
Abstract
Objectives:
Alcohol misuse and depression are commonly co-occurring conditions. To date, no review has examined the most efficacious treatment model for psychosocial treatment of co-occurring alcohol misuse and depression. This systematic review determined the: (i) methodological quality of publications examining psychosocial treatment of co-occurring alcohol misuse and depression using a sequential, parallel or integrated treatment model; and (ii) effectiveness of each dual treatment model compared to single treatment for those with co-occurring alcohol misuse and depression.
Methods:
PubMed, Medline and PsycInfo databases were searched for studies which were included if they involved treatment for alcohol misuse and depression and could be classified into one of the three treatment models. Included studies were assessed using the Cochrane’s Effective Practice and Organisation of Care risk of bias criteria. Relevant study characteristics and outcomes were extracted and are presented in a narrative review format.
Results:
Seven studies met inclusion criteria. None were categorised as low risk on the risk of bias criteria. No studies examined a sequential model of treatment, three examined a parallel model and four examined an integrated model of dual-focussed treatment. The studies examining the parallel model and two out of four studies examining the effectiveness of an integrated model demonstrated greater improvement for alcohol or depression outcomes compared to control conditions.
Conclusion:
Evidence for the psychosocial treatment of co-occurring alcohol misuse and depression is limited to a handful of studies. The evidence has several methodological limitations, which impact the interpretation of the findings. Therefore, while international guidelines recommend integrated dual-focussed treatment for co-occurring conditions, there is little evidence supporting the superiority of this treatment format for co-occurring alcohol misuse and depression. High-quality research demonstrating improvements in patient outcomes is required to ensure recommendations for clinical practice are based on strong empirical evidence.
Introduction
Prevalence and impact of co-occurring alcohol misuse and depression
Rates of concurrent mental illness are high for individuals with conditions related to alcohol misuse, estimated to range from 10% to 60% (Riper et al., 2014), with depression reported as one of the most prevalent co-occurring conditions (Lai et al., 2015). The term ‘alcohol misuse’ will be used in this paper to encompass all alcohol-related disorders, including excessive or risky consumption and alcohol use disorders such as abuse or dependence (Bradley et al., 2007). Recent meta-analytic data indicated major depression to be 2.4 times as likely among those with alcohol misuse compared to the general population (Lai et al., 2015). Compared to those with only one condition, individuals with co-occurring alcohol misuse and depression experience increased symptom severity, and poorer mental and social functioning (Burns et al., 2005; Sullivan et al., 2005). In addition, co-occurring alcohol misuse and depression has been associated with poor treatment outcomes, including higher rates of alcohol consumption after treatment when compared to those with alcohol misuse alone (Burns et al., 2005). Due to the high prevalence and burden of co-occurring alcohol misuse and depression, as well as the unique interaction between these two conditions, it is important to determine the most effective treatment approach.
Single- versus dual-focussed psychosocial treatment of co-occurring alcohol misuse and depression
There is substantial evidence to support the effectiveness of psychosocial treatment of alcohol misuse alone (Magill and Ray, 2009; Miller and Wilbourne, 2002) and depression alone (Cuijpers et al., 2008, 2011, 2013). However, considering the best approach to psychosocial treatment when these conditions co-occur may assist in improving treatment outcomes. There are two key approaches to treating co-occurring alcohol misuse and depression: single- or dual-focussed treatment. Single-focussed treatment is based on the assumption that treating one condition will improve the other. Often for individuals seeking drug and alcohol treatment, depressive symptoms subside after alcohol misuse treatment, which supports this treatment approach (Boden and Fergusson, 2011; Schuckit, 2006). However, for many patients, depressive symptoms remain after treatment and these symptoms can increase the likelihood of relapse (Nunes et al., 2006). As a result, there has been a push towards the treatment of both conditions, regardless of the historical onset of condition symptoms. Hobbs et al. (2011) conducted a meta-analysis examining supplemental depression and anxiety treatment for individuals seeking treatment for alcohol misuse. They found improvements in alcohol misuse and depression outcomes for those receiving dual treatment compared to those treated for alcohol misuse alone (Hobbs et al., 2011), supporting a dual-focussed treatment approach. This analysis, however, included nine studies for depression, of which only one study had a psychosocial intervention aspect while the others tested drug treatments. The effectiveness of dual-focussed psychosocial treatment compared to single-focussed therefore remains unclear.
Models of dual-focussed treatments
International clinical guidelines from the United Kingdom (Department of Health (England) and the Devolved Administrations, 2007), Canada (Centre for Addiction and Mental Health, 2002) and Australia (Marel et al., 2016) have outlined three different methods for dual treatment of co-occurring substance use and mental health conditions, namely: sequential, parallel and integrated models (see Table 1 for definitions). International guidelines recommend integrated treatment as the optimal treatment for co-occurring substance use disorders and mental health conditions (Centre for Addiction and Mental Health, 2002; Department of Health (England) and the Devolved Administrations, 2007; Kleber et al., 2007; Marel et al., 2016). Indeed the American Psychiatric Association’s guidelines on the Treatment of Patients with Substance Use Disorders exclusively outline an integrated treatment model for approaching co-occurring conditions (Kleber et al., 2007). However, to date, the supporting evidence for integrated care has focussed on general co-occurring mental health and substance use disorders which include more severe but less common disorders such as psychosis or illicit substance use (Drake et al., 1998, 2004; Hesse, 2009). One meta-analysis demonstrated integrated treatment of substance use and depressive disorders to be superior to single-focussed treatments for improving alcohol and depression-related outcomes; however, of the five included studies, only one was restricted to clients with alcohol misuse (Hesse, 2009).
Definitions of models for treating co-occurring mental health and substance abuse.
