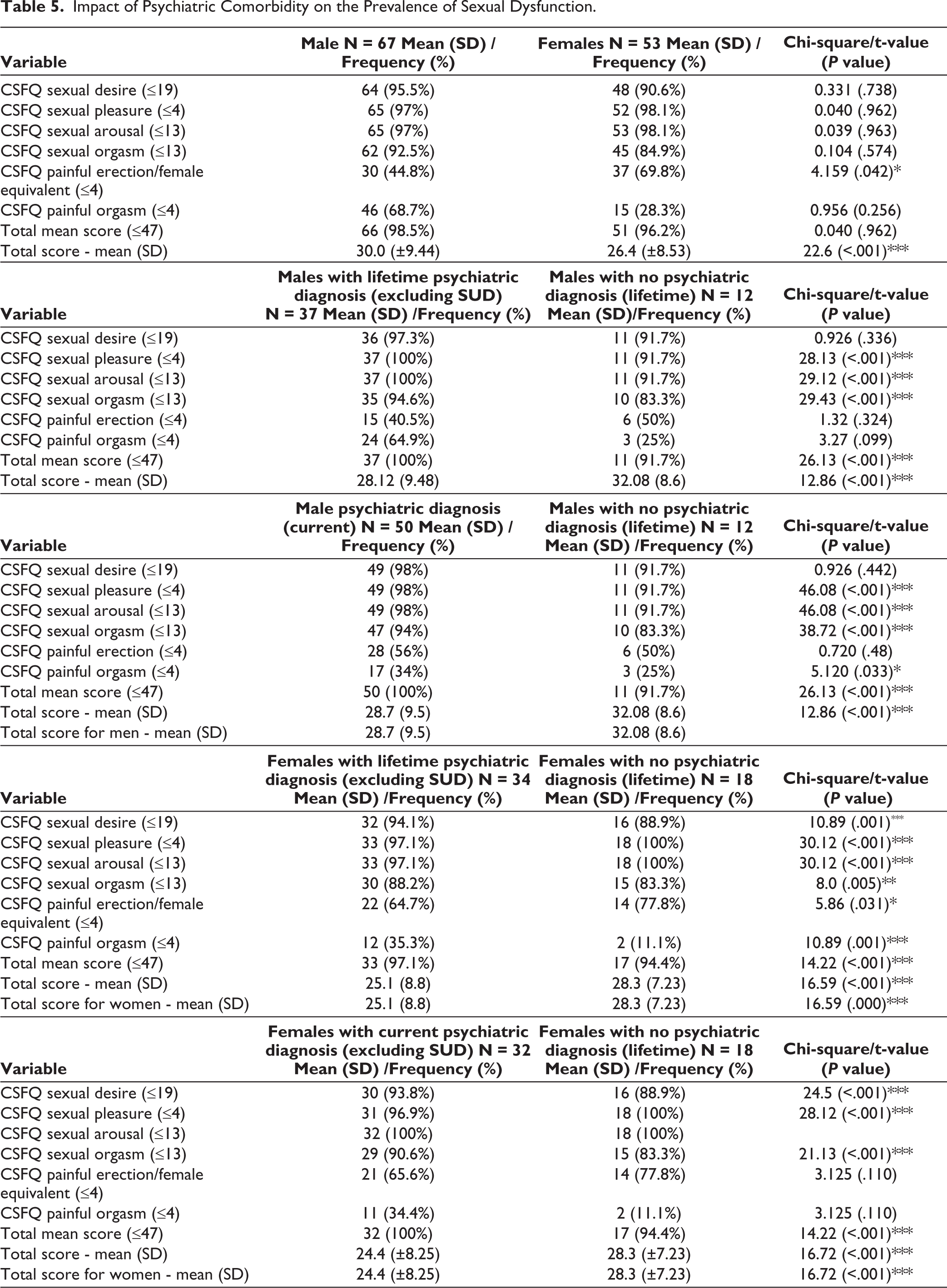
Impact of Psychiatric Comorbidity on the Prevalence of Sexual Dysfunction.
