
Abstract
We used the 2005–2010 National Health and Nutrition Examination Survey (NHANES), constructed to evaluate health of adults in the United States using consolidated data from interviews and physical exams that were conducted to obtain data for this study. The analysis sample was representative of noninstitutionalized US adults aged 20–59 years. When considering sexual frequency, overall, only female participants with lower sexual frequency were at a higher risk of all-cause death in a dose-response manner with a hazard ratio (HR) of 1.70 (95% CI 1.38–2.10, p trend < .001) during the follow-up period. This relationship was not significant in males. However, when sexual frequency was categorized (<52 times/year vs. ≥52 times/year), the adjusted HR was elevated [2.97 (CI 1.20–7.32, p = .02)] among individuals who had depression and low sexual frequency, but it was close to 1.0 (1.75, CI 0.50–6.07, p = .36) among individuals who had depression and high sexual frequency after adjusting for medical (obesity) and demographic (age, gender, education, and ethnicity) risk factors, indicating a 197% increase in mortality among individuals with low sexual frequency and depression than depression alone. Sexual activity is important for overall cardiovascular health possibly due to reduction of heart rate variability and blood flow increase.
Introduction
Sexual frequency has been demonstrated to be associated with multiple health and relationship outcomes and can be an important indicator of sexual and overall health and well-being. Muse et al. 1 demonstrated a correlation between sexual frequency and well-being outcomes that was curvilinear when the frequency was measured as 1 or more versus less than 1 time per week and when relationship duration along with gender and age were considered. Frequencies greater than once per week no longer produced greater well-being outcomes. Kashdan et al. 2 conducted a study using a daily diary approach to test the relationships between sexual activity, positive and negative affect, and meaning in life. They reported a positive relationship between sexual activity on a given day followed by a boost in mood and positive meaning in life the following day. Of the covariates tested (gender, relationship status, relationship closeness, and relationship length), greater relationship closeness was the most likely variable to be enhanced the next day. The authors found no corresponding negative impact on the day following a day without sexual activity.
Another research study focused on the relationship between sexual activity and health outcomes was conducted prior to and since the advent of the COVID-19 pandemic. Jackson et al. 3 used data from the English Longitudinal Study of Ageing to test relationships between sexual activity (including frequency) and illness (including diseases of the vascular system and cancer). They reported that decreased sexual activity was related to adverse health outcomes for both men and women, and they were the first to report a relationship between erectile dysfunction and cancer in older men. More recently, the relationship between sexual activity and intrapsychic, relational, and sexual health during the COVID-19 pandemic was tested. 4 The authors reported that both males and females with higher levels of sexual functioning were less likely to be depressed or anxious despite the difficulties related to COVID-19. The authors in both of these studies used definitions of sexual activity that focused on erectile dysfunction and orgasmic intensity rather than actual frequency counts or defined frequency as having sex in the past two months (yes or no).
Cao and colleagues 5 examined the US National Health and Nutrition Examination Survey from 2005 to 2016 and the National Health and Nutrition Examination Survey 2005–2014 Linked Mortality File (through December 31, 2015) to determine associations between sexual frequency and all-cause, cardiovascular disease and cancer mortality. The authors reported links between increased sexual frequency and decreases in all measures of mortality in their study. In our study we used the same data set to test relationships between sexual frequency and depression in addition to all-cause mortality expanding on the work of Cao and colleagues. 5
There is mounting interest in understanding how precisely sexual health affects overall health. Sexuality can be considered “the dynamic outcome of physical capacity, motivation, attitudes, opportunity for partnership, and sexual conduct” 6 and is important to understand because sex can bring many benefits, including increased happiness, well-being, and quality of life 7 encompassing all sexual orientations. Since physical and mental comorbidities coincide to impact overall health, identifying any association in the biopsychosocial context would be beneficial in both public health and clinical settings.
