
Abstract
Background:
Erectile dysfunction (ED) is one of the most common psychosexual disorders in clinical practice, and it results in significant distress, interpersonal impairments, poor quality of life, and marital disharmony. However, there is limited research on ED in India. Therefore, this study aimed to assess the sociodemographic and clinical profile of patients presenting with ED.
Method:
Cross-sectional evaluation of patients with ED presenting to the psychosexual outpatient department (OPD) of psychiatry department in a tertiary care hospital was done on structured clinical pro forma, Mini-International Neuropsychiatric Interview, International Index of Erectile Function-5, Arizona Sexual Experience, Hamilton rating scale for depression, and Hamilton rating scale for anxiety.
Results:
The sample included 102 patients. The mean age was 33.38 years. The majority of the patients were married (81.4%), Hindu (82.4%), residing in a rural area (60.8%), and belonging to a nuclear family (62.7%). The majority of the patients had a moderate level of ED (50%) followed by mild-to-moderate ED (26.5%) and severe ED (23.5%). Premature ejaculation (46.1%) and depression (28.4%) were the most common sexual and psychiatric comorbidities. Obesity was common (62.7%), and only a minority had other metabolic dysfunction, namely dyslipidemia (7.8%), diabetes (5.9%), and hypertension (4.9%). Tobacco dependence and alcohol dependence were present in 37.3% and 6.9% cases, respectively.
Conclusion:
Young adults with moderate-to-severe ED were present for treatment at a tertiary center. Comorbidities of other sexual disorders, psychiatric disorders, and substance use are commonly encountered in such patients. Promotion of early help-seeking should be encouraged. Clinicians should thoroughly assess even the young patients for other sexual, psychiatric, and medical comorbidities.
Keywords
Introduction
Erectile dysfunction (ED) has been defined as “the persistent or recurrent inability to attain or maintain an erection sufficient for satisfactory sexual function.’’ 1 ED is currently one of the most common sexual dysfunctions in men worldwide. 2 ED is the chief complaint of more than 50% of all men treated for sexual disorder. The severity of presentation may range from a partial decrease in penile rigidity to a complete erectile failure. This is a severe health problem and has gained public attention in recent times. Prins et al 3 published a systematic review on the prevalence of ED in the general population, which included 23 studies from Europe, USA, Asia, and Australia. 3 A meta-analysis on the prevalence of ED in Asian populations, which included 6 studies comprising 8,653 individuals for analysis, found it to be ranging from 2% to 81.8%. 4 The wide variance in prevalence rates of ED is often attributed to the embarrassment attached to admitting having ED, differences in methodology of studies, use of different tools for assessment, and differences in sample characteristics. Most of the cases have acquired ED, and the lifelong subtype is relatively rare. The lifelong subtype is reported to occur only in about 1% of men under age 35 years. 5
The prevalence of ED has also been studied in association with various comorbidities. A study conducted among patients with hypertension and/or diabetes mellitus involving 7,869 patients found ED in 67% and 71% patients of diabetes alone and hypertension alone, respectively, using IIEF-5. 6 A study conducted in North Indian men with type 2 diabetes found ED in 77.2% of the 348 patients assessed using IIEF. 7 Concerning prostatitis, a Chinese study found ED in 35.1% of chronic prostatitis patients. 8 A retrospective chart review of patients attending psychosexual outpatient department (OPD) in north India reported that ED was the second most common cause of the consultation. About 15% of OPD visits were related to ED. 9
ED is an age-dependent disorder, possibly resulting from physiological changes associated with the aging process.10,11 Earlier studies have reported an increase in the prevalence of ED by 5% to 17% with each passing year in men older than 18 years. The prevalence of ED increases markedly after 60 years of age.3,12 Education and household income are inversely related to ED in some studies. Lifestyle factors and medical conditions partly mediate the effect of socioeconomic status on ED. Higher socioeconomic status has been linked to better health, and better-educated men have physically and emotionally less stressful lifestyles. A low level of education is also a marker of the high prevalence of nondiagnosed diseases, and low income is also often related to higher levels of stress. 13 A high level of stress, anxiety, and depressive symptoms are known to be associated with ED. A bidirectional influence of stress and ED has been proposed. Chronic stress elevates corticosteroid level, which reduces testosterone levels, resulting in difficulties in sexual response and functioning. 14
The sociodemographic and clinical characteristics of treatment-seeking patients for primary ED are still not well researched in India. Therefore, this study evaluated patients’ sociodemographic and clinical profile presenting with ED in a tertiary care marital and psychosexual OPD.
