
Abstract
Background:
Premature ejaculation (PE) is a common sexual disorder. The profile of subjects seeking treatment of PE in India has not been reported earlier.
Objective:
To study the sociodemographic and clinical profile of subjects presenting with the complaint of PE.
Material and Methods:
The subjects presenting with the complaints of PE were recruited from a specialty psychosexual OPD in the department of psychiatry of a tertiary care center in North India. The subjects were assessed on semistructured proforma, MINI-International Neuropsychiatric Interview, version 7.0, the Diagnostic and Statistical Manual of Mental Disorders, Premature Ejaculation Diagnostic Tool, Arizona Sexual Experience Scale, Hamilton Rating Scale for Depression, and Hamilton Rating Scale Anxiety, Sexual Health Inventory for Men, and Short Form-36 Health Questionnaire.
Results:
A total of 102 subjects were selected after screening 148 cases attending OPD with the complaints of PE after applying selection criteria. The mean age of the sample was 32.17 years (± 8.11). Most of the subjects were married (80.4%), cohabitating with partners (70.6%) and living in the rural area (53.9%). The mean age of onset was 28.29 years (± 7.83, range 17–53), and the mean duration of illness was 3.87 years (± 5.49, range 0.5–31). Prevalence of sexual, psychiatric, and medical comorbidities was 60.8%, 16.7%, and 29.5%, respectively. Emotional role functioning, energy, and general health were the most adversely affected domains of health-related quality of life.
Conclusion:
Most of the men in this study of PE subjects seeking treatment were married young adults. The individuals typically had moderate to severe PE. Comorbidities are prevalent, and roughly two-thirds of people have another medical, psychiatric, or sexual dysfunction.
Introduction
In clinical practice, one of the most typical male sexual dysfunctions seen is premature ejaculation (PE). Premature ejaculation was the most prevalent sexual disorder in men reported in global research, and it was most common in Asians, Central/South Americans, and non-European Western grouping. 1 Although PE has been acknowledged in literature for a while, its frequency has remained unknown. The epidemiological data that are now accessible are inconsistent in nature, making it difficult to assess it on a global basis. A component in the differing statistics has been the use of various definitions and diagnostic standards over time. Premature ejaculation prevalence in the community apparently ranges from 5% to 40%.2,3 An epidemiological study of sexual disorders in south Indian rural population found that PE was prevalent in 8.76% of the subjects. 4
Recently, efforts have been made to standardize terminology and diagnostic standards in order to better understand the scope of the issue. The following definitions for PE were put forth by the International Society for Sexual Medicine Ad-hoc Committee in 2014. 3 Premature ejaculation is characterized by the inability to delay ejaculation on all or nearly all vaginal penetrations, ejaculation that always or nearly always occurs before 1 minute of vaginal penetration (lifelong PE), or a clinically significant and bothersome reduction in latency time, often to about 3 minutes or less (acquired PE), and negative personal consequences such as distress, bother, frustration, and/or the avoidance of sexual intimacy. 3 The Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) defined the PE as a “persistent or recurrent pattern of ejaculation occurring during partnered sexual activity within about one minute following vaginal penetration and before the individual wishes it.” 4
In epidemiological research conducted around the world, PE is linked to several sexual comorbidities.1,5–7 However, a lot of such variables are influenced by the sociocultural and demographic milieu. It is difficult to find a profile of PE subjects in India, who are seeking therapy. In this study, Indian men who complained of PE in a specialized sexual OPD were examined for sociodemographic variables and clinical correlations.
Methods
Participant Characteristics
Subject enrollments were voluntary, following written informed consent without any compensation. Subjects above 18 years, who were in a heterosexual or bisexual relationship and had sexual intercourse in last 6 months presenting to a specialty sexual medicine OPD in a tertiary care hospital in north India, were included. Subjects with organic mental disorder, psychotic disorders, and intellectual subnormality were excluded. Subjects receiving medications that were likely to interfere with sexual functions during past 1 month and those with acute intoxication and withdrawal of psychoactive substances at the time of assessment were also excluded.
