
Abstract
Despite extensive global efforts to prioritise and improve primary mental health care, challenges and opportunities within resource-constrained settings, particularly in low- and middle-income countries (LMICs) such as South Africa, persist. The study explored the barriers and opportunities in primary mental health care in a resourced-constrained setting in the Eastern Cape, South Africa. Moreover, and based on the rationale, the study explored how staff and patients within a low-resource community experience and perceive mental health care at a primary health level. Using a qualitative method, semi-structured interviews were conducted with 24 participants (patients = 11, staff = 13), recruited using purposive sampling. Thematic analysis of the data revealed three overarching themes: (1) Challenges and opportunities, (2) Medication and admission, and (3) Mental health is misunderstood. The findings suggest that patient experiences of mental health care in primary health clinics are complex, approaches to mental health care are predominantly pharmacological and that mental health stigma persists. The findings indicate the need for integrative approaches to mental health care and improved mental health literacy in communities. They also align with the key action areas outlined in the National Mental Health Policy Framework and Strategic Plan (2023-2030). However, decisive governmental investment, implementation, and leadership are necessary. Future research, through systems approaches and implementation science, should focus on enhancing primary health clinic experiences, expanding mental health care provision through various community-based implementation strategies, such as task-sharing, low-intensity psychological interventions, and implementing mental health literacy initiatives to mitigate the impact of mental health stigma.
Introduction
The last decade has highlighted the need to prioritise and improve mental health care globally (Patel et al., 2018). The inadequacy of mental health care globally has not only been described as a public health crisis but as a human rights violation (World Health Organisation [WHO], 2021a). Saxena (2016) reported that the global mental health field has made noteworthy strides in advancing a research agenda to develop and disseminate knowledge, developing leadership and technical support where needed, monitoring health situations, and developing ethical and evidence-based policy options (Saxena, 2016). Moreover, the updated World Health Organisation’s comprehensive Mental Health Action Plan 2013 to 2030 reaffirms the need to (a) strengthen mental health leadership and governance; (b) provide integrated and responsive community-level-based mental health care; (c) implement promotion and prevention strategies, (d) and strengthen information systems, evidence, and mental health research (WHO Action Plan 2013-2030) (WHO, 2021b). The United Nations Sustainable Development Goals (United Nations, 2015) and the African Union Agenda 2063 (African Capacity Building Foundation, 2016) emphasise the importance of health for all persons. Ultimately, the efforts of the past decade have been based on the dictum: ‘There is no health without mental health’ (Saxena & Skeen, 2012). Global mental health efforts have resulted in the development of scalable psychological interventions and prioritisations of increasing access to mental health care, especially in low- and middle-income countries (WHO, 2016). Nevertheless, low- and middle-income countries (LMIC), such as South Africa (SA), still have long-standing challenges to increasing mental health care access at the community and primary care level (Petersen et al., 2019; Sorsdahl et al., 2023).
The South African public health care system consists of three types of health services: primary health clinics, secondary health clinics, and tertiary health care. Primary health is designated to cover larger services of care; secondary or district services require inpatient care, and tertiary focuses on more specialised care (Marais & Petersen, 2015). Importantly, primary health clinics are based in various communities to serve the respective communities daily, yet these clinics do not always receive the necessary resources (Marais & Petersen, 2015). A study by Petersen et al. (2019) found that integrating mental health care into existing primary health care services in South African communities is complex. Based on qualitative interviews conducted with several health managers and service providers (n = 121) across six LMICs, including South Africa, Petersen et al. (2019) found that several components were required for the synergistic integration of mental health care in primary health clinics (PHCs). For example, Petersen et al. (2019) stated that the availability of human resources to enable task-sharing initiatives of mental health care; securing financial investment and budgeting, and improved governance to ensure multi-sectoral collaborations, among other things, are crucial to enabling primary mental health care (Petersen et al., 2019; Shisana et al., 2024; Sorsdahl et al., 2023).
Notwithstanding the above-mentioned barriers, the updated Mental Health Policy Framework (MHPF) (2023-2030) of South Africa provides objectives, ranging from strengthening mental health promotion and advocacy to training primary mental health care staff in basic mental health care and detection, among other things (Lund, 2023). The MHPF is a crucial blueprint for understanding priorities and providing clear goals. Yet, a large part of the long-standing challenges in mental health provision relates to minimal financial investment and poor leadership and governance, which remains a risk for updated MHPF (2023-2030) (Lund, 2023).