Materials and Methods
The study is a cross-sectional, observational study conducted on patients presenting with ED attending the marital and psychosexual OPD in the Department of Psychiatry at a tertiary care teaching hospital with a large referral area. The study was approved by the Institutional Ethics Committee of the institute.
Study Population
The study sample consisted of 102 male patients who fulfilled the selection criteria. Subjects included were heterosexual or bisexual males with age ≥18 years attending marital and psychosexual OPD of psychiatry department with the complaint of ED, having the experience of sexual intercourse in last 6 months, with the ability to speak and understand Hindi/English, and willing to give written informed consent. The above inclusion criteria kept as the validated tools are available only for heterosexual males.
Patients in acute intoxication and withdrawal of psychoactive substances, with an organic mental disorder, psychotic disorders (schizophrenia spectrum disorders and bipolar disorder), and intellectual subnormality, as well as the patients having psychiatric and medical comorbidities requiring priority medical management were excluded from this study. Patients receiving medications that might interfere with sexual functioning and those unable to cooperate due to any reasons were also excluded from this study.
Data Collection
Patients attending marital and psychosexual OPD in the Department of Psychiatry presenting with complaints of ED were screened for inclusion into the study. Mini-International Neuropsychiatric Interview (MINI 7.0) was applied to the patients to assess comorbid psychiatric illnesses. A physical examination was performed, which included genital and rectal examinations (as clinically indicated). Investigations for metabolic syndrome (blood pressure, lipid profile, blood sugar, and Body Mass Index [BMI]), serum testosterone level, thyroid function tests, hemogram, and urine-routine, as well as microscopy, were performed according to the standard of care. Patients were tested on the same day or at a mutually suitable time later in the week. Demographic profiles and clinical details were collected on semi-structured pro forma for the patient. International Index of Erectile Function (IIEF-5) was applied to patients to diagnose and assess the severity of ED. Patients were then classified into specified subtypes of ED as per IIEF-5 scoring. Arizona Sexual Experience (ASEX) scale was applied to assess sexual dysfunction. Hamilton rating scale for depression (HAM-D) and Hamilton rating scale for anxiety (HAM-A) were applied to check the severity of depressive and anxiety symptoms.
Statistical Analysis
The information gathered was tabulated using software and statistically analyzed using the Statistical Package for the Social Sciences (SPSS version 16). For continuous variables, descriptive tests were performed using mean and standard deviation. In addition, the frequency and percentage of nominal variables were calculated.
Results
The total number of patients screened was 146. Out of these, 102 patients were selected for the study. Out of the patients screened, 44 (30.14%) could not be selected and were excluded. The most common reason for the nonselection was that patients had last sexual intercourse >6 months ago (n = 18), followed by noncompletion of investigations (n = 11), no sexual experience with a partner (n = 9), and patients having psychotic disorder hence could not reliably cooperate with needs of the study and priority was to manage their psychiatric illness earlier (n = 4). Two subjects were homosexual. Rating scales used for this study cannot be reliably applied in the patients not having experience of sexual intercourse with a partner; hence, such patients were excluded.
