
Abstract
Abstract
Introduction: Premature ejaculation is a complex condition with controversial management modalities. We decided to assess the treatment-seeking behavior of affected couples, which is an indirect indicator of the efficacy of the present management modalities of premature ejaculation.
Materials and Methods: Couples, who reported premature ejaculation at our outpatient clinics between January 2015 and December 2016, were enrolled in the study. Patients with acquired causes for premature ejaculation were excluded. Both the partners were administered premature ejaculation diagnostic tool (PEDT) questionnaire separately at the time of initiation of the study and after 1 month. They were asked to report intravaginal ejaculatory latency time (IELT) and their treatment-seeking behavior at these time intervals. The couples were counselled regarding their diagnosis and offered treatment with dapoxetine 30 mg as and when required.
Results: A total of 117 couples with an average married life of 5.4 years were enrolled for the study. Among these, 68 had premature ejaculation (PE), 30 had probable PE and 19 had no PE as estimated on PEDT. Post treatment, 55% of couples with PE, 47% of couples with probable PE and 55% of couples without PE wanted to continue treatment seeking despite improvement. Female partners had the desire to seek treatment despite the male partner reporting otherwise.
Conclusion: The treatment seeking behavior of the affected couple indicates the inefficacy of the present management modalities of PE. As specialized health care providers, we need to address these concerns to provide a comprehensive solution to their problems.
Keywords
Introduction
Premature ejaculation (PE) is the most common sexual dysfunction in males. According to International Society for Sexual Medicine (ISSM), PE is defined as the ejaculation that occurs within a minute of vaginal intromission, without the control of the ejaculating male associated with distress in the affected couple. 1 This describes lifelong PE, wherein it is reported from the very first sexual act. 2 This describes our study population as well because our patients also reported PE from their first sexual encounter.
The criteria of 1 minute brands 95% of the population as normal, though the reported incidence of PE is 30%. 3 As one can make out, the definition itself fails to define the affected population comprehensively. In such a scenario, the diagnostic methods as well as treatment modalities based on this definition are unlikely to address the issue comprehensively. As a result, the affected men are left with no other options than seeking treatment from all available options, which include modern medicine, traditional medicine, Ayurveda, Unani, homeopathy, etc. Most of the time, the affected couples remain dissatisfied despite trying all the options. Failure to address the issue in a comprehensive manner indirectly paves the way for quackery as well. Treatment-seeking behavior of the affected couple indirectly speaks about the efficacy of the present modalities of available treatment for PE. Hence, we decided to assess the treatment-seeking behavior of the affected couple, which is an indicator of the efficacy of the present diagnostic and therapeutic modalities available in modern medicine.
Materials and Methods
After obtaining written informed consent and institutional review board approval, couples reporting to our outpatient department with the complaints of PE between January 2015 and December 2016 were enrolled for the study. Among these, the patients with erectile dysfunction, thyroid disorders, prostatitis, or relationship problems were excluded from the study. Premature ejaculation diagnostic tool (PEDT) was administered to all the enrolled couples. PEDT is a validated questionnaire developed by Symonds et al. 4 There are 5 questions, to which there are 5 possible responses each. Each response is given a score from 0 to 4, based on the answers chosen by the participants. The questions refer to male partner’s perceived difficulty in delaying ejaculation, frequency of ejaculations which occur despite male partner not willing to ejaculate, ejaculation that occurs with minimal or no stimulation, feeling of frustration due to the early ejaculation, and the female partner’s dissatisfaction, respectively. By adding the responses to the 5 questions of the tool, the final score is calculated. If the final score is 8 or less, it indicates no PE. If the final score is more than 8, but less than or equal to 10, it indicates probable PE. If the final score is more than 10, it indicates PE. Both the partners involved in the sexual act were administered PEDT questionnaire separately and independent of each other at two separate time intervals, first at the time of initiation of the study and the second after 1 month. They were asked to report intravaginal ejaculatory latency time (IELT) and their treatment seeking behavior at these fixed time intervals. These were also recorded in both the partners separately and independent of each other.