Fundamental Cause Theory
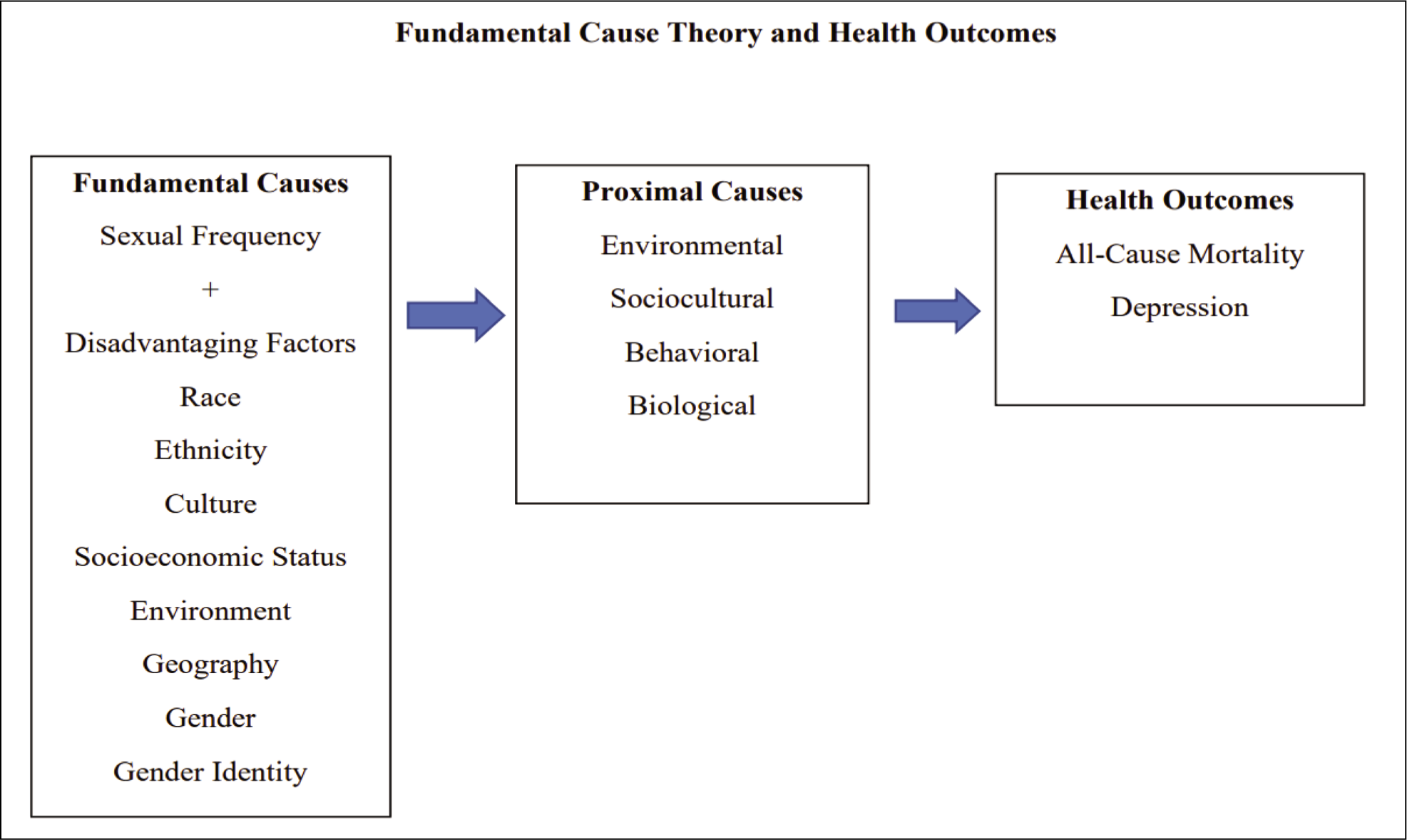
Theories are important to ground the research and potential connection between sexual health and overall mortality. The theory of fundamental causes 8 contributes to our inquiry (Figure 1). Through this theory, authors attempt to explain why social inequalities in health continue even with medical innovation and disease elimination. 9 This theory includes multiple concepts showing the importance of social factors in disease causation. The first concept is contextualizing fundamental aspects of individually based factors to predict unequal individual characteristics of a disease. For this concept we are testing depression. The second concept is the fundamental causes or determination of social conditions such as socioeconomic status, under which risk factors are related to the disease. 8 In our model, the potential moderating variables are represented as proximal determinants with health conditions as the final outcomes. In our model, sexual frequency was added as a moderating variable. This theory stems from Lieberson’s concept of basic causes developed in 1985, who proposed that changes in basic causes (factors responsible for generating a particular outcome) create a change in the outcome. 8
Fundamental Cause Theory and Health Outcomes in Sexual Health.
Sexual Health and Chronic Disease
Due to various physiological mechanisms, chronic diseases negatively affect sexual health. For instance, it is well known that chronic and long-standing diabetes leads to neuropathy and sexual dysfunction.10,11 Multiple sclerosis and other autoimmune disorders negatively affect the autonomic nervous system, resulting in sexual comorbidities.12,13 Due to the multisystemic effect of chronic diseases, the effects are experienced over a long period of time with multiple periods of remission. Sexual dysfunction can be an indicator of individual experience especially during the latency period of the disease when other indicators may appear normal.
Although the connections between physical health, social determinants of health, mental health, and poor health are well known, there is a paucity of research regarding the connection between sexual health and long-term mortality outcomes. In this study, we explored the long-term connections between depression and all-cause mortality and whether sexual frequency modifies this relationship. Furthermore, we assessed whether after controlling for physical health (i.e., obesity), age, ethnicity, and education, low sexual frequency independently led to increased five-year all-cause mortality. Furthermore, we created a revised version of the theory of fundamental causes as the theoretical framework to guide our study.
Methods
Study Participants
We used the 2005–2010 National Health and Nutrition Examination Survey (NHANES), a program of the National Center for Health Statistics (NCHS), which was constructed to evaluate the health of adults in the United States using consolidated data from interviews and physical exams, to obtain data for this study. The analysis sample is representative of noninstitutionalized US adults aged between 20 and 59 years. The procedures and protocols for NHANES are approved by the NCHS before data collection. Data is available for public use through the CDC website. We received additional ethical approval through the Walden University Institutional Review Board for data analysis using publicly available files.
All-cause Mortality
Vital status was determined using the Continuous NHANES Public-use Linked Mortality File, which provides vital status follow-up data in person—months from the date of NHANES survey participation through the date of death or December 31, 2015. Mortality was ascertained by the NCHS through a probabilistic match between NHANES participants and National Death Index (NDI) death certificate records. This probabilistic match approach is a modification of the probabilistic match approaches developed by Fellegi and Sunter 14 and Rogot et al. 15 Each NDI possible match record is assigned a probabilistic match score. The probabilistic match score is the sum of the weights assigned to each of the identifying data items used in the NDI record match, where the weights reflect the degree of agreement between the information on the submission record and the NDI death record. Participants who were not matched with death records were considered to be alive through the follow-up period.