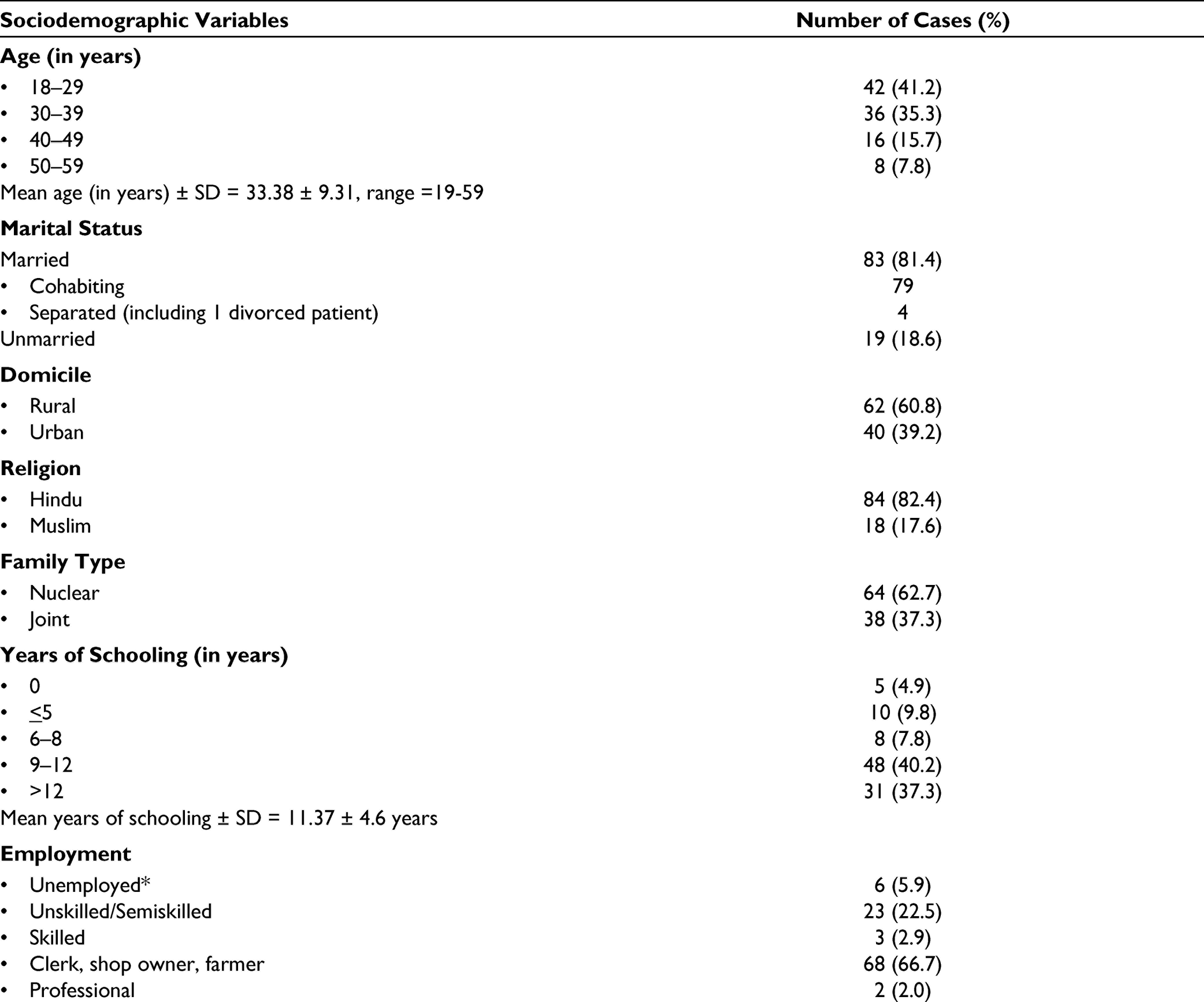
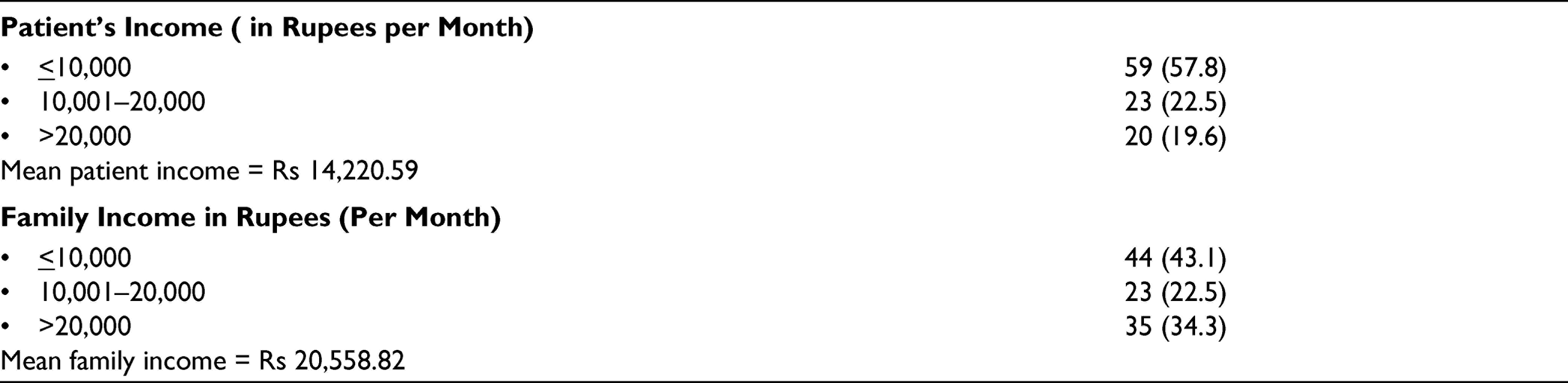
Sociodemographic Profile
Most of the patients were in the age group of 18 to 29 years (mean age 33.38 ± 9.31; Range: 19-59). The majority of the patients were Hindu (82.4%), married (77.5%), and had a nuclear family (62.7%). Most of the patients had 9 to 12 years of schooling (40.2%), were employed as a clerk, shop owners, or farmers (66.7%), and had income below Rs 10,000. The mean patient income was Rs 14,220 (Table 1).
Demographic Profile of Patients (N = 102)
Clinical Profile
The mean years of age of onset were 30.70 ± 8.79 years (range: 15-55 years). The mean years of duration of illness were 1.95 ± 1.10 (range: 0.8-10 years). For most of the patients, the duration of illness was within 1 year (49.0%). Majority of patients were obese (n = 64; 62.7%). The frequency of intercourse per month was ≤5 in most patients (n = 43; 42.2%), and they were mostly in a monogamous relationship (n = 60; 58.8%; See Table 2).