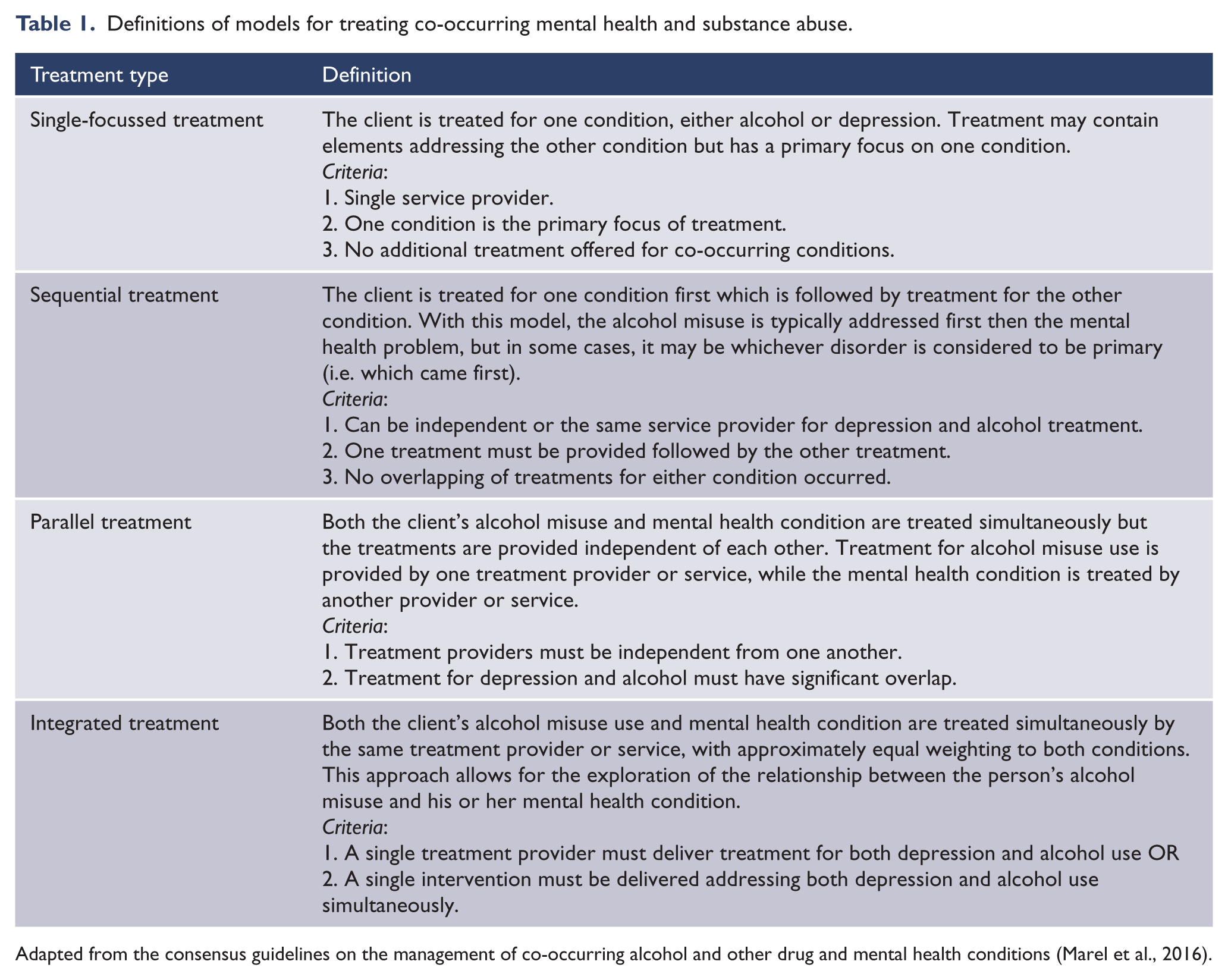
Adapted from the consensus guidelines on the management of co-occurring alcohol and other drug and mental health conditions (Marel et al., 2016).
To date, no reviews have examined the efficacy of these treatment models for co-occurring alcohol misuse and depression. Understanding whether one model is empirically superior (i.e. results in statistically significant improvements to outcomes measures) could improve effectiveness of future intervention studies and treatments.
Aims of the study
This systematic review will determine and summarise the: (1) methodological quality and characteristics of studies examining the effectiveness of psychosocial treatment of co-occurring alcohol misuse and depression using a sequential, parallel or integrated model; and (2) effectiveness of each dual-treatment model compared to single treatment for those with co-occurring alcohol misuse and depression.
Methods
Search strategy
A search of PubMed, Medline and PsycInfo databases for randomised and non-randomised comparative trials was completed on 4 August 2017. The search had no year restriction but was limited to humans, adults and English-language publications. The search terms were as follows: (Alcohol* OR ethanol OR drinking behaviour OR problem drinking OR hazardous drinking OR heavy drinking OR harmful drinking OR at-risk drinking) AND (Depress* OR major depression OR dysthym* OR unipolar depression OR primary depression) AND (Intervention). The search strategy is presented in Supplementary Appendix S1. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were adhered to (Moher et al., 2015).
Inclusion and exclusion criteria
Participants
Studies were eligible for inclusion if participants were aged over 16 years and reported some form of alcohol misuse (i.e. Diagnostic and Statistical Manual of Mental Disorders [4th ed., DSM-IV] dependence, DSM-IV abuse or researcher-defined harmful or risky use) or were undergoing treatment for alcohol misuse. Studies could include participants with other substance use problems; however, the majority of participants (>50%) had to report alcohol misuse to meet inclusion criteria. Where possible, the researchers extracted data for the alcohol misuse group only. Participants also had to report elevated depressive symptoms on a validated measure or have a diagnosis of depression. Studies could include participants with anxiety as long as the majority (>50%) had depression or elevated depressive symptoms. Where possible, the researchers extracted data from the depression group only. Studies examining children or adolescents and those involving mental health conditions other than depression or anxiety were excluded.