Study Design and Procedure
This was a cross-sectional study. The study was approved by the institutional ethics committee (Registration no. ECR/262/Int/UP/2013/RR-16). Detailed medical history and sexual history were obtained, and physical examination was done in the initial evaluation. Information was collected on semistructured proforma for the subject. Psychiatric diagnoses were made using DSM-5. 8 MINI-International Neuropsychiatric Interview, version 7.0 9 was applied on the subject to rule out comorbid psychiatric illness requiring priority treatment. On the subjects, the Premature Ejaculation Diagnostic Tool 10 was used. It is a quick and simple questionnaire with 5 questions that evaluate answers using a Likert scale with a maximum of 5 points (0–4). Scores between 8 and 11 denote PE, 9 and 10 denote likely PE, and 11 denotes PE. To evaluate sexual dysfunction, the Arizona Sexual Experience Scale (ASEX) 11 was used. A 6-point Likert scale is used in the 5-item self-report inventory known as ASEX. Regardless of sexual orientation or relationships with partners, it assesses sexual function in both men and women. Clinical sexual dysfunction is related to an ASEX total score greater than 19, a score greater than 5 on any 1 item, or a score lower than 4 on any 3 items. In order to assess the severity of the symptoms of depression and anxiety, respectively, the Hamilton Rating Scale for Depression (HAM-D) 12 and Hamilton Rating Scale for Anxiety (HAM-A) 13 were used. To examine and identify any co-occurring erectile dysfunction (ED), the Sexual Health Inventory for Men 14 was used. On a 5-item Likert scale, its 5 questions measure the reaction (1–5). Erectile dysfunction is identified as having a score below 22. A health-related quality of life assessment was conducted using the Short Form-36 (SF-36) Health Questionnaire. Assistance in interpretation and responding during filling of the rating scales was provided to the subjects, if asked by the subjects. Investigations such as hemogram, thyroid function test, random blood sugar, serum lipid profile, and serum testosterone were done.
Statistical Analysis