Clinical Characteristics of the Sample (N = 102)
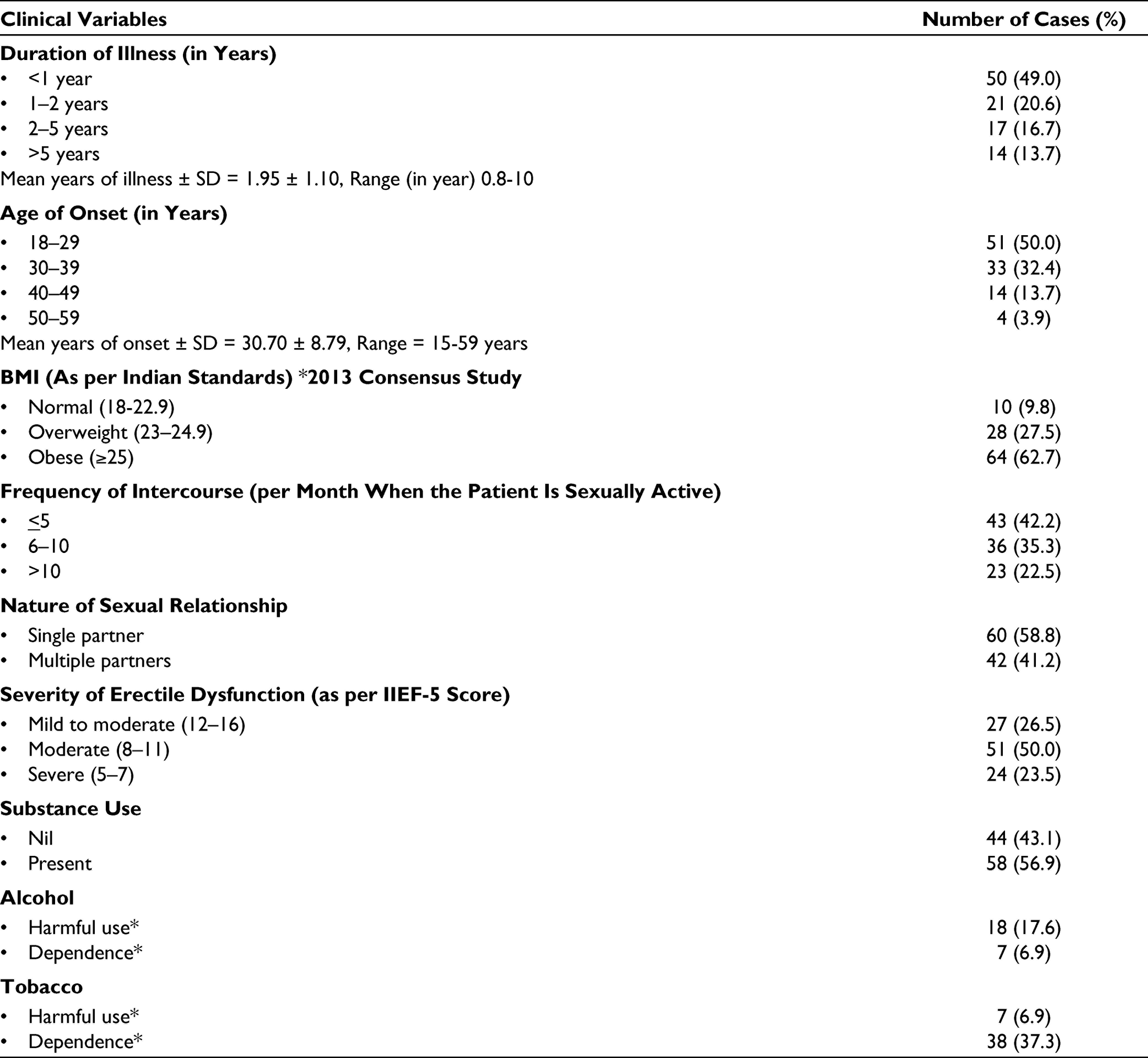
The severity of ED as per IIEF-5 score was moderate ED (n = 51; 50.0%) followed by mild-to-moderate ED (n = 27; 26.5%) and severe ED (n = 24; 23.5%). No patient with mild ED was found in the study sample. Substance use was found in the majority of the patients (n = 58; 56.9%). Among the patients using substances, tobacco dependence followed by alcohol dependence was common.