Initially, the couples were counselled to assess their understanding of PE and also to rule out any other sexual dysfunction in both the partners. Based on their PEDT score, the couples were counselled regarding their diagnosis, and as part of the counselling, patients were provided an insight about their condition. All the couples were counselled by only 1 professional counsellor in an outpatient setting with adequate privacy. They were offered pharmacological treatment in the form of dapoxetine 30 mg as and when required. All the treatments were supervised by only 1 urologist/sexual medicine consultant.
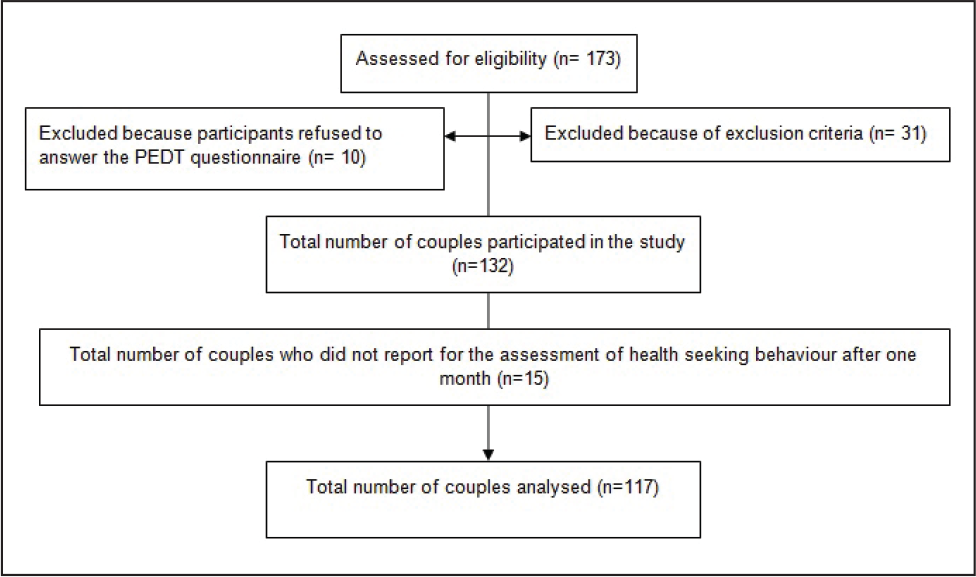
Treatment-seeking behavior of the 117 couples was analyzed (Figure 1). Those having PE and probable PE were counselled and pharmacotherapy was provided in the form of dapoxetine 30 mg. Couples, in whom PE was ruled out on PEDT, were offered counselling as part of the treatment, wherein the insight was provided regarding their condition. At the initiation of the study, all the 117 couples were asked to report the reason for seeking treatment. All these couples were again enquired as to whether they would like to continue seeking treatment at the end of the completion of the treatment. They were also enquired as to specify reason for continued treatment-seeking despite improvement in IELT or PEDT score or both.
Results
Average married life of these couples was 5.4 years. Mean age of the male partner and female partner were 34.44 years and 29.42 years, respectively. Of the 117 couples, who answered PEDT questionnaire, 68 had a score of more than 10, hence diagnosed as having PE and grouped as premature ejaculators. A total of 30 couples had a score of more than 8, but less than or equal to 10 on PEDT questionnaire, hence diagnosed as having probable PE and grouped as probable premature ejaculators. A total of 19 couples had a score of 8 or less on PEDT questionnaire, hence diagnosed as having “no” PE and grouped as “no” premature ejaculators. The correlation between the diagnosis based on the reported IELT at the beginning of the study and the diagnosis based on the PEDT was poor, especially when the IELT threshold was taken at 1 minute.
Mean ages of the male and female partners were 33.88 years and 28.84 years, respectively, in the premature ejaculators group; 35.1 years and 30.3 years, respectively, in the probable premature ejaculators group; and 35.42 years and 30.11 years, respectively, in the “no” premature ejaculators group. Average married life was 4.93 years, 6.2 years, and 5.79 years in the premature ejaculators group, probable premature ejaculators group, and “no” premature ejaculators group, respectively.