The data collected were tabulated using computer software and statistically evaluated using Statistical Package for the Social Sciences (SPSS version 16.0). Descriptive statistics were used to calculate means, standard deviation, and frequencies. Data were expressed as the mean and standard deviation or number (percentage) when appropriate.
Results
To choose 102 participants in the study, a total of 148 subjects were evaluated. Subjects who had their last sexual encounter more than 6 months ago were the most often cited reason for nonselection (n = 15), followed by examinations that were not completed (n = 13). Other causes were receiving medicines likely to interfere with sexual function (n = 8), having never had a sexual experience (n = 6), having a mental disease (n = 3), and being homosexual (n = 1). The mean age of the sample was 32.17 years (± 8.11). Most of the subjects were married (80.4%), cohabitating with partners (70.6%), living in a rural area (53.9%), Hindu, and belonged to a nuclear family. About 40% of them were educated till graduation or above. Most of the subjects were working and earning, and the mean income of the sample was ₹18,318 (Table 1).
Sociodemographic Profile of Subjects.
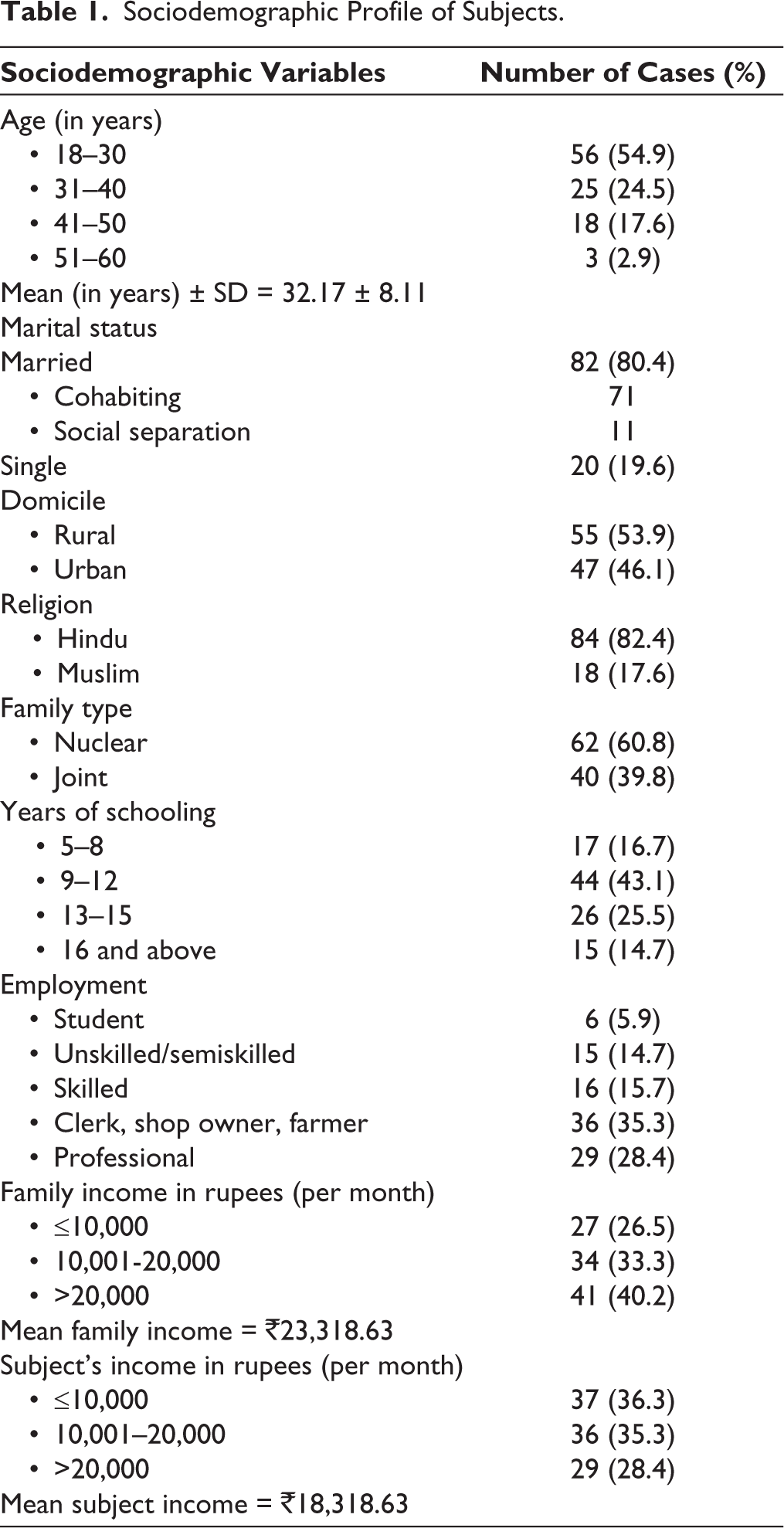
The mean age of onset was 28.29 years (± 7.83, range 17–53), and the mean duration of illness was 3.87 years (± 5.49, range 0.5–31). About half of the subjects had a duration of illness of more than 3 years. One-third of the subjects had tobacco use disorder (harmful use = 9.8%, dependence = 28.4%). Reported per month frequency of intercourse was ≤5 in 48.1%, 6 to 10 in 33.3%, and >10 in 17.6% subjects. Total 91.2% subjects reported to have only 1 sexual partner.
Severity of the PE was assessed as per self-reported intravaginal ejaculatory latency time (IELT) as per the DSM-5 classification. Out of the total subjects, 37.3% had mild (IELT 30–60 seconds), 22.5% had moderate (IELT 15–30 seconds), and 20.6% had severe (IELT <15 seconds). Total 19.6% subjects in the sample had IELT >60 seconds. Data of subjects reporting anteportal ejaculations (AEs) (ejaculations occurring even before vaginal penetration) were also assessed, and 16.7% subjects in the mild severity category, 5.6% in the moderate severity category, and 77.7% subjects in the severe category reported instances of AEs.
Distribution of comorbidities in the sample is reported in Table 2.
Comorbidities in the Sample.