Intervention
Studies aimed at comparing the effectiveness of a psychosocial treatment delivered via one of the three dual-treatment models (sequential, parallel or integrated) compared to single-focussed treatment were included. Studies were excluded if they involved only pharmacological treatment comparisons.
Outcomes
Studies were eligible if they measured both alcohol use and depression with a standardised instrument at baseline and post-intervention, reported alcohol outcomes separately to other substance use outcomes and reported findings for depression outcomes separately to other mental health outcomes. Studies were excluded if their primary aim was to examine the differential effectiveness of treatment modality on study outcomes, or the impact of mediators, such as stress, on treatment outcomes.
Design
Studies were included if they used an experimental design recognised by the Cochrane Collaboration’s Effective Practice and Organisation of Care (EPOC) Group (randomised controlled trials, non-randomised controlled trials, controlled before and after studies or interrupted time series). Studies were excluded if they reported on the study protocol (i.e. did not present data).
Screening process
One author (B.H.) undertook the initial review of titles and abstracts. Of identified as potentially relevant for inclusion, a random 20% of abstracts were reviewed by an independent second reviewer (J.B.). Of the potentially relevant full-text articles, a random 20% were reviewed against all inclusion criteria by a second reviewer (J.B.). The kappa statistic demonstrated a 92% agreement rate between reviewers for full-text review (κ = 0.8312; p < 0.0012). Disagreements between reviewers were discussed until agreement was reached.
Classification of treatment model
All relevant full-text articles were independently categorised by three authors (B.H., J.B. and M.C.) using the treatment model criteria. Any discrepancies were resolved through discussion until consensus was reached.
Assessment of methodological quality
Methodological quality was assessed using the EPOC risk of bias tool for studies meeting design criteria (Cochrane Effective Practice and Organisation of Care (EPOC), 2015). All included studies were assessed independently by two authors (B.H. and J.B. or M.C.). Each study was rated against each criterion as: ‘Low risk’, where the EPOC criterion was met; ‘Unclear risk’, where there was not enough information provided; and ‘High risk’, where the EPOC criterion was not met. The EPOC criteria are as follows: adequate generation of allocation sequence, adequate allocation concealment, similar baseline outcome measurements, similar baseline characteristics of providers, incomplete outcome data were adequately addressed, prevented knowledge of allocated interventions, protection against contamination, no selective outcome reporting and free from other risk of bias. Disagreements between reviewers were discussed until agreement was reached.
Data extraction
Data extraction was undertaken by one author (B.H.) with a second author reviewing and revising the data (J.B. or M.C.). Data extracted included author, year, country, setting, eligibility, sample (total number of participants, age and gender), primary diagnosis, diagnostic tools, treatment model, intervention, outcome measures and follow-up time point(s), and treatment outcomes.
Data synthesis
Due to the low number of included studies and heterogeneity in the outcome measures and data reported, meta-analysis was not possible. A narrative approach to data synthesis was therefore adopted.
Results
Search results
Database searches returned 9498 abstracts. Manual searching of reference lists of included studies and other sources identified an additional two relevant studies which were assessed for eligibility. After duplicates were removed, 4909 titles were screened for relevance, 227 underwent abstract screening and 64 were then assessed for eligibility through full-text review (see Figure 1). Seven studies, reported in eight publications, met the inclusion criteria.
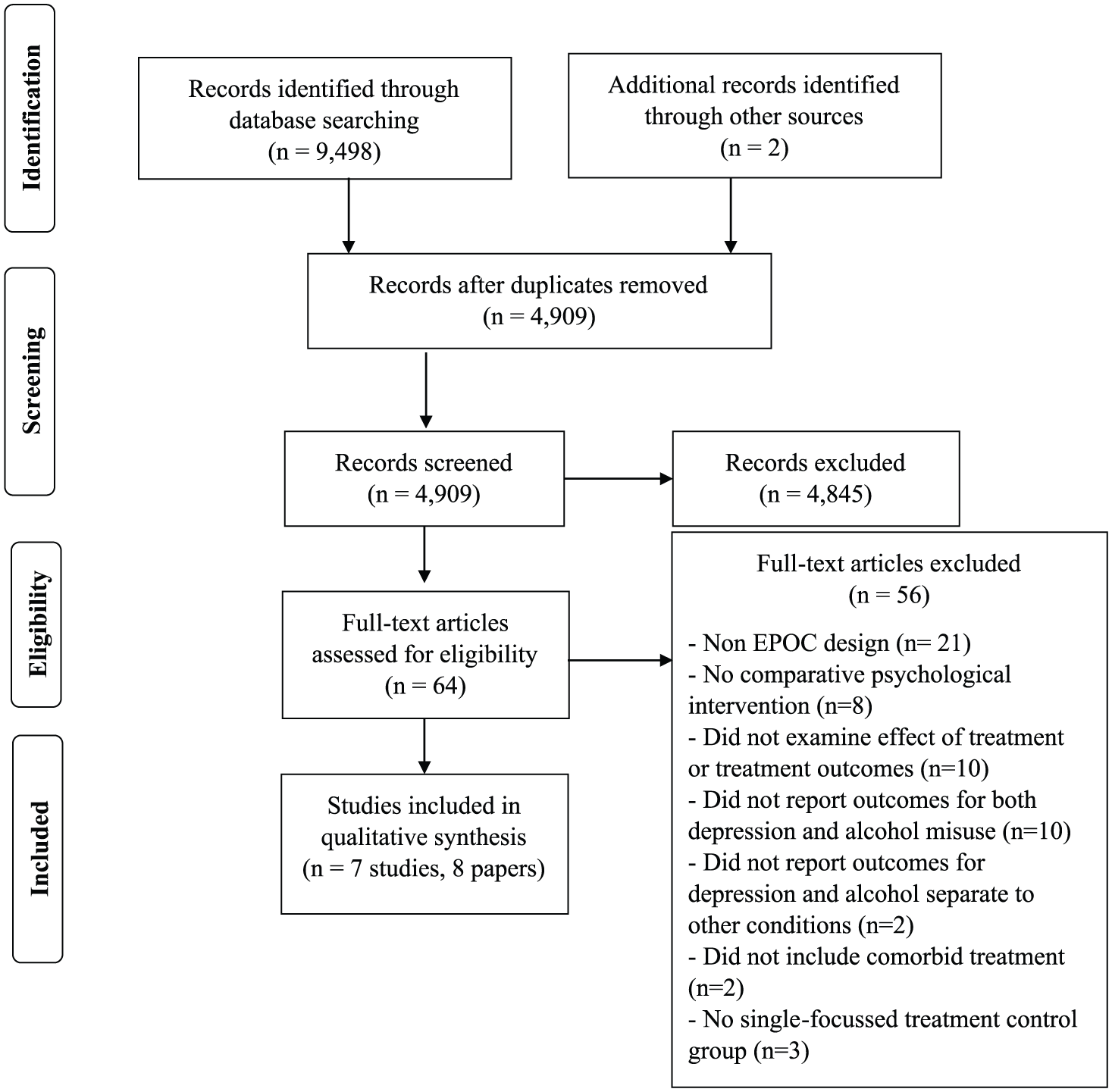
PRISMA flow chart of search strategy and article selection.