For example, in the North-West Province, stakeholders (n = 17) from the Department of Health and the Department of Social Development in the Kenneth Kaunda District were interviewed regarding systemic factors within institutional and policy contexts likely to facilitate or impede the implementation of integrated mental health care in South Africa. The study found that new policies were being developed that embraced task-sharing approaches and interventions to mitigate mental health stigmatisation, among other things. This said, some challenges were still related to poor governance and policy implementation at provincial levels, infrastructural constraints, and the lack of a dedicated mental health budget (Marais & Petersen, 2015).
A study conducted in the Eastern Cape (EC) by Strümpher et al. (2014) found that professional nurses working at primary, secondary, and tertiary level health care facilities reported that barriers to mental health care ranged from a lack of leadership and limited financial investment, to facility infrastructure, among other things (Strümpher et al., 2014). Similar findings were reported by Booysen et al. (2021) in the Eastern Cape, where limited trained mental health professionals and mental health stigma were identified as structural and attitudinal barriers. Of concern, is that mental health care at the provincial level remains stagnant and beleaguered by persistent issues of low prioritisation of financial investment and good governance (Lund et al., 2010; South African Human Rights Commission, 2019).
Considering the global efforts to improve mental health and the impact of the existing barriers to mental health care at the primary care level, especially in LMICs, the aim and rationale were to explore and ascertain the barriers and opportunities in primary mental health care in a resource-constrained setting. Moreover, the study was guided by the following research question: How do staff and patients within a low-resource community experience and perceive mental health care at a primary health level? By including both patients and staff in the study, we aimed to have a more nuanced understanding of the challenges and opportunities regarding primary mental health care in a resource-constrained community.
Method
Participants
Qualitative research refers to the methodological and systematic practices focused on producing knowledge of a person’s experiences and actions within a social context (Levitt et al., 2017). Considering the aim of the study, a descriptive qualitative research approach was used to explore the experiences and perceptions of participants within a specific social context. The sample consisted of mental health care users (hereafter referred to as patients) from a low-resourced community, professional nurses, and facility managers (hereafter referred to as staff members) working at PHCs in the Makana Municipality, Eastern Cape, South Africa. Staff and patients were 18 years and older, with the majority of the patients being unemployed. Their general level of education ranged from primary to further education levels. A purposive sampling strategy was used, based on one key characteristic of the participants: patients accessing health care at PHCs and staff working at a PHC. Twenty-four persons (11 patients and 13 staff members) spread across four PHCs in the Makana Municipality participated in the study. The recruitment process started by obtaining gatekeeper permission from the relevant sub-district department of health, which informed the local clinics of the study. Facility managers interested in knowing more about the study met with the first author and research assistants who presented information about the study and answered any related questions. After the information sessions, the facility managers requested staff to inform patients about the study. If they were interested, the clinic staff informed the research assistants of the number of interested patients and staff, thereafter scheduling a date and time for information sharing at the respective clinics. The research assistants who met with the interested staff and patients, had an opportunity to present information about the study again, answer any questions, and obtain consent from staff and patients.
We used the ecological systems theory (Bronfenbrenner, 1979; Crawford, 2020) to conceptualise the experience and perceptions of staff and patients within the context of PHCs and the broader social and health care systems. Ecological systems theory purports that a person’s functioning and development must be understood within the different systemic layers that are nested and interdependent. In the present study the qualitative data can be understood from an individual, organisational, community, and societal level as well as how these systems interact from a nested systemic perspective. For example, participants’ perceptions of mental health at a community level can be influenced by various systems, such as family, community, and culture (Crawford, 2020).
Interview guides
Two separate interview guides were developed for patients and staff, and an iterative question conceptualisation and refinement process was undertaken. Questions for patients included: (a) What is your experience of the services you access at the clinic? (b) Where could a person access support for mental health care? (c) Is there a need for mental health care in your community? For staff, questions embraced: (a) How does the general community view mental illness? (b) Does the work of your clinic involve issues related to mental health? What is this work? (c) How important is mental health for the clinic, compared to other health conditions? (e) Would the community access mental health care at a clinic level if the services were readily available?