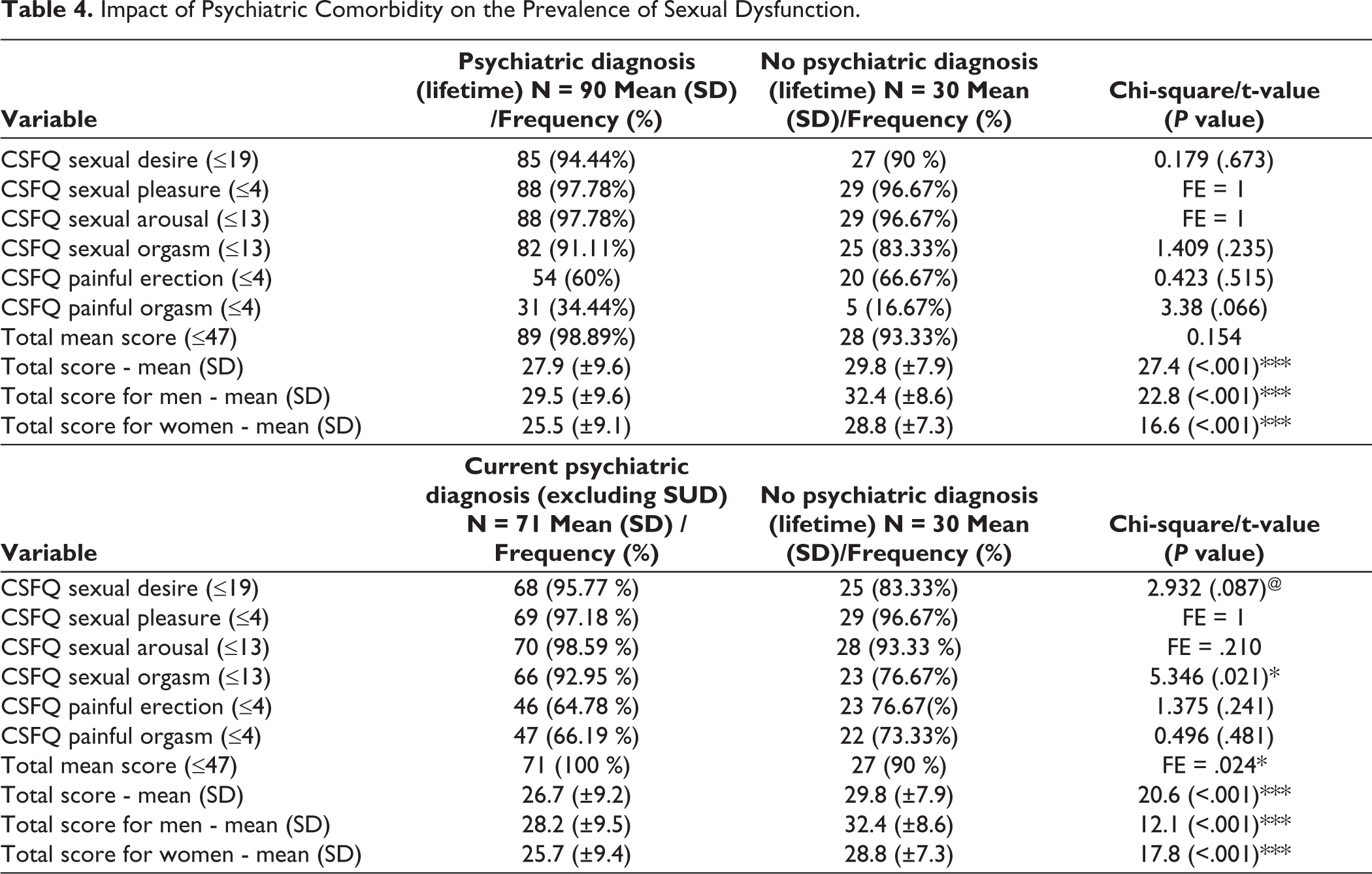
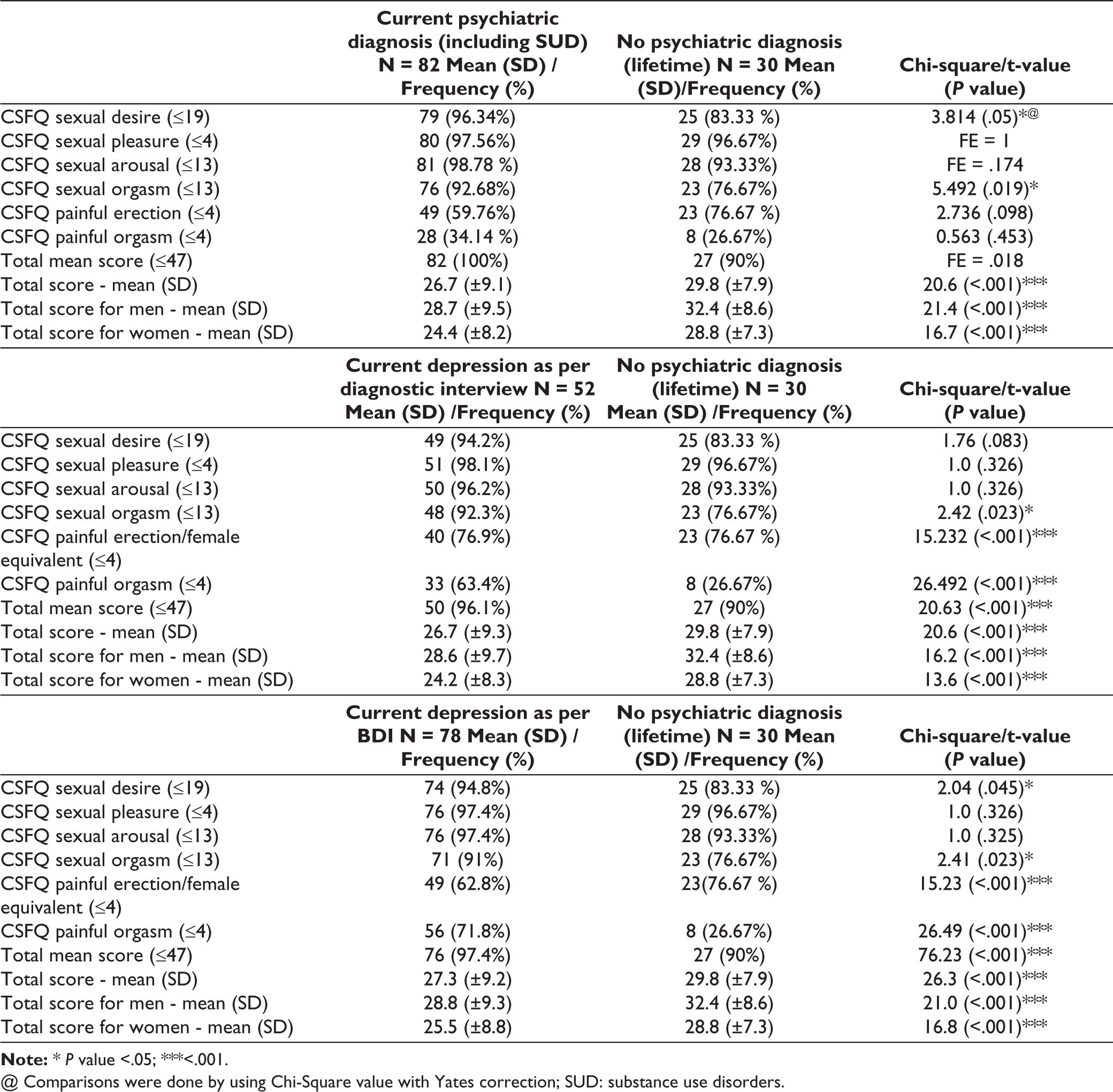
@ Comparisons were done by using Chi-Square value with Yates correction; SUD: substance use disorders.