Study characteristics
All seven studies used an experimental design, of which four studies were randomised (Baker et al., 2010, 2014; Geisner et al., 2015; Morley et al., 2016; Oslin et al., 2003) and three were non-randomised (Brown et al., 1997, 2011; Watkins et al., 2011). Five studies were conducted in the United States (Brown et al., 1997, 2011; Geisner et al., 2015; Oslin et al., 2003; Watkins et al., 2011) with the remainder conducted in Australia (Baker et al., 2010, 2014; Morley et al., 2016). Study sample sizes ranged from 35 to 311. Outcome measures were assessed at follow-up time points ranging from 1 to 36 months, with five studies conducting multiple follow-ups (Baker et al., 2010, 2014; Brown et al., 1997, 2011; Morley et al., 2016; Watkins et al., 2011).
Methodological quality of included studies
No studies scored low risk on all nine EPOC risk of bias criteria (see Table 2). One study scored low risk on eight out of nine criteria (Oslin et al., 2003) and three studies scored low risk on seven out of eight applicable EPOC criteria (Baker et al., 2010, 2014; Geisner et al., 2015; Morley et al., 2016). All studies scored low risk for selective outcome reporting, baseline outcome measurements, adequately addressing incomplete outcome data and other risk of bias. Four out of seven studies were scored low risk for adequate generation of allocation sequence, preventing knowledge of allocated interventions and concealment of allocation. Adequate generation of allocation sequence was scored as unclear for one study that did not specify how the allocation sequence was generated (Brown et al., 2011) and two studies were scored as high risk as non-random methods of allocation were used (Brown et al., 1997; Watkins et al., 2011). Two studies were rated as unclear for adequate prevention of knowledge of allocation as they did not report who administered the outcome measures (Brown et al., 1997, 2011) and one was rated as high risk as outcomes were not blindly assessed (Watkins et al., 2011). Two studies were coded as high risk for concealment of allocation due to patient allocation methods being without a centralised form of concealment (Brown et al., 1997; Watkins et al., 2011) and one study was coded as unclear as no concealment method was specified (Brown et al., 2011). Protection against contamination was scored low risk for two of seven studies, with one study coded as unclear due to communication between study providers being possible (Morley et al., 2016) and four coded as high risk as patients were the unit of allocation (Baker et al., 2010, 2014; Brown et al., 1997, 2011; Geisner et al., 2015). Only two studies had the provider as the unit of allocation rendering the similarity of provider baseline characteristics criteria applicable. One study was rated as unclear as some provider characteristics were reported in text, but there were no data presented (Watkins et al., 2011) and one was rated as high risk as there were no mention of provider characteristics in text or data (Oslin et al., 2003).
EPOC methodological quality ratings of included studies.
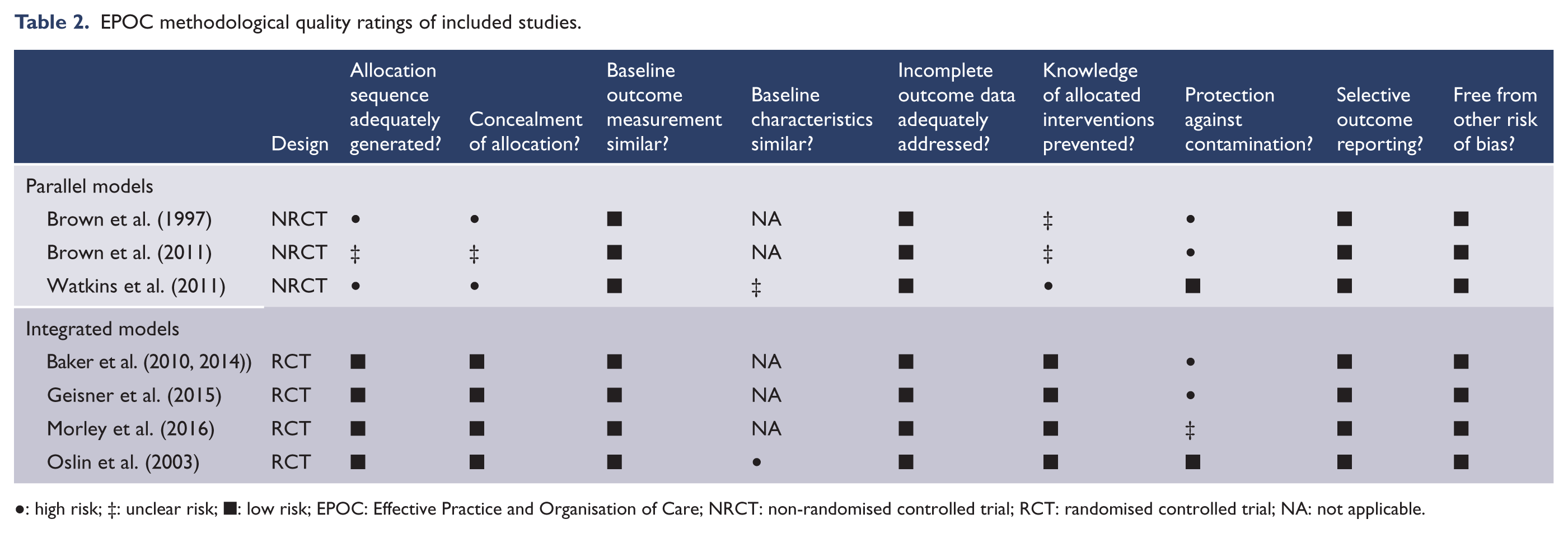
●: high risk; ‡: unclear risk; ■: low risk; EPOC: Effective Practice and Organisation of Care; NRCT: non-randomised controlled trial; RCT: randomised controlled trial; NA: not applicable.