Several strategies informed the development of the interview guide; first, interview guides for facility managers were based on the World Health Organisation’s Mental Health Atlas Questionnaire. Interview guides for service users and staff at PHCs were informed by relevant public mental health literature (i.e., Kleintjes et al., 2010). Once interview guides were drafted, the clarity and relevance of the questions were discussed prior to interviews and were refined as interviews were conducted.
Procedure
Upon ethical approval from Rhodes University and the Eastern Cape Department of Health, several PHCs were invited to participate in the study. Two post-graduate students in clinical psychology conducted semi-structured interviews of about 30-60 minutes. The student clinical psychologists were trained in interviewing skills and had no conflicts of interests, as they were unfamiliar with the clinics, patients, and staff. All interviews were audio recorded and conducted in the interviewee’s language; therefore, interviews were conducted in English, Afrikaans, and isiXhosa. Interviews were transcribed and translated by a professional and qualified language and transcription expert, to ensure data accuracy.
Ethical considerations
Ethical approval was obtained from the Rhodes University Human Research Ethics Committee (Review Reference: 2022-5578-7109), and gatekeeper permission was obtained from the Eastern Cape Department of Health (EC_202209_008). Considering the focus (i.e., primary health care patients and staff) and setting (low-resourced community), we had to safeguard against any risk and harm towards an ostensibly vulnerable population. Therefore, participants were informed about the study by the various clinic managers and were not approached directly by the researchers. All patients and staff who participated provided written informed consent. Interviews with staff and patients were held in private consultation rooms at the various PHCs, thus ensuring privacy and anonymity and limiting any stereotyping or stigmatisation towards their participation. No adverse events were noted or reported, and none of the participants required counselling, due to their participation in the study.
Data analysis
The first author conducted the thematic analysis and coding. Trustworthiness and the credibility of the data were ensured through audio recordings, record-keeping of the coding, and using a qualitative analysis software system that kept a record of the coding process. Rigour was maintained through discussions of the analysis and results with the second author. Discussions with the second author and research assistants created an awareness of certain biases within the data. All interviews were audio recorded and transcribed for accuracy. An established analytic framework (i.e., thematic analysis) was used to ensure the credibility and trustworthiness of the findings (Johnson et al., 2020). Thematic analysis was used to analyse the interview data and to highlight the salient themes that were identified across the interviews (Braun & Clarke, 2019).
Interviews were audio recorded, and participants could speak English, Afrikaans, or isiXhosa. Audio recordings were transcribed and translated by a professional language editor and transcriber. The completed transcripts were entered in NVivo 12 for analysis and coding. Transcripts were then read, and initial codes were generated using NVivo. NVivo visualisation graphically displayed the initial coding and relationships to assess the coding frequency across participants and synthesise superordinate codes. Coding procedures were reviewed for clarity and consistency, and supporting textual evidence. The themes with the most textual support and evidence from participants were selected based on endorsement by the various patients and staff.
Findings
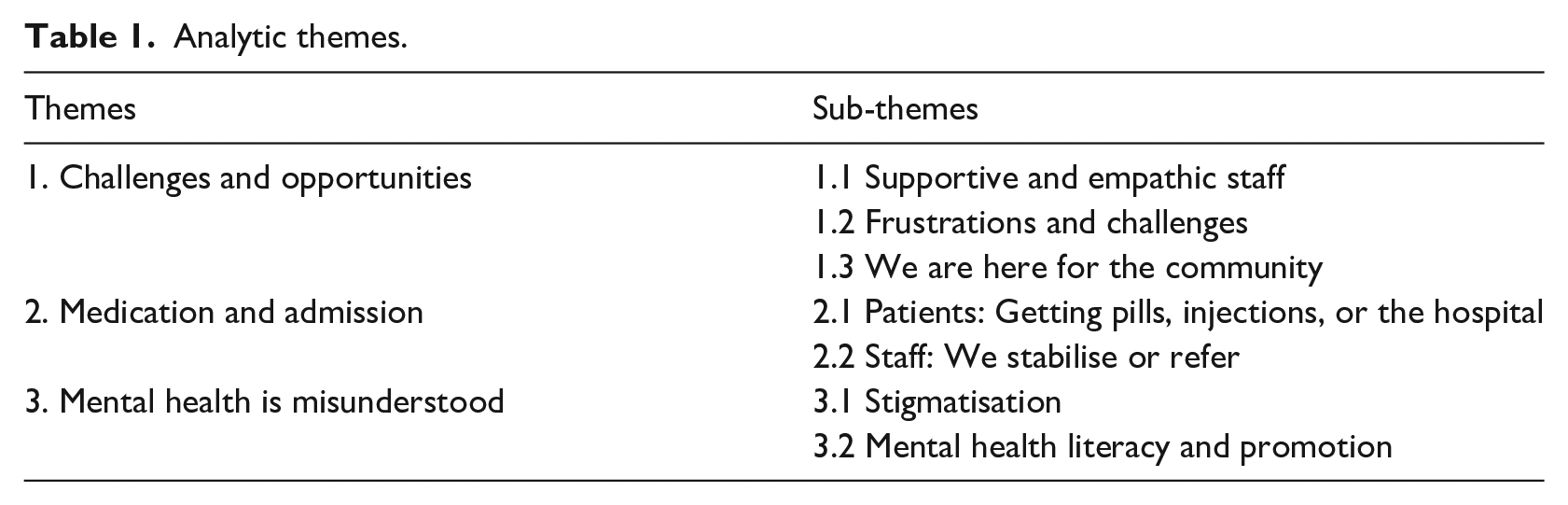
The thematic analysis resulted in three overarching themes and seven sub-themes related to the patient and staff member interviews (See Table 1).