There was no significant difference between male and females in terms of prevalence of sexual dysfunction, except for significantly higher prevalence of painful erection/female equivalentamong females (Table 5). When sexual dysfunction was evaluated among males and females with and without psychiatric diagnosis, significantly higher prevalence was noted among those with psychiatric disorders for most of the domains of sexual dysfunction (Table 5).
Impact of Psychiatric Comorbidity on the Prevalence of Sexual Dysfunction.
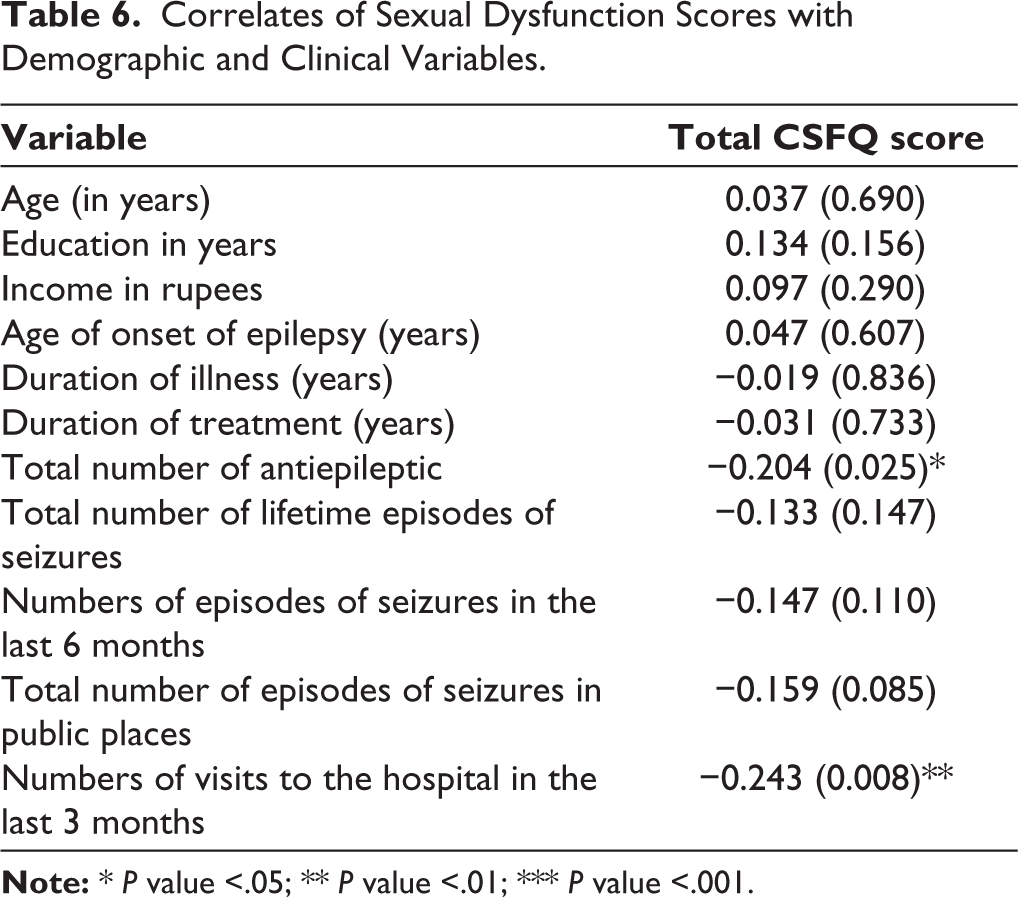
In terms of clinical correlates, significant negative correlation was observed between the total number of antiepileptic medications, the number of visits in the last 3 months, and the total CSFQ score, suggesting an increased count of antiepileptic medications and increased number of visits in the last 3 months (Table 6).