Of the eight included publications, five specified at least one primary outcome (i.e. the key measurement) and three did not specify (Brown et al., 1997, 2011; Oslin et al., 2003). Three studies included a primary measure for depression using the Beck Depression Inventory-II (BDI-II) (Baker et al., 2010, 2014; Geisner et al., 2015; Watkins et al., 2011) and one using the Hamilton Depression Rating Scale (HDRS) (Oslin et al., 2003). Six studies included primary outcomes for alcohol using the following measures: Timeline Follow-Back (TLFB) (Baker et al., 2010, 2014; Morley et al., 2016; Watkins et al., 2011), Q-scores for alcohol from the Opiate Treatment Index (Baker et al., 2010, 2014), the CAGE questionnaire (Oslin et al., 2003) and the Daily Drinking Questionnaire and Rutgers Alcohol Problem Index (Geisner et al., 2015).
Effectiveness of treatment models
Of the included studies, none used a sequential model, three used a parallel model (Brown et al., 1997, 2011; Watkins et al., 2011) and four used an integrated model (Baker et al., 2010, 2014; Geisner et al., 2015; Morley et al., 2016; Oslin et al., 2003). Studies compared integrated or parallel models of care to usual care (Brown et al., 1997, 2011; Morley et al., 2016; Oslin et al., 2003; Watkins et al., 2011) or single treatment (Baker et al., 2010, 2012; Geisner et al., 2015). No studies directly compared a parallel model to an integrated model of care. A summary of treatment outcomes can be found in Table 3.
Number of follow-up time points with a significant intervention effect over the total number of follow-up time points for each study for both depression and alcohol outcome measures.
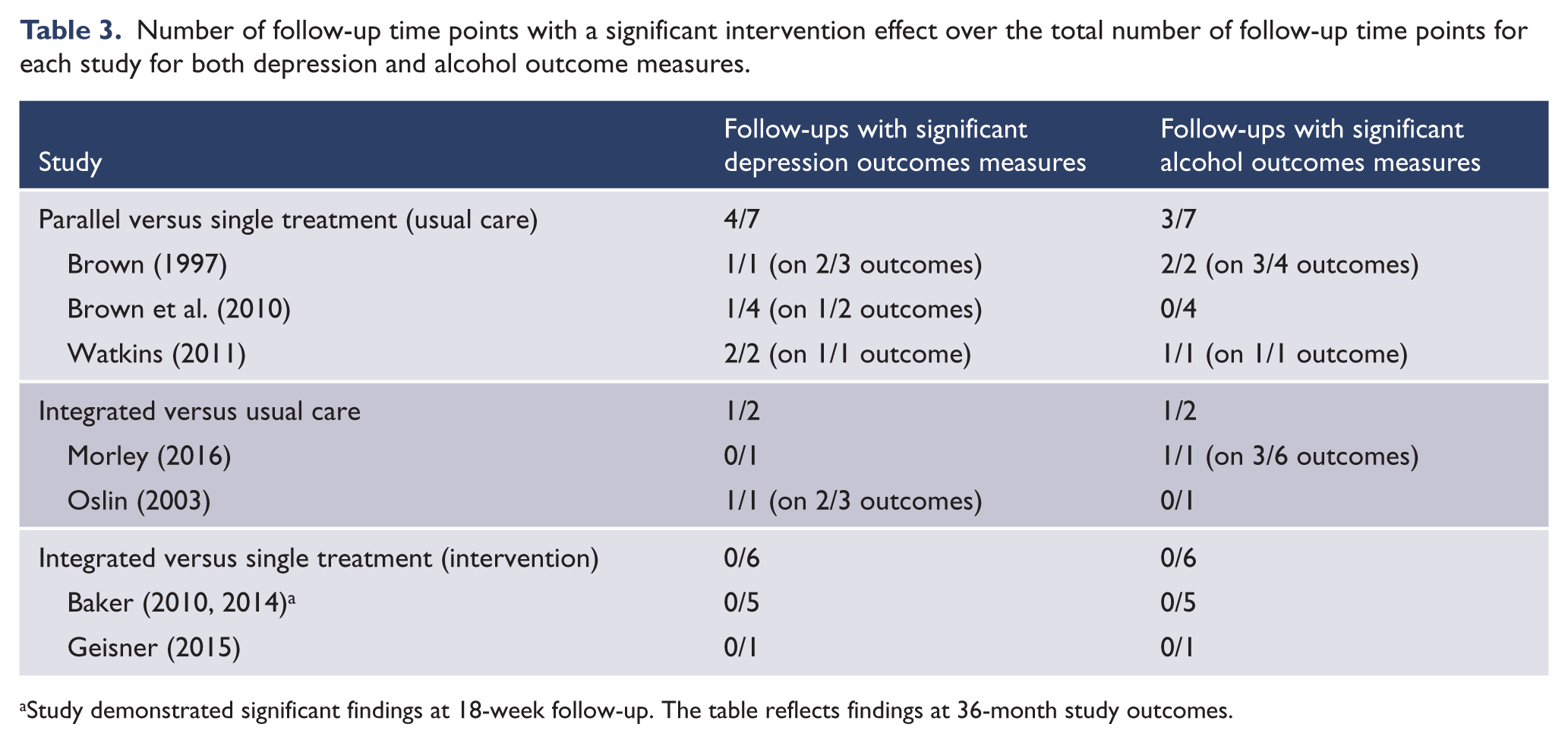
Study demonstrated significant findings at 18-week follow-up. The table reflects findings at 36-month study outcomes.