Analytic themes.
Theme 1: challenges and opportunities
The theme outlines patients’ and staff’s complex relational experiences within the context of PHCs. It highlights, amid the complexity, the opportunities for PHCs to serve a more dynamic role within communities.
Sub-theme: 1.1: supportive and empathic staff
This sub-theme demonstrates how patients experienced services at PHCs across the various communities in the municipality. Patients highlighted experiences of a supportive and compassionate nature. Patient 1 stated, I love it very much. And the way they treat us makes me very happy. If someone is very sick now, the nurses will ask others to allow that person in first. ‘Can we please allow this one first? He is very sick so that we will get back to you’. Their service is very good . . .
Patients’ experiences in some PHCs reflect a caring and accommodating environment between patients and staff and a collective sense of care at PHCs. These experiences were further described by patient 3, who stated, ‘That’s why I like this clinic. And I receive good treatment here. Health care worker[s] here are very compassionate, and they are caring as well’. Moreover, patient 7 highlighted the value and function of the relationships that are developed with staff at PHCs: I have my favourite people, my favourite nurse or sister, I’d like to see. They know my situation. . . [yet] it’s [also] government, so you can’t choose who you want to see. So when you see someone you don’t want to see, you keep things very limited. . .
The above extracts illustrate the relational processes that exist as part of the general health care services at PHCs. Within PHCs, and between staff and patients, a collective sense of care and support is experienced within some of the PHCs.
Sub-theme 1.2: frustrations and challenges
This sub-theme describes the more complex and challenging aspects of PHC services. Patient experiences of PHCs are underpinned by tension and frustration. For example, Patient 6 stated, ‘I wish more nurses could be added because they are so few’. Other patients had concerns regarding privacy and confidentiality. For instance, Patient 4 reported, ‘You will see about your business on Facebook, and they will talk about you on WhatsApp. You see? So, you can’t be comfortable because they write about you on WhatsApp or Facebook’. Patient 4 further described how, at times, interacting with staff can be confrontational: Sometimes they attend to me nicely, and sometimes they don’t. Sometimes, other nurses don’t speak nicely with you. You see? You become humble when you get to the clinic, so you speak nicely. Maybe one of them will not answer you nicely because they want to provoke you.
The above extract illustrates how some patients’ experiences with PHCs are dynamic and challenging. Patients need to navigate difficult interactions, and some need to ‘humble’ themselves to avoid conflict or humiliation. Patients 4 and 5 further described their experiences of frustration due to delayed services at PHCs: ‘Even if you arrive at 7:00 or 8:00, you can leave around 14h00 to 15h00. They don’t even have soup for old people who could take treatment. There’s no soup, there’s nothing’ (Patient 4). The above excerpts reflect the challenges of limited staff, confidentiality, and interpersonal tensions between staff and patients, due to being within a resource-constrained environment. These experiences reflect the more intricate experiences between staff and patients within the PHC system. For example, the sub-theme also alludes to the deeper challenges staff and patients need to navigate and that expectations from patients can go beyond health care to social support; for example, receiving food for those who do not have the resources. For staff, it can become difficult to maintain the standard of care and service while your work environment is arguably the source of the frustration. As a result, patients and staff impact each other and the environment of service and care.