Measures: Depression
The Patient Health Questionnaire 9 (PHQ-9) is a nine-item depression screening instrument that asks about the frequency of symptoms of depression over the past two weeks. Total PHQ-9 scores range from 0 to 27 and are categorized as “none or minimum” (0–4), “mild” (5–9), “moderate” (10–14), “moderately severe” (15–19), and “severe” (20–27) for depression severity. 16 In this study, we combined scores 10–27 (“moderately severe or severe”) to improve precision of estimates. We defined PHQ-9 total scores ≥ 10 as depression since this is consistent with clinically relevant depression. This is consistent with depression process/outcome performance measures recommended by the National Quality Forum. PHQ-9 score ≥10 has shown a sensitivity of 88% and a specificity of 88% for major depression.
Measures: Sexual Frequency
Sexual frequency can be considered a proxy measure for overall sexual health. The frequency of sexual activities in the NHANES data set was self-reported during the in-person interview. 17 Participants were asked, “In the past 12 months, about how many times have you had vaginal or anal sex?” with options of never, once, 2–11 times, 12–51 times, 52–103 times, 104–364 times, and 365 times or more in the past 12 months. For analysis of the association between sexual activities and mortality outcomes, we categorized participants into <52 times/year and ≥52 times/year. We used these cutoffs because previous authors reported that the average frequency of sexual activity is 54 times/year or about once a week among the US adults, which also approximated the median values in the present study population.
Measures: Obesity
Obesity data from the NHANES data set was subdivided into four categories according to body mass index (BMI) derived from measured height and weight. The categories were as follows: participants with BMI < 25 were considered normal weight; participants with BMI = 25–29 were overweight; participants with BMI = 30–39.9 were considered as obese; and participants with BMI > 40 were considered severely obese. For the multivariate models, obesity was dichotomized and considered present for BMI ≥ 30 and considered absent for the rest.18–20
Measures: Additional Covariates
NHANES demographics were also assessed as covariates. Age and ethnicity were demographic variables. Ethnicity was divided into “Non-Hispanic White,” “Non-Hispanic Black,” “Hispanic,” and “Asian.” Finally, the education-level data was subdivided into a trichotomous indicator as “completing some High School” versus “High School graduate” versus “Some College or above.”
Statistical Analysis
We weighted demographic and environmental variables to approximate distributions in the USA by using the provided sample weights to account for oversampling of young children, older people, non-Hispanic Black individuals, and individuals of Mexican-American ethnic origin in the NHANES survey. We described continuous variables as mean ± standard deviation (SD). We assessed normal distributions of values by using the Shapiro–Wilk test. Categorical variables were expressed as percentage values and analyzed using chi-square testing. Analysis was performed using Cox proportional hazards, and separate models for sexual frequency versus all-cause mortality were run by depression status. Additionally, complex sample multiple Cox regression models were used to examine the potential effect of various sexual frequency-level differences after adjusting for sociodemographic and health factors, estimating variances using the Taylor series linearization method. We also adjusted for variables recognized widely as potential confounders for depression. Statistical analyses were conducted using the SAS System for Windows (release 9.3; SAS Institute Inc., Cary, NC) and SUDAAN (release 9.0; Research Triangle Institute, Research Triangle Park, NC). All analyses included sample weights that accounted for the unequal probabilities of selection and nonresponse. All variance calculations incorporated the sample weights and accounted for the complex sample design using Taylor series linearization. All significance tests were two sided using p < .05 as the level of statistical significance.
Results
Demographic Characteristics
A total of 14,542 study participants aged 20 years or older were included for analysis in this study. Table 1 provides the data for the distribution of the demographic characteristics, lifestyle behaviors, and chronic diseases among the study participants stratified by depression status using bivariate analysis. The weighted prevalence of depression in the US population ages between 20 and 59 years was 6.0% (4.8%–7.6%). The average age of the participants within the sample was 46.1 years (S.E ± 0.35) with a statistically significant difference between high sexual frequency versus low sexual frequency (35.7 vs. 40.0 years, p < .001), where individuals with high sexual frequency were younger in age. There were statistically significant differences between sexual frequency status based on age, race/ethnicity, education level, poverty–income ratio, smoking status, and chronic diseases. Among the individuals with low sexual frequency, participants were more likely to have elevated CRP (9.6%), were never smokers (54.3%), with at least some college or more (65.5%), and were people with depression (6.6%) compared to their counterparts who were not deemed to have low sexual frequency. Approximately 9.3% of low sexual frequency participants were non-Hispanic Black compared to 11.0% of their high sexual frequency counterparts. This trend is opposite to the non-Hispanic White population and Hispanic population.
Characteristics of Study Participants Stratified by Sexual Frequency.