Effectiveness of a parallel model of care compared to single treatment
Three studies compared a parallel model of care to usual care (single-focussed alcohol treatment) (Brown et al., 1997, 2011; Watkins et al., 2011). In all three studies, participants in the parallel treatment condition reported greater improvements than those in the control condition(s) for alcohol use or depression for at least one follow-up time point. Brown et al. (1997) reported on a two-arm trial comparing eight individual sessions of cognitive behavioural therapy (CBT) for depression to eight sessions of a relaxation treatment control administered during a 21-day inpatient stay (Brown et al., 1997). Both groups received standard alcohol treatment consisting of a daily abstinence-oriented group treatment. The relaxation treatment control group was developed to account for contact time. This treatment involved meditative training intended to present patients with a viable alternative to drinking and decrease feelings of stress. As this was not intended to treat or manage depression, this group was considered a single treatment group. At the 3-month follow-up, individuals in the intervention group had a significantly greater proportion of days abstinent compared to the control group. At 6-month follow-up, individuals receiving CBT had significantly fewer drinking days, greater overall abstinence and fewer drinks per day than the control group. Individuals in the CBT group showed significant improvements in post-treatment depression scores compared to those in the control group (see Table 4). Brown et al. (2011) was a replication study of Brown et al. (1997) with an increased sample size, longer follow-ups and the intervention sessions administered primarily as outpatient treatment over a 6-week period (Brown et al., 2011). No significant differences in drinking outcomes were found between the two groups at the 6-week and 3-, 6- or 12-month follow-ups. Depression scores were significantly lower for the intervention group at 6-week follow-up, but no significant differences remained at the other follow-up points.
Characteristics of included studies.
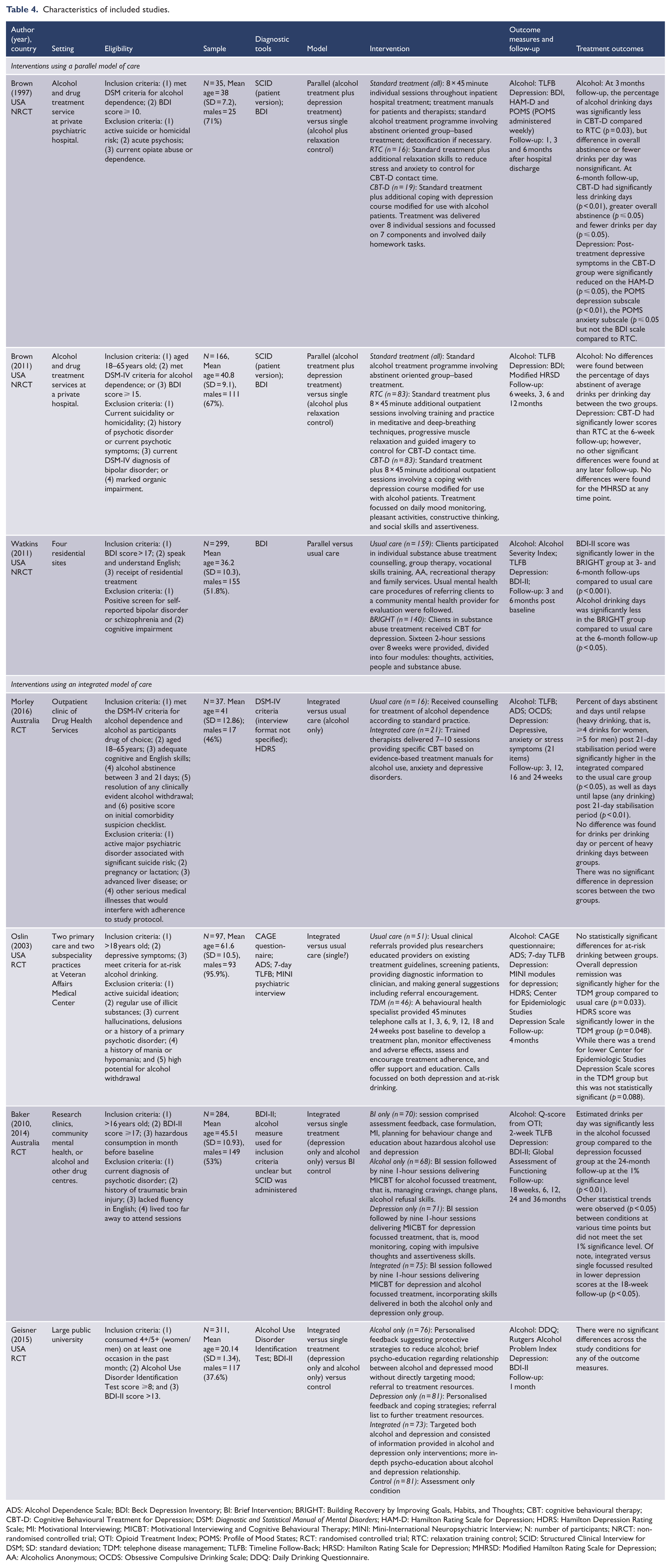
ADS: Alcohol Dependence Scale; BDI: Beck Depression Inventory; BI: Brief Intervention; BRIGHT: Building Recovery by Improving Goals, Habits, and Thoughts; CBT: cognitive behavioural therapy; CBT-D: Cognitive Behavioural Treatment for Depression; DSM: Diagnostic and Statistical Manual of Mental Disorders; HAM-D: Hamilton Rating Scale for Depression; HDRS: Hamilton Depression Rating Scale; MI: Motivational Interviewing; MICBT: Motivational Interviewing and Cognitive Behavioural Therapy; MINI: Mini-International Neuropsychiatric Interview; N: number of participants; NRCT: non-randomised controlled trial; OTI: Opioid Treatment Index; POMS: Profile of Mood States; RCT: randomised controlled trial; RTC: relaxation training control; SCID: Structured Clinical Interview for DSM; SD: standard deviation; TDM: telephone disease management; TLFB: Timeline Follow-Back; HRSD: Hamilton Rating Scale for Depression; MHRSD: Modified Hamilton Rating Scale for Depression; AA: Alcoholics Anonymous; OCDS: Obsessive Compulsive Drinking Scale; DDQ: Daily Drinking Questionnaire.