Sub-theme 1.3: we are here for the community
Patients and staff also shared an appreciation for the function and role of PHCs in communities. Yet, operating in a resource-constrained environment with limited infrastructure made it challenging to maintain adequate services. Staff member 10 stated: We have an established clinic committee. . . when we have input, we listen. And we do react to what they want. Because, at the end of the day, [it] is what the community wants. It’s not what I want. And I’m here to provide a service.
Staff member 10 also highlights the impact of resource constraints, especially limited infrastructure, (So with the building, unfortunately, we can’t do anything. It’s structural. So we’ll have to be very innovative). Staff member 15 stated that PHCs do not only provide health services, but they also serve a broader community function of support: We’ve got a good relationship with our clients because what makes me say that, even the people who moved from this area go and stay in other areas . . . they don’t want to come to other clinics, even if you can ask why don’t you go to your nearest clinic, cos there is a clinic in Joza, there’s a clinic in Extension 7. Still, they will tell you, no we want to come here.
This extract illustrates the importance of adequate services and how they can enable longer-lasting relationships between PHCs and patients. Furthermore, staff were asked if community members would access broader mental health services if they were available at PHCs: Staff member: Obvious because we are here for the community. If kukho uncedo abalu-needayo ikhona chance yoba bangalufumana eclinic [there is the help they need, there is a chance they can get it at the clinic].
The three sub-themes describe the frustrations and opportunities of care in a resource-constrained setting. In addition to health services, this theme suggests opportunities for PHCs to fulfil a broader community role.
Theme 2: medication and admission
This theme describes the current approach towards mental health care patients at a PHC level. It reflects a limited approach to mental health care, especially at a primary health care level.
Sub-theme 2.1: patients: getting pills, injections, or the hospital
This sub-theme describes patients’ and staffs’ perceptions and understanding of mental health care at a PHC level. It highlights two approaches to mental health care, namely, pharmacological treatment and hospitalisation as the primary approach to mental health care at PHCs. Patients generally understand that mental health care at PHCs is to dispense medication, or refer or admit persons with severe psychiatric conditions to the hospitals. Patient 1 reported that you ‘always have to start by the clinic, go to a doctor. So they can send you to the psychiatric hospital if you need help or whatever like that’.
Patient 2 stated, ‘I must come to the clinic; the clinic will send me to the hospital. The hospital will send me to the psychiatric hospital. I will be treated there, and I will be all right’. Patients understood that PHCs provide treatment focused on pharmacology, as described by Patient 6: ‘Here they can give me pills. Maybe they can inject me as well. If I do not get well, I am sent to the hospital’. Based on these reflections, mental health care at a PHC level is largely focused on pharmacology and hospitalisation. This said, a small number of participants referred to cultural practices. Patient 3 stated, ‘When we do traditional things like ceremonies... African beer, slaughtering the cattle, sometimes the stress is so much less. Because you know that. . . to do this thing for our ancestors’. According to patient 3, culturally informed practices are also used to address mental health-related difficulties.
Sub-theme 2.2: staff: we stabilise or refer
Staff working at four different PHCs in the municipality reported that their focus at a PHC level was to provide pharmacological treatment and, if necessary, refer and admit patients for observation and possible admission to a psychiatric hospital. The following exchange reflects the general focus of mental health care at a PHC level:
They only come with a need to be transferred to psychiatric hospitals or the ones who are adhering to their treatment.
So, would you say that here at the clinic, you provide just a referral to a psychiatric hospital?
For those who are mentally disturbed, but those who are mentally disturbed on treatment and responding well to the treatment, they’re fine; they come here for meds.
The above description is supported by several other staff statements that mental health care at the community level is solely on a pharmacological level for patients who merely follow up to receive medication. Staff member 12 described her understanding of mental health care at PHCs: . . .people are just here to take their medication, not for us to assess them to investigate and dig deep. It’s just they come for their treatment, then we observe and ask if everything is okay because maybe the medication is working and you have any side effects. . .