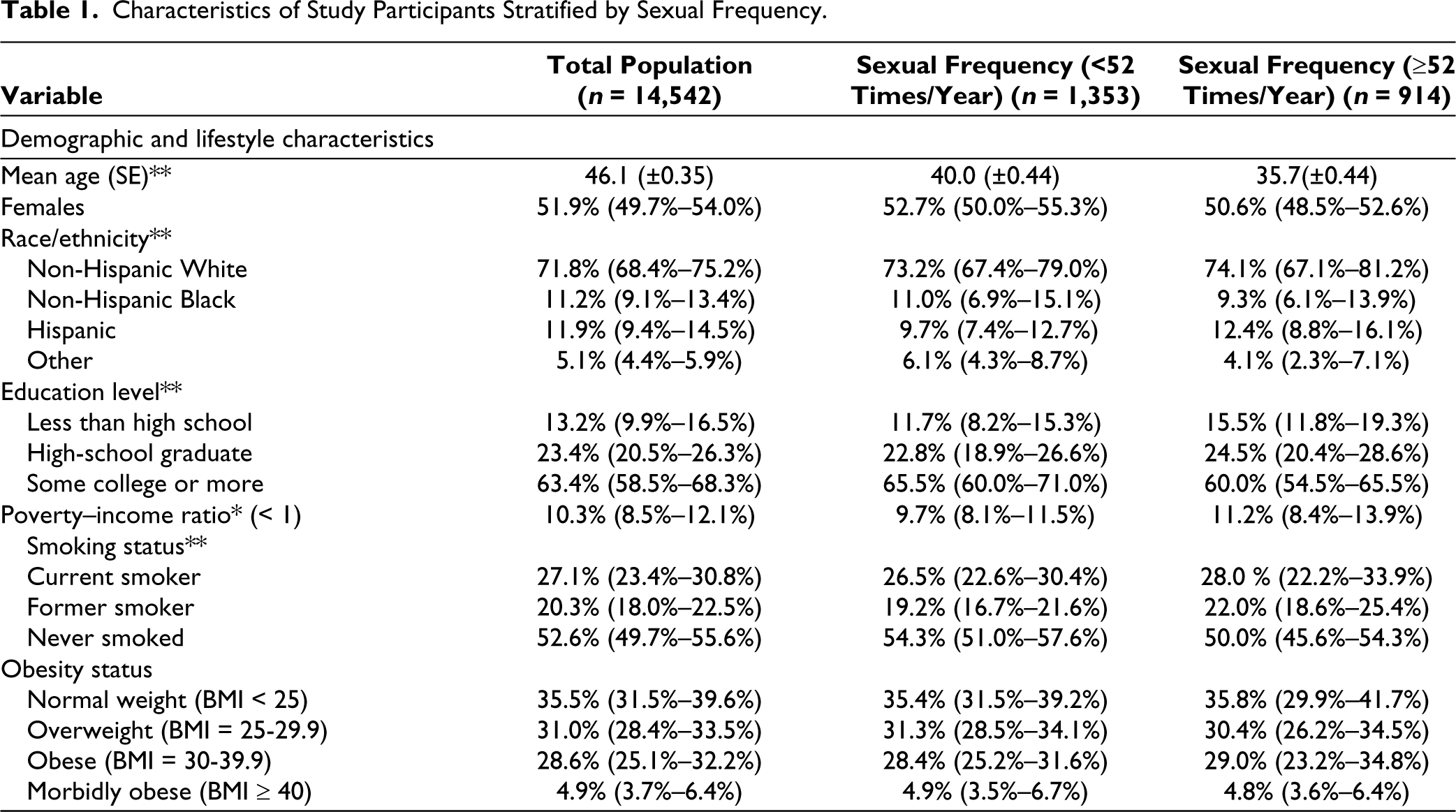
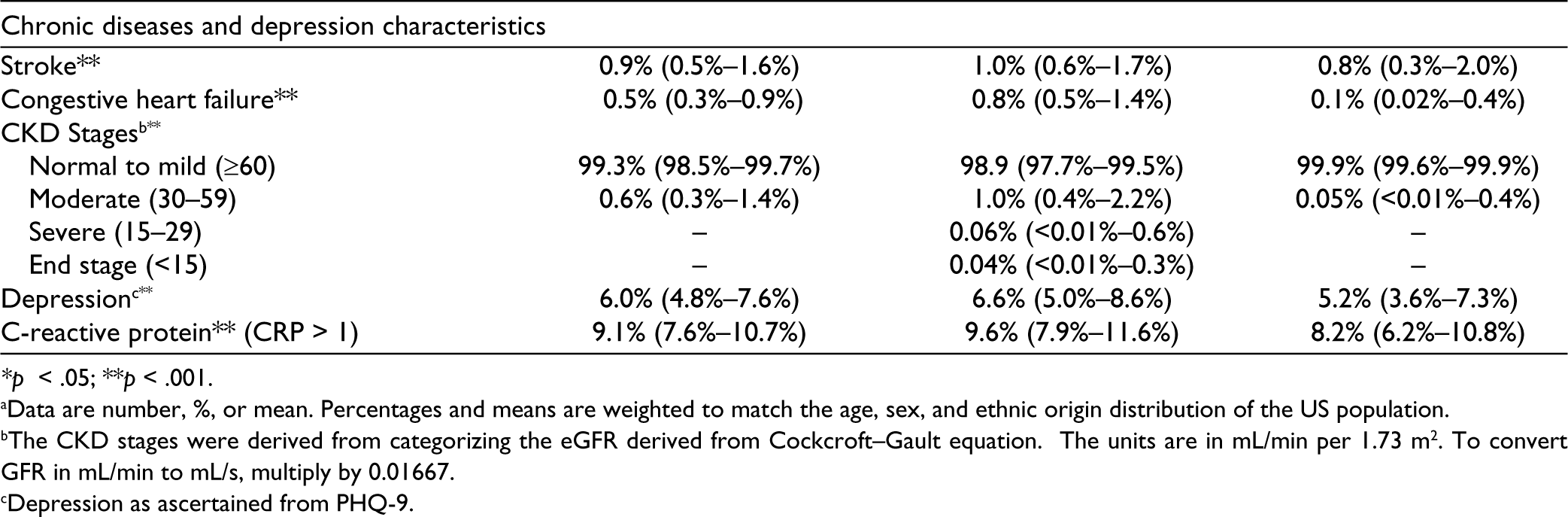
*p < .05; **p < .001.
aData are number, %, or mean. Percentages and means are weighted to match the age, sex, and ethnic origin distribution of the US population.
bThe CKD stages were derived from categorizing the eGFR derived from Cockcroft–Gault equation. The units are in mL/min per 1.73 m2. To convert GFR in mL/min to mL/s, multiply by 0.01667.
cDepression as ascertained from PHQ-9.