The Watkins et al. study was also a two-arm controlled trial (Watkins et al., 2011). Standard residential substance abuse treatment was compared to standard treatment plus 16 two-hour group sessions of CBT for depression over an 8-week period. The administered CBT treatment was adapted to incorporate an additional module on substance abuse, however, the primary focus of the treatment was depression, therefore this intervention was categorised as parallel treatment. The intervention group showed significantly lower depression scores at the 3- and 6-month follow-up and had significantly fewer drinking days at the 6-month follow-up.
Effectiveness of an integrated model of care compared to single treatment
Studies comparing integrated care to usual care
Two studies compared an integrated intervention to usual care (single-focussed alcohol treatment). One study found improvements for alcohol outcomes and the other showed improvements for depression outcomes. Morley et al. (2016) conducted a two-arm trial which employed an integrated CBT intervention for alcohol use, depression and/or anxiety, delivered in 7–10 outpatient sessions over a 12-week period. The usual care group only received counselling for alcohol dependence in accordance with standard practice. The sample included individuals with anxiety; however, 64% had a primary or secondary diagnosis of a depressive disorder. At 12-week follow-up, Morley et al. found significantly better outcomes for the intervention group on three out of five alcohol-related outcomes (see Table 4). There was no significant difference between the two groups for depression scores, but the study was not adequately powered to detect such a difference.
Oslin et al. (2003) conducted a two-arm trial examining the effect of integrated treatment delivered via a telephone disease management programme compared to usual care for older veterans. Little information was provided regarding the theoretical underpinnings of the programme. The integrated treatment involved a disease management approach for depression and adaption of a brief alcohol intervention. The telephone disease management group received seven calls from a behavioural health specialist over a 24-week period. The usual care group were referred to an outpatient behavioural health clinic. The intervention group demonstrated significant improvements for depression response, defined as an HDRS score of ⩽10 or a 50% reduction in depressive symptoms, compared to the usual care group at the 4-month follow-up. There was no significant difference in at-risk drinking response between the two groups at follow-up.
Studies comparing integrated care to single-focussed interventions
Two studies compared integrated interventions to single-focussed interventions for either alcohol or depression. One study found an effect for alcohol-related outcomes. No studies found differences for depression outcomes. Baker et al. (2010, 2014) conducted a four-arm trial consisting of a 90-minute single session integrated intervention for all participants followed by no further treatment, nine sessions of single-focussed treatment (alcohol or depression), or nine sessions of integrated treatment. Three primary alcohol-related outcomes and one depression outcome were measured across five follow-up time points from 18 weeks to 36 months. Baker et al. (2010) found a significantly greater reduction in average drinking days per week and depression scores for the integrated treatment group compared to the alcohol/depression single-focussed groups at the 18-week follow-up (Baker et al., 2010). However, a more stringent p-value was used to account for multiple testing in the long-term outcome paper and this effect was lost (Baker et al., 2014). No significant differences between the integrated and the alcohol/depression single-focussed interventions were found at any other follow-up time point.
Geisner et al.’s four-arm trial examined integrated versus single treatment for alcohol or depression versus a control group (no treatment) using a personalised, web-based intervention for college students (Geisner et al., 2015). Participants in the integrated or single treatment conditions received weekly email invitations to review their feedback over a 5-week period. The control group was provided with treatment resource information. Geisner et al. found no significant differences for alcohol or depression-related outcomes between any of the treatment conditions at the 1-month follow-up.
Discussion
This is the first systematic review to examine the methodological quality and effectiveness of dual-treatment models for co-occurring alcohol misuse and depression. It identified seven evaluations of three parallel models that were of low to moderate quality and four integrated models that were of reasonable quality. There is little evidence to date that dual models achieve significantly better patient outcomes than single models. For dual treatment, the apparent superiority of parallel models of care relative to integrated care is tempered by their relatively low methodological quality.
Methodological quality of included studies
The overall methodological quality of included studies was moderate with no studies rated low risk on all EPOC criteria and three studies rated low risk on four or fewer criteria (see Table 3). The findings of this review therefore need to be interpreted with caution in light of these limitations. For the studies using a parallel treatment model, two were low risk on 4/8 EPOC criteria and one was low risk on 5/9 criteria. Studies using an integrated model demonstrated better methodological quality than parallel studies with low risk scores on 7/8 (Baker et al., 2010, 2014; Geisner et al., 2015; Morley et al., 2016) or 8/9 (Oslin et al., 2003) applicable criteria. One study was classified as unclear for only one EPOC criteria (Morley et al., 2016). It is possible that this criterion was associated with low risk of bias, but full details were not reported in the published texts.