The above extracts align with how patients described their understanding of mental health care at PHCs. Nevertheless, some staff members expressed a broader understanding and, arguably, how members from the community do experience general mental health distress that requires a different form of support that is not available at PHCs. For example, Staff Member 16 stated: This person needs someone to talk to, even if it’s just to sit and unburden all this she is feeling because we can’t run away from the fact that our families have issues and are broken. That generational brokenness that happened, you see. Those things people are still carrying some of those things here.
The above extract highlights a subtle, yet deep awareness and empathy staff have towards patients. This support and care can also mean creating a supportive and empathic environment for patients at PHCs. Yet, the sub-themes presented above suggest that mental health is still mainly understood and approached from a pharmacological perspective and that broader understandings of mental health care, such as psychosocial care, remain eclipsed at the community level.
Theme 3: mental health is misunderstood
The theme describes barriers, such as stigma and mental health literacy in primary health settings. The sub-themes highlight the impact of both stigma and mental health literacy but also describe the importance of mental health promotion as a means to limit stigmatisation and increase mental health literacy.
Sub-theme 3.1: stigmatisation
Staff, patient, and broader community perceptions allude to elements of stigmatisation. Staff member 5 reflected on how persons from broader communities can be disparaging towards persons who live with a mental illness: ‘Names will call that person, even the children, don’t go too nearby, because he or she is mad, you know, which is not good’. Several staff members reported assisting mental health patients quite quickly to avoid disruptive behaviour in the clinic ( ‘We will usually help mental health patients first because they do become irritable at a point, where they can’t wait for two hours’ (Staff member 10). Furthermore, staff member 1 stated: We just want to treat them and go home; we want to give them treatment and go home, so really, if we truly face it like that, we don’t care for them that much. . . There’s still discrimination, there’s still discrimination, especially with us in the primary healthcare . . . I wish these nurses could do this client, and it must go home because he or she is going to beat us. So, I think we are not truly prioritising it, like other programmes.
The above extract candidly describes some attitudes towards mental health patients and that some staff might have misconceptions regarding their safety when supporting mental health patients. As a result, mental health care services remain too narrowly focused. Staff member 12 reported, ‘The only thing that we think of is this person getting [a] grant? If not, let’s apply for a grant for him. That’s how far we go with mental illness’. Staff member 1 highlighted the importance of adequately prioritising mental health in PHCs and reported that ‘mental illness needs to be looked at properly because it’s not our priority’. The extracts mentioned above candidly reflect how mental health service is perceived, yet they also express a concern regarding the importance of prioritising mental health services at PHCs.
Sub-theme 3.2: Mental health literacy and promotion
Staff and patients highlighted the importance of ‘education’ about mental health in communities and how it could enable a more supportive and tolerant environment towards mental health care at PHCs. Staff member 5 stated, ‘We need to educate our community so that they can be aware, and also they must support those on treatment’. Several of the staff reported that health education is presented on various health conditions, such as HIV and TB, at the clinics and within the communities. Yet, no clear programmes exist about mental health within PHCs. Staff and patients identified education as a crucial factor for overcoming negative community perceptions of mental health. Staff member 5 stated: Our community, they are not aware of mental illness because, you know, we are at a black community . . . where there are beliefs and misconceptions of other illnesses, you know. So, if someone had that behaviour or acted strangely, they will say, no, it’s a cultural problem that needs cultural medicine, you know, herbal all those things. So I think they are not aware of mental illness, you know.
The extract illustrates two key points. First, staff allude to the importance of education about mental health, which is necessary within and across all communities as well as equipping community members with the necessary information to know when, and how, to seek assistance. Second, education on mental health is an important addition to cultural understanding, and both should be prioritised to enable communities to integrate and understand that cultural understanding and mental health can be understood in a complementary fashion. Staff member 10 summarises the current state of and needs required to make mental health services at community level more progressive: I think mental health services need more awareness on a community level. I think we can participate perhaps more in the actual mental health day. . . They do HIV campaigns all the time. You’ll see there’s a campaign for measles. There’s a campaign for vitamin A, but not that much for mental health. It’s like, okay, we know there’s a need, but you keep quiet about it. Now it’s okay. We know that person is mentally ill, and it’s fine, but we need, to elevate the awareness.