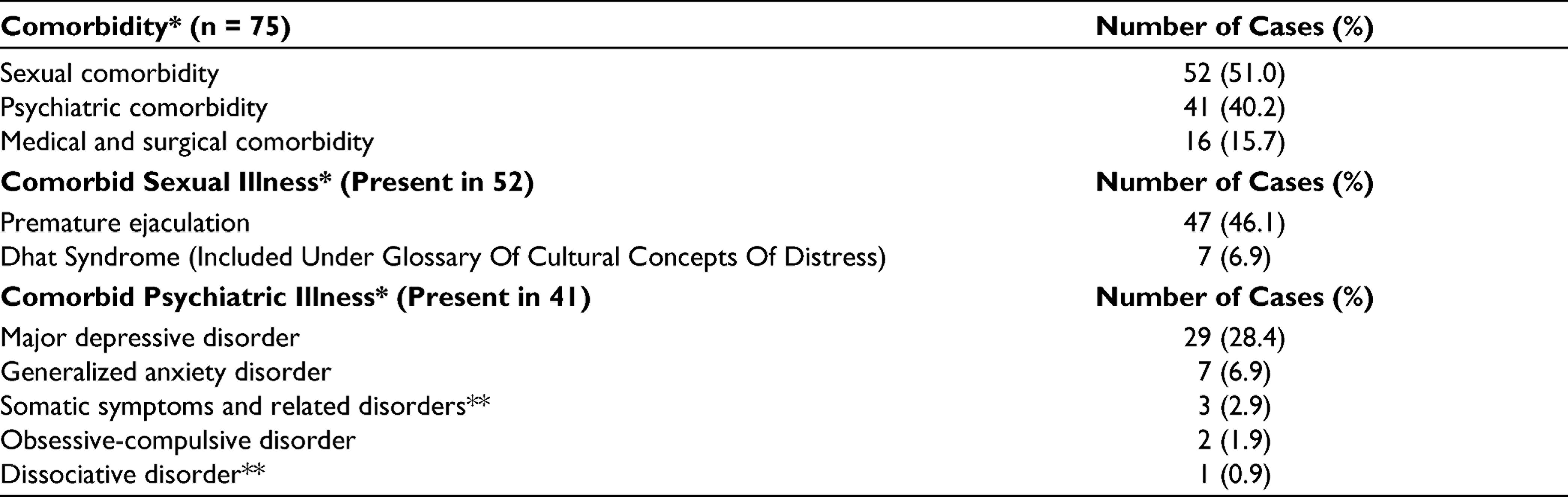
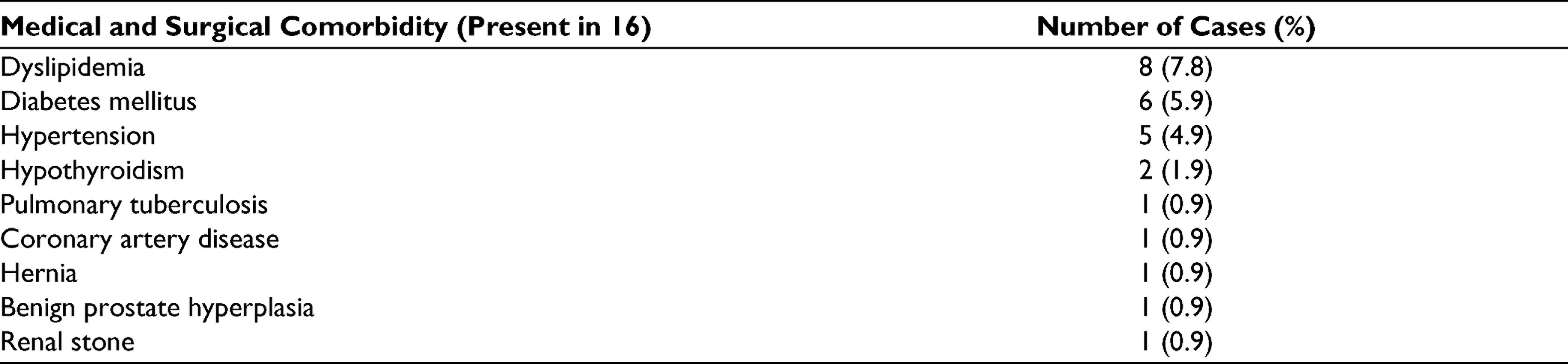
The majority of the patients had other sexual dysfunctions as a comorbidity (60.8%), followed by psychiatric disorders as comorbidity (40.2%). In sexual comorbidity, premature ejaculation (PE) was most common, followed by Dhat syndrome. Among psychiatric comorbidity, depression was most common. Among physical comorbidity, the most common comorbidity was dyslipidemia (7.8%), followed by diabetes (5.9%) and hypertension (4.9%; Table 3 and 4).