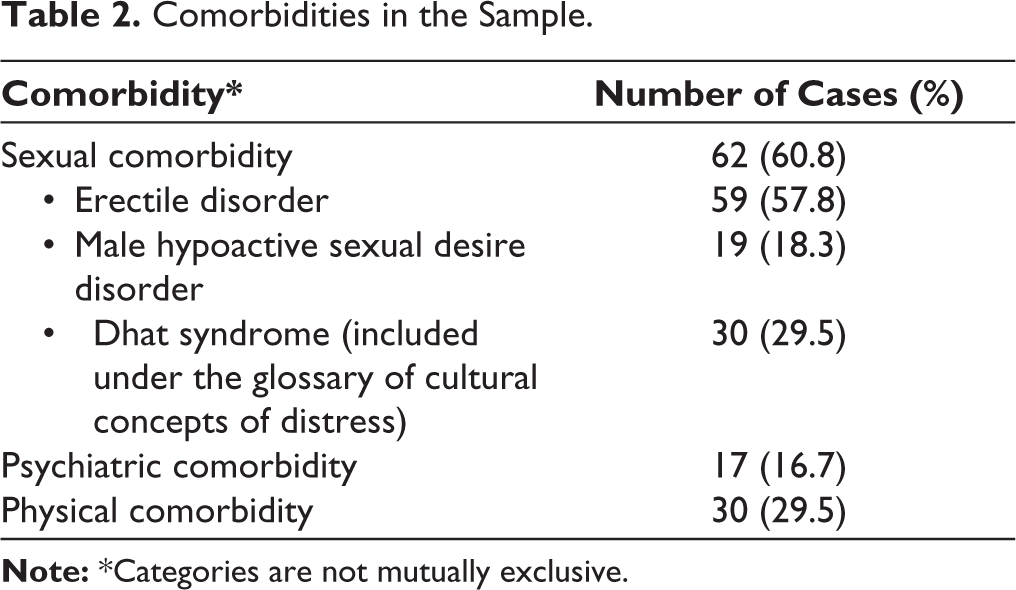
Diagnosable psychiatric comorbidity was present in 16.7% cases (depression: 6.9%; adjustment disorder: 2.9%; generalized anxiety disorder: 4.9%; and somatoform disorder: 1.9%). As per the HAM-D score of the sample, there was no depression in 59.8% cases, mild in 33.3% cases, and moderate in 6.9% cases. No subject had severe/very severe scores as per HAM-D. The anxiety symptoms as per the HAM-A score were normal in 52.9% cases, mild in 35.3% cases, and moderate in 11.8% cases. There were no subjects with severe anxiety symptoms.
The physical comorbidities were present in 29.5% cases and included the deranged lipid profile (11.8%), anemia (18.6%), and hypothyroidism (3.9%). Subjects having hypertension, diabetes, kidney stones, seizure disorder, vitiligo, and primary infertility were 0.9% each.
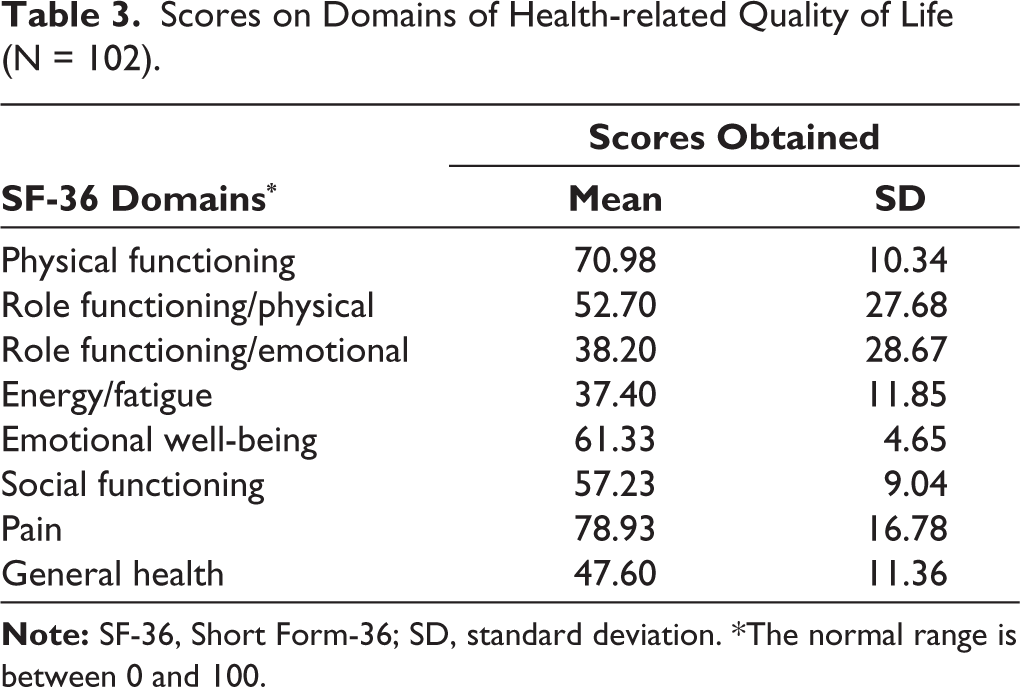
The health-related quality of the sample is reported in Table 3. In comparison with other domains, lower scores were seen in emotional role functioning, energy, and general health.