The extract illustrates that long-standing issues, such as physical health conditions (i.e., metabolic syndromes, such as hypertension), receive more attention than mental health. As a result, it would appear that there is an acknowledgement of mental health within communities and PHCs, but no clear effort is made to improve mental health services.
Discussion
Our study explored the perceptions of mental health services among staff and patients at PHCs, to gain insight into the challenges, barriers, services, and opportunities within this area of health services. The findings suggest that patient experiences of PHCs in a resourced-constrained setting remain complex. The complexities that staff and patients have to navigate between themselves also stem from broader systemic factors. Ecological systems theory (Bronfenbrenner, 1979; Crawford, 2020) elucidates the interrelated and interdependent nature of the different systems (i.e., micro, mesosystem, exosystemic, macros, and chronosystem) and how these systems interact and affect the development and functioning of a person (Crawford, 2020). Our findings highlight that patients, staff, and PHCs should be understood from an interdependent systems perspective, within a resource-constrained context.
Considering the challenges, our findings also suggest an opportunity for PHCs to fulfil a larger supportive function within communities and expand the position of PHCs not only to health care but also to be a beacon of support within communities. We found that understanding and providing mental health services is mainly from a pharmacological framework and that perceptions among staff and patients towards mental health and patients living with mental health difficulties, are stigmatised and mostly not prioritised in PHCS. Our findings align with the extant literature on mental health care in PHCs. This said, the study suggests that current mental health care at a primary care level is limited and that integrating mental health care at a primary care level is necessary (Dunlop et al., 2024; Petersen et al., 2019).
Patient reflections and care experiences at PHCs presented a more complex understanding of how patients need to navigate the challenges of limited infrastructure and tardy services. Research on patient experiences and perceptions of health care services at PHCs appear to be influenced by several factors. A qualitative study by Kelly et al. (2019) explored the experiences of older persons accessing primary health care across diverse socio-economic settings in Cape Town. The authors found that patients accessing care in resourced settings had fewer challenges than those in low-resourced communities, who had less trust in the services and felt that staff did not meet their needs. A study by Harrichandparsad and Mahomed (2021) found a higher level of positive (n = 369) experiences among patients who received care at PHCs, compared to community health centres in KwaZulu-Natal. Moreover, there was a non-significant association between ideal PHCs and positive patient experience. Yet, from a micro-systems perspective, our findings highlighted how limited resources and infrastructure in PHCs can impact the experiences of staff and clients as well as influence the interpersonal interactions between staff and patients within resource-constrained settings.
Several contextual circumstances (i.e., limited clinic resources) and interpersonal factors (i.e., staff-patient interactions) influence patient experiences and perceptions of services at PHCs. Our findings highlighted difficult contextual and interpersonal experiences, but in the case of Harrichandparsad and Mahomed’s (2021) study, there appears to be opportunities for positive experiences at PHCs. These positive experiences require further study and understanding to enhance the factors found in Harrichandparsad and Mahomed’s (2021) research. As found in our study, PHCs can fulfil a larger function within communities, providing more than just a service; they can also act as a place of support and compassion to the broader community. The purported broader role that PHCs can fulfil can be conceptually understood at the mesosystemic level, as PHCs can go beyond only service to patients but to other community microsystems (i.e., schools or non-profit organisations) (Crawford, 2020).
Staff and patient understanding of mental health care were primarily underpinned by a pharmacological approach, namely, dispensing of medication and hospitalisation when necessary. Using a purely biomedical approach to the conceptualisation and treatment of mental health has received much criticism and has resulted in a stronger focus on a more integrative approach (i.e., Clark, 2014; Ventevogel, 2014). As a result, in recent years, global mental health initiatives have shown how mental health care requires more collaborative and integrated approaches to improving access to primary mental health care (Petersen et al., 2019; Ventevogel, 2014).
Over the last decade, scalable psychological interventions have been developed and implemented in low-resource settings. A systematic review by Singla et al. (2017), found that psychological interventions for common mental disorders are first-line treatments. There has been an increase in scalable disorder-specific and trans-diagnostic psychological interventions to treat multiple problems within individuals and groups. Interventions, such as Problem Management Plus and Group Problem Management Plus (WHO, 2016), among other interventions, are trans-diagnostic, low-intensity interventions that can be implemented by lay persons within community settings. Furthermore, implementation strategies, such as task-sharing have brought about a change in how the implementation of mental health interventions is to be considered. Task-sharing is deemed a pivotal implementation strategy to improve access to mental health care in LMICs (Booysen et al., 2024; Kaminer et al., 2024).