Distribution of Comorbidities (N = 102)
Distribution of Medical and Surgical Comorbidities
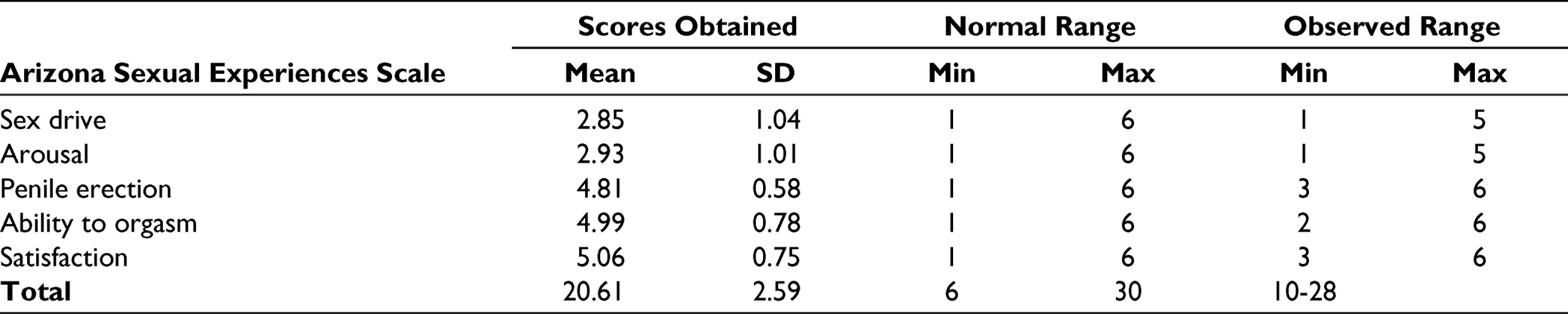
Higher scores indicate more significant sexual dysfunction in the ASEX domain. ASEX scores show greater sexual dysfunction in penile erection, ability to orgasm, and satisfaction domains and lesser scores in the domain of sex drive and arousal in our sample (Table 5).
Sexual Experience as per Arizona Sexual Experiences Scale (ASEX)
Discussion
The study was designed to study the sociodemographic and clinical profile of patients presenting with the complaint of ED in a specialty psychosexual clinic of a tertiary care hospital. The study sample consisted of 102 participants. The majority of the patients in this study were young adults with a mean age of 33.38 (standard deviation ± 9.31) years and range from 19 to 59 years. The earlier studies on ED also found that majority of the patients seeking consultation for ED in clinics are young adults. Indian studies by Pal et al 19 (33.22 ± 8.44) and Langer et al 26 (33.93 ± 5.05) also reported similar findings. In our study, the majority of the patients were in the 18 to 29 years age group (41.2%). Only 24 patients were above the age of 40 years, and out of these, 8 were above the age of 50 years. There can be several reasons for this preponderance of young adults in clinics seeking help for ED. People commonly initiate marital life or sexual life in their 20s and 30s,15,16 and sexuality remains an important focus of life at a young age. Any dysfunction in sexual functioning leads to relatively prompt help-seeking. In comparison to the mean age of patient seeking help in our sample, Western studies have reported a relatively higher mean age of treatment-seeking patients for ED. 17 There can be the following plausible explanations for this difference. Patients in India may be developing ED earlier than their Western counterparts. Though there is no literature on the reason for this differential ED onset, 1 possibility may be an earlier occurrence of the causative factors for ED, like cardiometabolic diseases. 18 Another possibility could be that older people in India do not seek treatment for ED. Sex is still considered a taboo subject in India. People at a later age may accept their ED as an age-related decline of sexual functioning and might not be inclined to help-seeking for the same. This study cannot answer these questions, and future research with community sample and prospective follow-up may clarify these age-related differences in treatment-seeking in India.