Scores on Domains of Health-related Quality of Life (N = 102).
Discussion
This was a clinical study to evaluate sociodemographic and clinical profile of subjects presenting with the complaints of PE to a specialty sexual OPD in the psychiatry department of a north Indian tertiary medical university.
The study group comprised 102 subjects out of which more than half (54.9%) were aged between 18 and 30 years, and the mean age was 32.17 years (±8.11). As in countries like India, this age group is the common age group for initiating marital life. Sexual difficulties at this age is considered as a major reason of distress. Hence, people at this age with sexual difficulties often consult doctors. As sexual difficulties adversely affect the marital life, people consult for remedies. Hence, most of our study participants were married (80.4%).
There were only 21 subjects over the age of 40 years, and out of those, 3 were above the age of 50 years. It has been suggested that PE decreases with age, perhaps as a part of learned sexual experience or because of associated physiological changes.2,15 The data available from studies till date present a varied picture. Large-scale studies conducted in a community show that the prevalence remains the same across all age groups. 1 Other studies have shown that men with PE present with a higher age.5,6 On the other hand, some have shown that the risk decreases with aging.7,16 It is to be noted that the aforementioned studies were population based, and our study sample was from a treatment-seeking clinical population. As sexual disorder causes much more dysfunction and concern in early life, treatment-seeking population is younger. With increasing age, even subjects with persistent problems adjust with their dysfunctions, hence may lead to lesser clinical consultations of their problems. So, our sample derived from clinical population was primarily consisting of younger population. Hence, the mean age is expected to be on a lower side.
As per the sociodemographic distribution of the study region, the majority of the subjects were Hindu and belonged to the rural population. Since most of the subjects were married, it can account for a higher number of nuclear families. Results from the National Health and Social Life Survey do not reveal a difference in the prevalence of PE among married or single men. 1 Since premarital sexual exposure in Indian population is not as common in West and marriage provides an opportunity for sexual activities as well, it can unmask sexual problems otherwise hidden within the individual. Thus, it can account for most of the subjects being married in our sample.
The majority (43.1%) had a secondary education, 16.7% had a primary education, and 40.2% were graduates or higher. There is evidence to suggest a negative relationship between education and physical activity. The Global Study of Sexual Attitudes and Behavior study added to this finding. 1 It is proposed that the increased prevalence of PE in less educated men can be explained by the assumption that one’s educational status influences one’s health status. Simply put, people with more education have a higher quality of life, including better emotional and physical health, and are thus less likely to experience PE.
This finding was also supported by a Turkish study that discovered an increased frequency of PE in men with lower levels of education. 6 Considering the general lack of education in our country, the study sample was fairly educated.
In our study, the subjects were mostly farmers, clerks, or shop owners with a monthly income, which can be explained by the level of education in the majority of the sample, as described above. Again, because occupation and income have a direct impact on lifestyle and health, lower socioeconomic status leads to a higher prevalence of PE. This comparison is also biased because of the difference in the health systems across countries. Access to health care, especially sexual health, is significantly limited and difficult because of out-of-pocket expenditure and monetary concerns involved with treatment. Most common consultation seeker of public health institutions in India remains lower- or middle-class population. Upper-class population typically prefers private sector consultations for their medical problems.
Subjects had a long duration of illness with most of the subjects had a duration of more than 3 years. There can be several contributors for this delay in seeking treatment for subjects with PE. Some of the men presented after a long-standing illness can be attributed to the deficient health infrastructure of our country. Poor availability of treatment centers and lack of adequate expertise in sexual medicine among clinicians remain an area of concern. Also, a minor contribution can be of the conservative nature of Indian society where men are hesitant to discuss their sexual problems out of shame, thus their reluctance to seek treatment. Lack of proper sexual education and prevalent sexual myths in the society further complicate the problem.