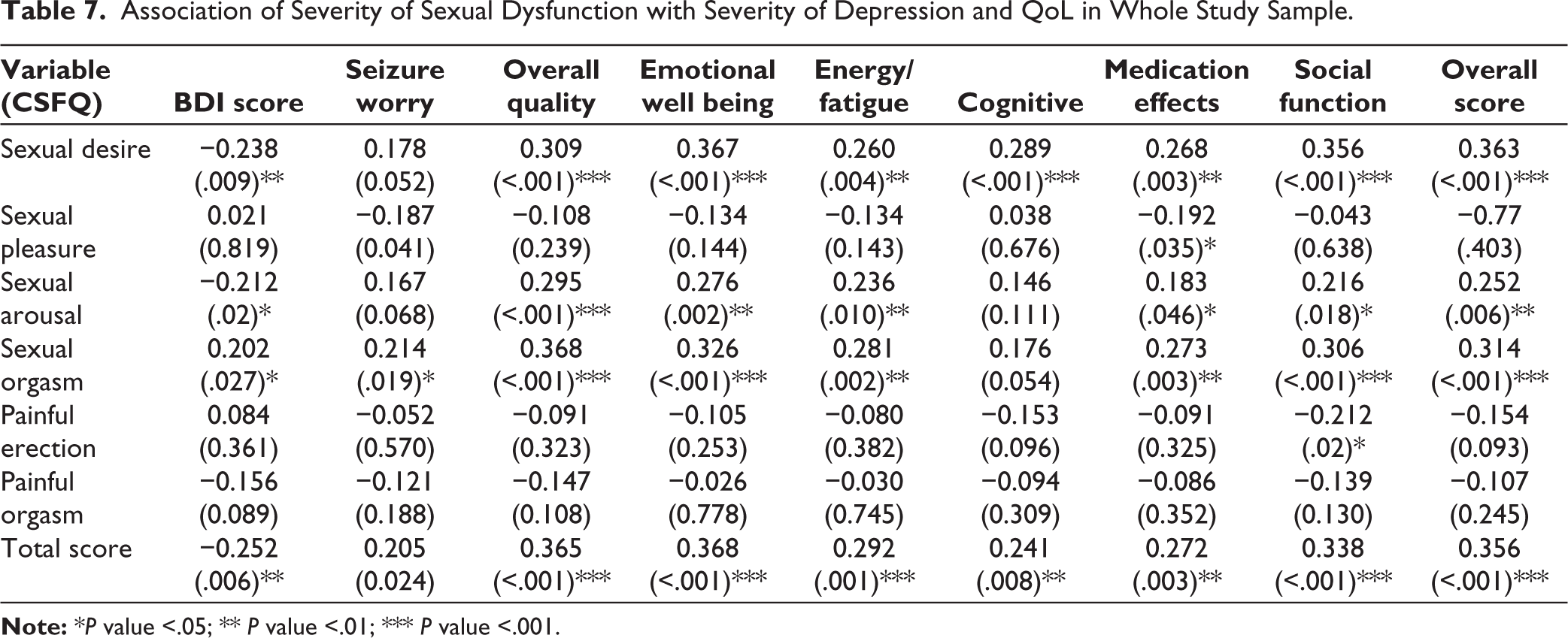
Poor sexual desire and total CSFQ scores was associated with poorer QoL in all the domains except for seizure worry. Sexual orgasm dysfunction was associated with poorer QoL in all the domains. Sexual arousal dysfunction was associated with poorer QoL in all domains except for QoL in cognitive domain. Absence of painful erection/female equivalent was associated with better quality of life in the social function (Table 7). In terms of severity of depression, higher severity of depression was associated with a higher dysfunction in sexual desire, arousal, orgasm, and overall sexual dysfunction (Table 7).