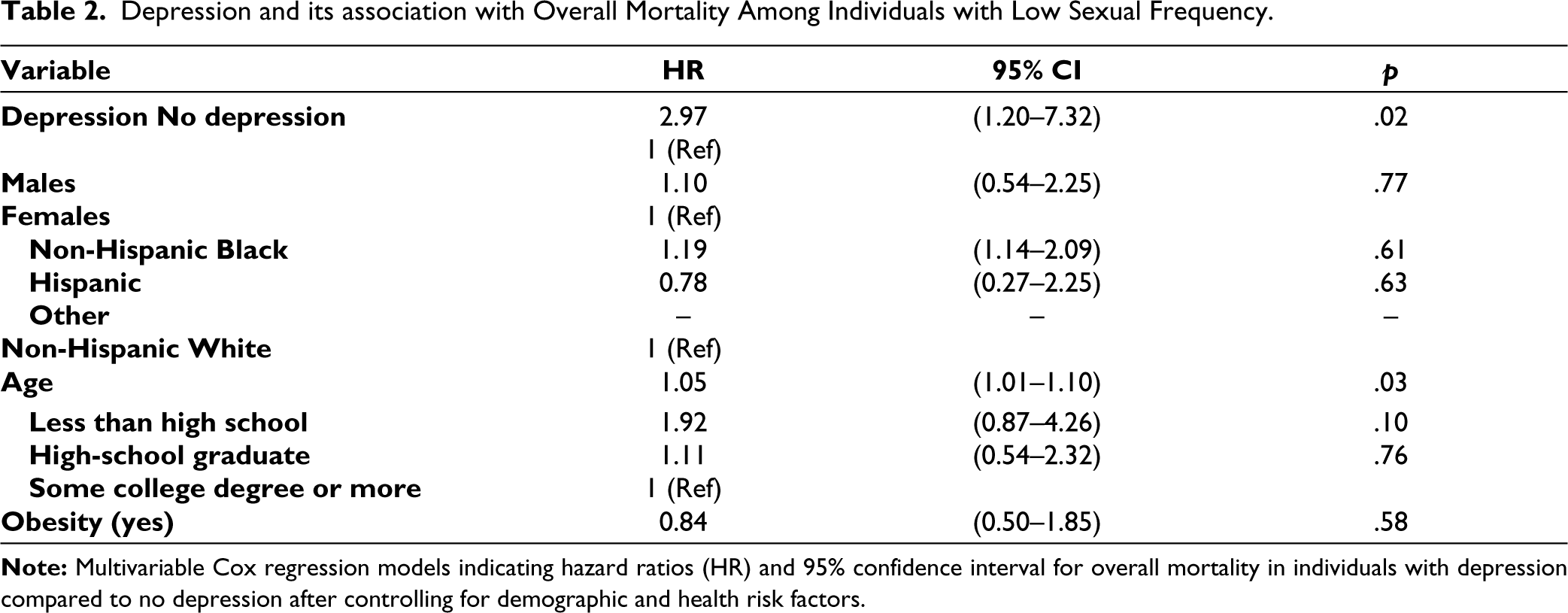
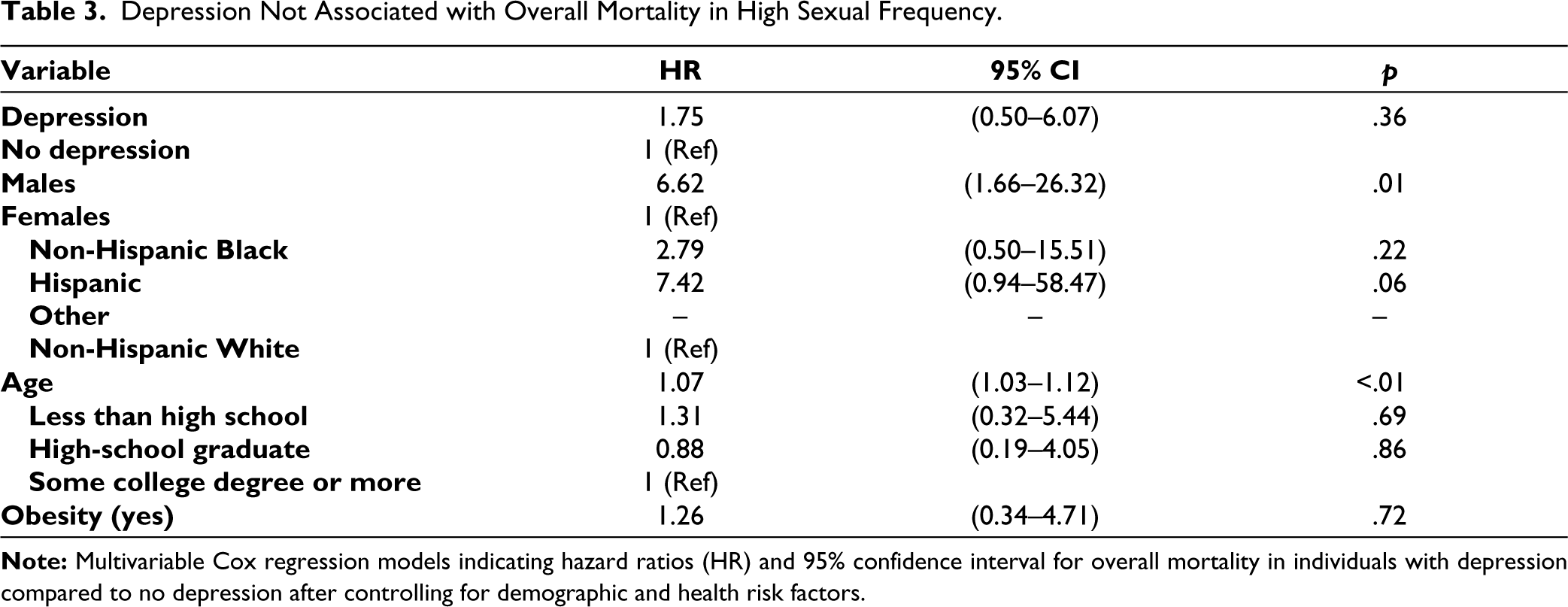
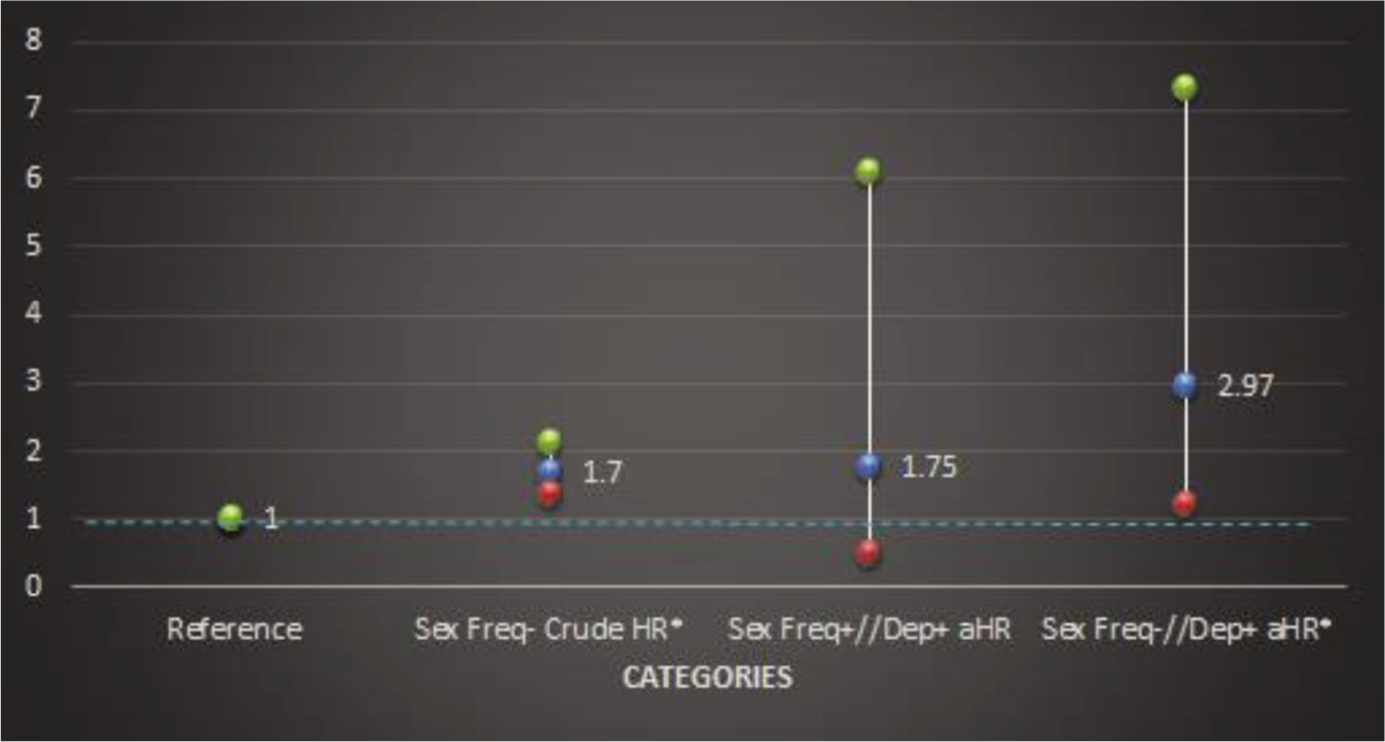
Out of the total respondents (N = 2,267), 94.4% (95% CI, 83.1%–99.8%) US adults aged 20–59 years engaged in sexual activity ≥12 times/year (monthly), and only 38.4% (95% CI, 33.5%–43.4%) of them engaged in sexual activity ≥52 times/year (weekly). Overall, only female participants with lower sexual frequency were at a higher risk of all-cause death in a dose-response manner with the hazard ratio (HR) of 1.70 (95% CI 1.38–2.10, p trend < .001) during the follow-up period. However, when sexual frequency was categorized (<52 times/year vs. ≥52 times/year), the adjusted HR was elevated [2.97 (CI 1.20–7.32, p = .02)] among individuals who had depression and low sexual frequency but close to 1.0 (1.75 CI 0.50–6.07, p = .36) among individuals who had depression and high sexual frequency after adjusting for medical (obesity) and demographic (age, gender, education, and ethnicity) risk factors, as seen in Table 2 and Figure 2, indicating a 197% increase in mortality among individuals with low sexual frequency and depression than depression alone. This indicates a (197% versus 75% (as seen in Table 3) higher probability of mortality among those individuals with depression and low sexual frequency rather than depression and high sexual frequency.