Around 40% of study subjects consumed some kind of substance. Since the study excluded intoxicated and withdrawal state subjects, those with dependence and harmful use pattern were taken. Alcohol and tobacco being the most commonly used substances in Indian population, data were collected keeping them in mind. Tobacco dependence was found to be most commonly associated (28.4%) with PE. Substance use has been linked to PE in few studies, which indicates a higher smoking and alcohol consumption rate in men with PE.5,7 Higher rates of physical illnesses, such as neurological and vascular disorders that are implicated in the etiopathogenesis of acquired PE (APE), are the likely contributors of PE in such men.
The severity of PE in the study was judged as per the self-perceived IELT and using the DSM-5 criteria. Anteportal ejaculation, which refers to ejaculation before penetration, was present in 18 of the subjects. Fourteen of those subjects belonged to the severe category. Around half of the subjects had moderate to severe PE as per the DSM-5 score.
Premature ejaculation is frequently associated with a variety of sexual, psychiatric, and medical comorbidities. As per the data available from population-based studies, men with PE are likely to have more comorbidities than those without PE.5,6 The distribution of comorbidities in our study was sexual (60.8%), followed by physical (29.5%), and psychiatric (16.7%). Among the sexual comorbidities, the most common was erectile disorder (ED) (57.8%). Various studies have also reported that ED is a common comorbidity associated with PE. 17 Erectile disorder has been recognized by a few authors as the single greatest risk factor for PE. 18 Total 18.3% of the subjects also had male hypoactive sexual desire disorder that could explain the lower sexual intercourse frequency in some. Now, it must be noted that this disorder might be a consequence of the disorder itself, resulting out of distress and anxiety related to early ejaculation. Dhat syndrome, a Southeast Asian culture-bound syndrome, was also found in men with PE; however, no link between the 2 disorders has been established as yet. Dhat syndrome causes subjects to be extremely anxious and overly concerned about their health and sexual lives. Significant anxiety in Dhat syndrome subjects may impair sexual performance. An Indian multicentric study looking for sexual comorbidity in Dhat syndrome subjects discovered PE in 32.4% of the cases. 19 Anxiety and depression are the most commonly reported psychiatric symptoms in subjects. Previous research has also found a link between anxiety and depression and PE. 20 Anxiety and depression are the most common stress reactions. This could explain why anxiety and depression were observed in the study population. Anxiety has frequently been proposed as a cause of rapid ejaculation, with several types of anxiety being blamed for the disorder, including trait anxiety. 15 Anxiety in general appears to be a significant risk factor for PE. Dunn et al 21 discovered a strong link between anxiety and PE in a large study. The common medical comorbidities reported in our samples are anemia, dyslipidemia, and thyroid dysfunction (hypothyroidism). These medical comorbidities are probably chance findings depending on the commonalities of these medical dysfunctions in this region. Deranged lipid profile has not been found to be associated with PE in earlier studies also. 21 The hyperthyroidism has been reported associated with PE in earlier reports. 22
The mean scores on domains of SF-36 to assess the health-related quality of life revealed relatively lower scores in domains of emotional role functioning, energy, and general health signifying poor quality in these domains than other domains. These findings can be explained by the fact that most other domains assess quality affected by physical functioning that remains unaffected in PE. Poor general health is an indicator of poor sexual functions, and resultant distress might result in lower scores in emotional role functioning. Emotional problems and stress may be both a risk factor for and a result of sexual dysfunction, particularly PE.
Limitations
The study population was selected from treatment-seeking subjects at a specialty sexual OPD of a tertiary center; hence, one should be cautious in generalizing the finding. The sample size was small. It was a cross-sectional study; hence no cause-and-effect relationship can be ascertained among factors.
Conclusion
In this study of treatment-seeking subjects with PE, most of the men are married young adults. Typically, the subjects were suffering for several years and had moderate to severe PE. The rates of comorbidities are high and about two-thirds have another sexual disorder or medical illness.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the institutional ethics committee (Registration no. ECR/262/Int/UP/2013/RR-16).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.