Discussion
The study aimed to explore the impact of epilepsy on sexual functioning. The findings of the present study suggest a high prevalence of sexual dysfunction in individuals with epilepsy, with the majority experiencing impairments in desire, pleasure/arousal, orgasm, painful erection, and painful orgasm. The prevalence of sexual dysfunction in PWE was significantly higher than that reported for a healthy control group in all domains of sexual functioning. Previous studies have reported varying prevalence rates of sexual dysfunction among people with epilepsy. These rates have ranged from 10% to 75% and among men ranged from 3% to 60%. 11 Notably, a recent study that specifically assessed sexual dysfunction in women with epilepsy, that controlled depressive and anxiety disorders, reported that 70% of subjects experienced significantly poorer sexual functioning across multiple domains.17-19 A study, that compared sexual dysfunction in PWE and controls also reported significantly higher prevalence of sexual dysfunction in PWE (women: 75% vs 12%; men: 63% vs 10%). 20 Findings of the present study are also in the similar direction.
Correlates of Sexual Dysfunction Scores with Demographic and Clinical Variables.
Association of Severity of Sexual Dysfunction with Severity of Depression and QoL in Whole Study Sample.
When we compare our findings with these studies, it is apparent that the prevalence of sexual dysfunction in various domains in our study sample was higher than that reported in the existing literature. The high prevalence in the present study could be attributed to the difference in the scale used for assessment in the present study and the earlier studies. In contrast to the previous studies, we relied on CSFQ that allows the participants to compare their functioning with earlier levels of functioning. Hence, it can be said that this may provide a better measure of sexual dysfunction. However, it is also important to note that CSFQ has not been validated in the Indian population and the very high prevalence in the present study could be attributed to the use of cutoffs that have not been validated in India.
This high prevalence of sexual dysfunction in PWE suggest that they should be regularly evaluated for sexual dysfunction during the routine clinical visits. Available literature suggests that sexual dysfunction in PWE could be due to the effect of epilepsy itself or the AEDs on the various hormone levels. However, in the present study we did not evaluate the same. Future studies must build on the findings of the present study, and must attempt to evaluate the possible biological markers for sexual dysfunction.
Previous studies suggest that comorbid depression in PWE influences the prevalence of sexual dysfunction. 21 Considering this, we also evaluated the role of lifetime and current psychiatric morbidity on the prevalence of sexual dysfunction. In general, psychiatric morbidity did not have much influence on the prevalence of sexual dysfunction in various domains except for sexual desire, orgasm, and overall prevalence of sexual dysfunction. However, when the same was evaluated separately for males and females, in general, those with comorbid psychiatric morbidity had higher sexual dysfunction in few of the domains. When the association of severity of depression and sexual dysfunction was evaluated, it was seen that a higher severity of depression was associated with higher severity of sexual dysfunction in sexual desire, arousal, orgasm, and overall sexual dysfunction. Based on our findings, it can be said that sexual dysfunction in PWE is influenced by depression or presence of psychiatric morbidity. Hence, any PWE who reports sexual dysfunction should be carefully evaluated for comorbid psychiatric morbidity in general and depression.
Our study suggests that among PWE, QoL is influenced by sexual dysfunction. Accordingly, any effort directed towards improving the QoL of PWE should focus on evaluation and management of sexual dysfunction too.
The findings of the present study must be interpreted in the light of its limitations. We assessed sexual dysfunction using CSFQ, but it is essential to note that this instrument has not been formally validated for use in the Indian population. The cut-off values applied in our study were adopted from the original authors’ work. Thus, it is essential to exercise caution in drawing definitive conclusions regarding the prevalence of sexual dysfunction observed in our study. Future research endeavors should prioritize the validation of CSFQ in the Indian population to provide a more robust foundation for assessing sexual dysfunction in this context. Further, the study sample was drawn from a clinic attending population, chosen by purposive sampling. This precludes the generalization of the findings to the community samples. The present study did not evaluate the hormonal profile of PWE that could have provided better insight about the association of sexual dysfunction with various hormonal changes. Future studies must attempt to overcome these limitations.
Conclusion
In conclusion, this study shows that sexual dysfunction is highly prevalent in PWE. Our findings emphasize the pervasive nature of sexual dysfunction in this population and the negative impact of the same on various domains of QoL. To improve the holistic care of individuals with epilepsy, healthcare providers must recognize and address the sexual dysfunction in PWE to improve their QoL.
Footnotes
Declaration of Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study received approval from the institute’s ethics committee.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.