Depression and its association with Overall Mortality Among Individuals with Low Sexual Frequency.
Depression Not Associated with Overall Mortality in High Sexual Frequency.
Discussion
A unique finding of this study is the long-term effect of low sexual frequency on premature mortality after long follow-up in a large-scale nationally representative population. Without adjusting for multiple causal factors for premature mortality (e.g., demographic and mental health comorbidities), low sexual frequency was associated with 70% higher probability of mortality compared to those who had higher sexual frequency. After adjusting for multiple demographic factors, physician and mental health risk factors, the probability of mortality in low sexual frequency remained 46% higher compared to those who had high sexual frequency. The findings are similar to a smaller-scale study conducted in Israel, where it was found that despite confounders, sexual activity after a myocardial infarction was inversely related to mortality. 21 This finding warrants additional research and investigation to ascertain causal pathways for premature mortality in individuals with low sexual frequency. While our adjustment for well-known modifiable and demographic health risk factors showed a reduction in the likelihood of mortality among individuals with low sexual frequency, the reduction was modest.
Sexual Expression and Overall health
Sexual expression, which is quantitatively measured through sexual frequency, is an essential component of both physical and mental health. Physical health and disease directly affect a person’s capacity for sexual expression. 22 Using findings from our study, we can infer that sexual activity, broadly defined, may ameliorate loss of function that can occur with age and the progression of disease. 6 Likewise, loss of sexuality is the hallmark of some mental states, such as depression, and in turn, satisfying sexual relationships can buffer the effects of everyday stressors. 22 Some components of sexuality and sexual expression may be more important than others in each of these mechanisms.
Understanding that sexual health is an indicator of overall health is important. Equally as important is to understand that the treatments that are present may also lead to lower sexual frequency, which could then, in turn, lead to more depression. So, in effect, from a pathophysiological perspective, once an individual has depression, the condition alone may lead to lower sexual frequency, in addition to the treatment regimen used to address the condition.
Sexual Health and Depression
Another unique finding in our study was the modifying relationship of sexual frequency on the impact of depression on overall health. Depression has been shown to be strongly connected to loss of interest. This would partially explain why when along with depression, when there is also low sexual activity, this is associated with increased overall mortality. There is an increase in overall mortality when there are mental health risk factors along with low sexual activity than if the person had depression alone. Additionally, many of the anti-depressants, along with the first-line treatments, such as selective serotonin uptake inhibitors (SSRIs), are effective 40%–60% of the time but many times require multiple medications for proper treatment. 23 In fact, SSRIs are associated with decreased libido, problems with arousal and erection, and delayed or absent orgasm.24-26 This, in turn, would negatively affect sexual frequency and, according to our study, is associated with a stronger effect on the effect of depression on overall health. The strong connection between libido and depression is further affected by the social determinants of health.
Healthcare practitioners take a strategic approach to manage depression. Our findings suggest that sexual health be specifically considered when thinking about mental health. Usually, if one pharmacotherapeutic agent does not work or has sexual side effects, then psychiatrists switch to another medication in the same class. 26 Then, typically, they would find another class that may be more effective or may cause less side effects. However, this treatment titration requires close patient–physician communication, which is connected to health and social determinants of sexual health.
Social Determinants of Sexual Health
Our findings demonstrate the need for improved overall sexual health. However, the gaps in the US healthcare system lead to decreased sexual activity and overall poor sexual health due to multiple reasons. We argue that sexual health should be included as an important component of social determinants of health. Healthcare practitioners use several models to assess for sexual health. The Centers for Disease Control and Prevention have established the 5-P model to guide sexual history-taking in a systematic manner. The five P’s stand for partners, practices, prevention of pregnancy, protection from STDs, and past history of STDs. 27 Another research includes another P for pleasure in order to get a complete understanding of overall sexual health. However, as part of this questionnaire, depression should be included due to our finding that depression independently is associated with sexual activity, which would then affect the findings of sexual history-taking. Sexual behavior and frequency are a complex interplay of societal and cultural factors, sexual behavior and attitudes, biological risk and genetic predisposition, and mental and physical illness, all combining to influence sexual health.
Socioeconomic Status as a Social Determinant of Sexual Health
Our article primarily focuses on sexual behavior, which is an important part of reproductive rights. Reproductive rights include the recognition that people should be able to decide if, when, and how often they want to reproduce. 28 This choice is more difficult among historically marginalized women and should be effectively addressed as it pertains to sexual frequency. For example, having access to all methods of birth control, regardless of socioeconomic status, is part of ensuring adequate reproductive rights.