As stated in our results, mental health is not prioritised by the services at PHCs. The lack of prioritisation and a narrow pharmacological focus limit the overall health care services provided by PHCs. Arguably, stigmatisation and discriminatory behaviour towards mental health services and patients are perpetuated as a result of a lack of service integration and mental health education. A systematic review by Heim et al. (2020) found that existing research on interventions to reduce stigma and discriminatory behaviour at PHCs in LMICs are inconclusive and require more robust research designs that include cultural adaptations for mitigating stigmatisation. A study conducted in the Eastern Cape Province on experiences and perceptions of mental health care at a PHC highlighted the importance of mitigating stigma through collaborative PHC and community interventions (Booysen et al., 2021). Most of the staff reported that PHCs do not prioritise mental health and that no clear programmes exist to increase mental health awareness. At a mesosystemic level, which is the interaction between the PHCs and other microsystems, such as families and organisations, barriers, such as stigma can be addressed by means of specific programmes.
Mental health literacy (MHL) has been identified as a central process and intervention to equip communities and health professionals perceive mental health distress from an informed position, and to seek or provide the necessary preventive and curative steps regarding mental health (Ganasen et al., 2008; Jorm, 2012). A recent cross-sectional study investigated MHL among health care staff in South Africa and Zambia, and found moderate levels of MHL among PHC staff and that MHL requires improvement among staff in PHCs (Korhonen et al., 2022). In our study, MHL among staff and patients appeared low, yet this was not assessed. Considering the prevalence of mental disorders in South African society and limited access to evidence-based and integrative care, MHL is a crucial step to equip communities and staff to understand better the nature and treatment-seeking options for mental health difficulties.
South Africa’s Mental Health Policy Framework (2023-2030) highlights several key focus areas, such as improved financing for mental health care, addressing stigma, implementing task-sharing initiatives, cultivating community resources, and developing mental health promotion programmes (Department of Health, 2023). Our findings align with several key action areas, yet the extant literature highlights a broader governmental apathy to implement long-standing recommendations (Lund, 2023). Considering the findings we have discussed, future studies should endeavour to better understand the complex experiences and perceptions of services at PHCs and attempt to expand the understanding of facilitators associated with positive PHC experiences. For instance, using implementation science methods can assist in implementing and terminating relevant service strategies (e.g., mental health promotion programmes). Second, broadening mental health care at PHC levels is important, and including task-sharing interventions that include active community involvement to increase MHL and psychosocial service is crucial. For example, community health workers could also be trained and supported to implement low-intensity psychosocial skills training interventions at the PHC level. Finally, increasing MHL among staff and patients will equip them to understand better what is needed to address mental health difficulties. The increase of MHL aligns with the MHPF action area of mental health awareness and addresses the pervasive impact of stigma within communities. The study is also limited in several ways; for example, we were unable to conduct interviews with stakeholders at a higher provincial level, and interviews were conducted only with persons at PHCs and not the broader community.
Conclusion
While global efforts to prioritise and improve mental health care are evident, challenges within low-resourced settings in LMICs, such as South Africa, remain. This research emphasises the multifaceted perceptions of mental health services among staff and patients at primary health clinics (PHCs) in an under-resourced municipality of the Eastern Cape Province in South Africa. The findings underscore the complexity of patient experiences and the potential for PHCs to serve as critical community support centres. Despite global efforts to address mental health difficulties through scalable psychological interventions, our findings reveal a predominantly pharmacological approach to mental health care as well as continued mental health stigma and discrimination. Integrative approaches to mental health care and enhanced mental health literacy are imperative to address these challenges. Research should prioritise understanding the nuances of PHC experiences; expanding mental health care provision; addressing mental health literacy interventions, and enhancing stakeholder engagement.
Footnotes
Acknowledgements
We want to acknowledge the participants for participating and sharing their unique experiences as trauma survivors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We also acknowledge the financial funding provided by the University Capacity Development Grant.