Another methodological issue consistently noted in the included literature was the use of multiple outcome measures combined with a lack of specificity regarding primary outcomes. In addition, adjustments for multiplicity were commonly overlooked. Although selecting a primary outcome variable for alcohol misuse is difficult due to the various ways to measure alcohol use, included studies used up to six different outcomes to determine intervention effects. Therefore, it is difficult to determine whether significant findings are clinically relevant for patients or are due to type 1 statistical errors (Bender and Lange, 2001). Future intervention trials should ensure careful consideration of clinically relevant outcomes during the study inception phase to overcome this issue. If multiple outcomes are necessary to determine change, appropriate statistical testing should occur and be accounted for in power calculations and hypothesis development.
Effectiveness of dual-treatment models
While there was some indication that parallel treatment outperformed single treatment within residential settings, overall these studies performed poorly on the risk of bias criteria making it difficult to determine the reliability of the results. Furthermore, only one integrated study showed greater improvements for depression (Oslin et al., 2003) and one for alcohol misuse (Morley et al., 2016). However, these studies also included multiple outcome measures, of which not all demonstrated this improvement (see Table 3). Therefore, there is little evidence demonstrating that psychosocial dual-treatment models result in greater improvements to outcomes compared to single models of treatment. This finding contrasts with previous reviews focussing on other substance use and co-occurring mental disorders (Drake et al., 2004, 2008; Hesse, 2009). This may indicate that psychosocial treatment for alcohol misuse or depression is sufficient in reducing symptoms for both, which may not be the case for more severe co-occurring conditions such as substance use and psychosis (Drake et al., 2004). This is apparent in several of the included studies where an effect of time was found; however, given the scope of the current review, these data were not extracted. In addition, alcohol-focussed treatment was as effective as depression-focussed treatment in reducing depression and more effective in reducing alcohol consumption in the study by Baker et al. (2014) (data not extracted). Interestingly, in the same study, the authors found that sizable improvements in levels of depression and alcohol consumption occurred in association with the screening and assessment process, and change in one domain was related to change in the other (Baker et al., 2013). The authors proposed that a warm and engaging health professional simply inquiring about levels of depression and alcohol consumption, followed by feedback and goal setting may be sufficient to produce significant early change in both depressive and alcohol use domains. The effectiveness of brief integrated or transdiagnostic approaches would seem worthy of further investigation, followed by single, parallel or integrated approaches (if needed) depending on progress in reductions in depression and alcohol use.
Evidently, within the current review, significant improvements in outcomes for dual-focussed interventions were primarily attributed to studies comparing it with usual care within routine practice (Brown et al., 1997, 2011; Morley et al., 2016; Oslin et al., 2003; Watkins et al., 2011) and less apparent among studies comparing dual-focussed interventions with controlled single-focussed interventions (Baker et al., 2010, 2014; Geisner et al., 2015) (see Table 3). Significant findings may therefore be attributed to a lack of standardised care administered in routine practice rather than superiority of dual-focussed treatment. The lack of evidence for dual-focussed psychosocial treatment could also be attributed to the limited number of studies performed in this area and the lack of methodological rigour and standardisation of available studies. For instance, the studies using a parallel model of treatment demonstrated improvements in some alcohol and depression outcomes; however, they also met few EPOC criteria for low risk of bias (Table 2) (Brown et al., 1997, 2011; Watkins et al., 2011). The potential high risk of bias and the lack of comparable control groups between parallel and integrated studies also prevent drawing firm conclusions about whether one model of dual-focussed treatment is superior to another.
Implications
This systematic review highlights the lack of methodologically rigorous studies evaluating different models for psychosocial treatment of co-occurring alcohol misuse and depression, resulting in a paucity of evidence to inform clinical practice. Recommendations for implementing integrated care routinely into clinical practice require costly and resource-intensive strategies. It is therefore important that assessment and monitoring of alcohol misuse and co-occurring symptoms of depression and anxiety inform practice and that various treatment models be considered when implementing care. While integrated interventions are commonly recommended for treatment of co-occurring mental and substance use disorders, there is little evidence supporting this for psychosocial treatment of co-occurring alcohol misuse and depression. Future studies in this field should focus on continuing to assess depression and alcohol consumption from screening, through assessment and intervention and employing methodologically rigorous research designs, outcome measures which are clinically relevant and have a strong empirical justification, and a systematic and rigorous comparison of different treatment models.
Limitations
This review should be considered in light of two main limitations. There was heterogeneity between the populations for the included studies. The data are based on studies conducted with college students, veterans, treatment seekers and community members. Furthermore, the authors included studies with other substance use or anxiety disorders if the majority of the sample were alcohol misusers or had depression. This decision was made due to the small number of studies available in this area of research; however, it increases the heterogeneity of the included papers. Once a stronger research base is established in this area, examination of treatment outcomes in specific subgroups should be considered. In addition, this review may not be a comprehensive review of the literature due to the exclusion of non-EPOC studies and non-English studies. While excluding non-EPOC design studies was an attempt to ensure the results of the review were based on the best available evidence, the exclusion of non-English studies was due to logistical issues relating to language translation. The search results may not have located all relevant literature; however, given the large number of studies returned using this search strategy, the authors expect this to be a reasonably comprehensive review of the available literature.
Despite the impact of these co-occurring conditions, there is a lack of high-level evidence to inform clinical practice and treatment guidelines. The available evidence demonstrates risk of bias or little to no improvements when compared to single-focussed treatment. Greater evidence is required to determine the optimal treatment model for this co-occurring condition; however, future researchers can utilise this review to inform intervention trials.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
B.H. is supported by an Australian Rotary Health Ian Scott Mental Health PhD Scholarship. J.B. is supported by an Australian Research Council Post-Doctoral Industry Fellowship. A.L.B. is supported by an NHMRC Senior Research Fellowship. R.P.M. is supported by an NHMRC Principal Research Fellow Award.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.