Furthermore, people should have information and access to safe, effective, affordable methods of family planning in order to maintain similar amounts of sexual frequency. In many ways, not being able to get a day off work to go to the clinic or not being able to receive childcare can lead to poor sexual health. Additionally, lack of transportation and not being able to get to the clinic combined with low literacy levels can lead to less reproductive choices and gaps in family planning and potentially affect sexual frequency and behavior, especially as has been established in the Appalachia region in the United States by researchers. 29 Many times, there are forms of birth control that all types of insurance may not cover if the individual happens to have insurance. There are many segments of the population that remain uninsured within the United States. Finally, not being able to leave an abusive relationship and being financially dependent can lead to both depression and lower sexual frequency.
Financial distress is a major factor in understanding both sexual frequency and depression. According to one study, it was found that individuals living in 300% of the federal poverty level or below was connected to higher rates of depression. 30 Treatment for major depressive disorders alone costs Americans $300 million dollars. 31 For instance, in a major study by the Planned Parenthood Federation of America, out of the 1,627 respondents, two-thirds lacked basic access to food, medical care, housing, and heating. 32 However, what was even more striking was that only half were willing to talk to their healthcare provider about these concerns. This would be associated with more mental stress and potentially affect sexual frequency and behavior overall. It is important to align payment structures with the needs of the women seeking sexual and reproductive health. This will allow for the mitigation of needs and better sexual health and overall health.
Education as a Social Determinant of Sexual Health
Both on a patient level and on a population level, it is important to take education into consideration in sexual health and behavior. The individual may not have the knowledge to maintain proper sexual health and well-being. While sexual frequency is only one aspect of sexual health, it is also important to note that sexual behavior, attitudes, and sexually transmitted infections are interconnected with sexual frequency. If a patient does not have access to birth control, then the chances of pregnancy are higher, in turn making the family more vulnerable to economic instability. While according to our findings, higher education was shown to be associated with low sexual frequency, the advantage is that higher education is associated with later entry into marriage, smaller families, more effective spacing and planning of childbirth, and more acceptability of contraception. This, in turn, can lead to less depression and indirectly higher sexual frequency. Additionally, women with a bachelor’s degree have access to higher reproductive health services than those who do not. 33
Additionally, factors like social isolation can play a role in those linguistic barriers, especially if a migrant work or another immigrant may feel isolated within their community. If they are outside the healthcare system, then they may not be able to access the full host of services as it pertains to maintaining adequate sexual health and potentially deleteriously affecting sexual frequency. It can be surmised that through low sexual frequency, social isolation can lead to increased overall mortality. This also means that during contraceptive counseling, the patient’s perception and awareness must be inquired about as well and considered, especially as it pertains to literacy. On a population level, perception and awareness can be easily assessed through a questionnaire introducing the knowledge, attitudes, and practice structure that is an approach taken to understand more about any public health problem. Understanding the problem of sexual frequency stemming from the actual issues with the sexual response cycle is important to note. For instance, one study found that premature ejaculation and erectile dysfunction are the most common types of disorder leading to distress. 34 This can then be associated with more depression. There are multiple ways that individuals with problems in the sexual response cycle can address the issue. 35 For instance, a large three-wave longitudinal study found that women’s sex activity improved with the use of pornographic viewing versus males’ performance deteriorated.
While our analysis was only limited to non-institutionalized populations, the sexual health of incarcerated individuals is also important to consider. About 42% of women identify as sexual minorities among women. 36 Sexual minorities have three times the rate of incarceration as non-sexual minorities. Sexual assault is common in prison as well, and condoms are not widely available. Regarding frequency, 64% of sexually active inmates have had sexual relationships at least once every 15 days. 37 Therefore, considering the sexual frequency of prison inmates is also important. The stigma behind condom availability leads to the lack of availability of this important commodity in prison. Additionally, prison sexuality is different due to the choices of abstinence, auto-eroticism, true homosexuality, situational homosexuality, and sexual violence. This also negatively affects sexual health. Undeniably, social isolation plays a critical role in depression and loneliness. 38 While the authors studied this social isolation in the context of COVID-19, social isolation is connected in complex ways to both depression and sexual frequency.
Limitations
We understand that while this study provides insights into the complex interplay between mental health, sexual health, and overall mortality, there are other aspects of sexual behavior that were not measured. For instance, the sexual satisfaction subscale is a part of the Multidimensional Sexual Self-concept Questionnaire (MSSCQ) and can provide more detailed insights into what type of specific sexual activities they engage in along with sexual frequency. 39 Providing more specificity can provide more insights, and also studying specific disease-related mortality can establish specifically whether low sexual frequency is associated with specific disease conditions.
Conclusion
In an ethnically diverse population, we found that low sexual frequency can lead to three times increased overall mortality, even after controlling for health and demographic factors. Consistent with our findings, sexual activity is important for overall cardiovascular health possibly due to reduction of heart rate variability and blood flow increase. Public health interventions should be designed taking into consideration sexual health.
Another unique finding from our study was that there was a combination effects that were experienced between sexual frequency and social variables. For instance, in the regression model with high sexual frequency, males were six times more likely to experience increased mortality than females. This shows that sexual frequency interacts with gender to increase mortality. The combination effect may exert an additional effect than just the sum of the individual effects from gender or sexual frequency alone. The implications are that by addressing sexual frequency, other health disparities can be addressed more directly.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
We received additional ethical approval through the Walden University Institutional Review Board for data analysis using publicly available files.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The National Center for health statistics ethical review board approved all NHANES protocols, and written informed consent was obtained from all participant.