Mean pre-treatment self-reported IELT as reported by the male and female partners were 2.69 minutes and 2.21 minutes, respectively, in the premature ejaculators group; 3.93 minutes and 3.63 minutes, respectively, in the probable premature ejaculators group; and 4.05 minutes and 3.63 minutes, respectively, in the “no” premature ejaculators group. Mean post-treatment self-reported IELT as reported by the male and female partners were 3.28 minutes and 2.57 minutes, respectively, in the premature ejaculators group; 4.23 minutes and 3.43 minutes, respectively, in the probable premature ejaculators group; and 4.37 minutes and 3.58 minutes, respectively, in the “no” premature ejaculators group.
Mean pre-treatment PEDT score as reported by the male and female partners were 12.04 and 12.18, respectively, in the premature ejaculators group; 8.57 and 8.83, respectively, in the probable premature ejaculators group; and 7.11 and 7.58, respectively, in the “no” premature ejaculators group. Mean post-treatment PEDT score as reported by the male and female partners were 10.26 and 11.46, respectively, in the premature ejaculators group; 8 and 8.97, respectively, in the probable premature ejaculators group; and 7.42 and 7, respectively, in the “no” premature ejaculators group.
A total of 98 couples, which included 68 couples from the premature ejaculators group and 30 couples from the probable premature ejaculators group, were treated with both counselling as well as pharmacotherapy by dapoxetine 30 mg. A total of 19 couples who were diagnosed as having “no” PE on PEDT were counselled about their condition. No pharmacotherapy was offered to these 19 couples. All the 117 couples answered PEDT questionnaire again after undergoing treatment. They reported IELT again at the end of the treatment.
The female partners always reported IELT lesser than their male partners, both at the beginning as well as at the end of the study. The same was true with PEDT score, wherein the female partners always reported higher score when compared to the scores reported by the male partners.
Among the male partners, 40% belonging to the premature ejaculators group, 37% belonging to the probable premature ejaculators group, and 47% belonging to the “no” premature ejaculators group wanted to continue seeking treatment despite an improvement in either the IELT or PEDT score, or both. Similarly, 69% of the female partners in the premature ejaculators group, 57% of the female partners in the probable premature ejaculators group, and 63% of the female partners in the “no” premature ejaculators group wanted to continue seeking treatment despite an improvement in either the IELT or PEDT score, or both. All these couples felt that improvements in IELT and PEDT score are mere numbers. All of them felt that their concern is not just prolongation of ejaculatory latency. All of them wanted to achieve a status wherein both the partners achieve the orgasm simultaneously, irrespective of the ejaculatory latency. They wanted to continue seeking treatment till such a thing is achieved. Female partners were more in favor of seeking treatment, though their male counterparts felt that they are satisfied with the treatment or counselling, or both.
Discussion
We evaluated the treatment-seeking behavior of the couples affected by PE to assess the efficacy of present management modalities of PE. The study revealed that majority of the couples wanted to continue seeking treatment despite improvement in IELT or PEDT score after the standard treatment. The female partners were more inclined to continue health-seeking compared to the male partner.
Though the PE is the most common sexual dysfunction in a male, even today it remains the least understood condition with vastly varied definitions. 5 There have been various attempts to comprehensively define a complex condition like PE without much success. In order to achieve objectivity, ejaculatory latency was included in the ISSM definition. Along with ejaculatory latency, ejaculatory control was of much concern for the affected couple. Giuliano et al showed that it was the perceived control over ejaculation that was more important than the IELT which had significant effect on ejaculation-related distress and satisfaction with sexual intercourse. 6 The concern of our patients was also more about their inability to delay ejaculation enough, suggesting lack of control over ejaculation. This further supports the view that PE is more of an uncontrollable early ejaculation rather than a simple early ejaculation. Measurement of ejaculatory control is most of the time subjective. Lack of objectivity in measuring ejaculatory control adds to the ambiguity of the definition of PE. Lack of control over ejaculation results in frustration in the couple and resultant performance anxiety in the male partner compounds the lack of control further. Hence, we need an objective tool to measure the control over ejaculation, which further helps in defining the disorder of PE better. IELT was expected to be surrogate marker for ejaculatory control. Contrary to the expectation, there is poor correlation between the IELT and ejaculatory control as shown by Grenier and Byres.7, 8 Though the reported IELT was more than the ISSM definition of 1 minute in our study, more than 65% of the couples who visited us for PE were bothered more about their inability to control ejaculation, clearly confirming the poor correlation between the two. Unless we define an objective tool to assess the lack of control on ejaculation in these patients and use the same in the definition of PE, definition remains incomplete. This is the gap that we need to bridge if we want to address the real issue of PE.
Present diagnostic modalities for PE are based on the ISSM definition. But crux of the problem is the definition itself, which fails to address the issue comprehensively. Hence, logically speaking, the diagnostic modalities based on the present definition are unlikely to address the real premature ejaculators. When we take the IELT of 1 minute threshold for the diagnosis, more than 95% of the population should be normal ejaculators. Contrary to this, the reported incidence is 30%. 2 Similarly, we found that, of the 117 couples who approached us for the complaints of PE, only 30% reported an IELT of 1 minute or less, whereas 70% had an IELT of more than 1 minute, but still complained that they were not happy with their ejaculatory latency. It was important to note that all these males reported early ejaculation from day 1 of their sexual intercourse, suggesting that they are “lifelong” premature ejaculators. When these men, whose reported IELT was more than 1 minute, were explained about the present-day definition of PE, they were of the opinion that sexual satisfaction was not based on the mathematics of IELT alone. Patrick et al reported median ejaculatory latency of 1.8 minutes in premature ejaculators, higher than the defined cutoff of IELT for PE in their observational study of PE. 9 It is amply clear that diagnosis of PE based on a minute cutoff of IELT becomes too exclusive to take it at its face value. Hence, a mere measure of IELT is of no value to assign an intercourse as most satisfactory.
As per Waldinger, those who are found to be normal on present diagnostic modalities for PE, but consider themselves to be suffering from PE, are perceived to be suffering from subjective PE.2, 10, 11 But in clinical practice, these patients seek treatment elsewhere if the treating physician fails to address the issue in a comprehensive manner. This paves way for quackery again. We found that not only “no” premature ejaculators but also the majority of premature ejaculators who reported post-treatment improvement on PEDT and IELT, preferred to continue seeking treatment. This suggests a clear dissociation between the modern therapists’ understanding of PE and the expectations of the patients who report PE. Unless we address the expectations of these patients, our efforts to address the issue of PE remain futile.
Our patients were of the opinion that their concern was more about the dissatisfaction that was experienced by the couple rather than the early ejaculation as an entity. They tended to connect the satisfaction with the ejaculatory latency. Similar outcomes were reported in a survey in Europe.9, 12 In these studies, “climaxing too soon on the part of the men” and “failure to delay ejaculation till the female partner wants” were reported as a cause of dissatisfaction. Similarly, in our study, the female partners wanted to continue seeking treatment, despite the male partners reporting a post-treatment satisfied outcome. This brings another fact to the fore that our target of prolongation of IELT might not address the real issue. Instead, we need to address more complex issues of mutual sexual satisfaction if we need to address the issue of PE comprehensively.
Though PE is a male sexual dysfunction, it becomes a matter of concern for their partners as the condition manifests during the intercourse. Graziottin and Althof have very rightly pointed out that the treatment modalities fail to deliver the desired results unless the treating physician considers and treats the PE as a couple’s problem and not as a problem of male partner alone. 13 Hence, any modality that addresses the concerns of a single partner is bound to be incomplete. We need to address the concerns of both the partners to provide a comprehensive care for PE patients.
Present-day approaches to treat PE is more focused around the male partner and IELT. A wider focus to address the female partner’s concerns and concerns about the ejaculatory control will be a step forward in the right direction.
Conclusion
Complex issue of PE is neither addressed comprehensively nor managed appropriately by the present diagnostic methodologies as well as treatment modalities, thus paving way for dissatisfaction among the couple reporting PE. This dissatisfaction is reflected by their choice of continued treatment-seeking behavior despite appropriate treatment with available treatment methodologies. Instead of aiming at the prolongation of IELT, we need to address the issue comprehensively by looking into the concerns of affected couples.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.