In this study, primarily married men sought treatment for ED as reported in some earlier Indian studies.16,19,20 An explanation for this can be attributed to the fact that unmarried individuals are less likely to indulge in regular sexual intercourse, thereby limiting the situations where their sexual dysfunction is apparent to them. 21
The sample of this study represented mainly the Hindu belonging to middle and lower socioeconomic classes, which were comparable with the study by Kumar et al. 22 A majority of the patients seeking consultation had education between 9 and 12 years (40.2%), followed by >12 years (37.3%) of education. This was supported by other studies by Capogrosso et al 23 and Verma et al. 16 In our study, the patients were primarily farmers, clerks, or shop owners with a monthly income of ≤Rs. 10,000/month. This finding can be explained by the level of education in the majority of the sample as described above. It can be argued that since occupation and income bear a direct effect on lifestyle and health, lower socioeconomic status may be associated with a greater prevalence of ED. Similar rates of higher prevalence of ED in patients with lower socioeconomic status is reported in few earlier studies also.24,25 The geographical and population characteristics of treatment seekers at this governmental medical university center mainly belong to middle and lower socioeconomic classes. Most of the patients seek help by themselves, and mostly only educated people are able to reach tertiary care centers for help-seeking. This can be a possible explanation for the above sociodemographic characteristics of the sample.
Our study sample’s mean years of illness were 1.95 ± 1.10, with a range of 0.8 to 10 years. Other Indian studies reported even longer mean years of illness compared to this study as 3.18 years in the study by Langer et al 26 and 5.68 years by Pozzi et al. 27 Although our study sample reached this treatment center relatively early in comparison to data reported by other Indian studies, patients of ED in India seek consultation after a considerable delay.26,27 As happens in other medical illnesses, chronicity of illness increases its severity, treatment resistance, and may result in poor outcomes. Hence, attempts should be made to encourage early help-seeking for the patients with ED. Early initiation of the management is likely to reverse underlying etiopathogenesis and might lead to better outcomes.
Only 9.8% of patients were in the normal BMI range. The rest of the patients with ED had BMI above standard limits, with 62.7% of the sample falling in the obese category. Our results are consistent with the findings in a study conducted on the role of lifestyle, and psychological variables in ED found similar results and observed a direct relationship between obesity and sedentary lifestyle with ED.26,28 Thus, obesity, via increased cardiometabolic risk and decreased testosterone levels, may act as a significant risk factor for ED. Hence, its effective management is crucial from a clinical point of view. 28
On assessing the severity of ED by IIEF-5 score, moderate severity was observed in 50%, followed by mild-to-moderate severity in 26.5% and severe ED in 23.5% patients. None of our subjects reported mild levels of ED. Other studies conducted in clinical population reported slightly different distribution of severity like the study by Nordin et al 15 (mild ED 17%, mild to moderate 11.5%, severe ED 29.5%) and Van et al 29 (mild ED 40.8%, mild to moderate ED 20.3%, severe ED 0.8%). As this study is conducted in a tertiary care referral center, patients with mild ED might not be seeking help here due to lack of access, perceived low severity, or lack of information about availability of the treatment. However, studies with community samples may identify them.
In comorbidities, sexual comorbidities were reported among 51% of participants. The most common sexual comorbidity was PE, followed by Dhat syndrome. Verma et al 16 reported similar findings. A study by Tsai et al 30 analyzed the relationship between ED and PE comorbidity. ED and PE frequently coexist and have a complex relationship. ED is reported to be the most critical risk factor of PE. The coexistence of both is associated with higher rates of psychiatric symptoms, namely depression and anxiety. Patients of ED need intense stimulation for achieving and maintaining an erection. This may lead to early ejaculation. Shared etiological biological mechanisms may also explain higher rates of this comorbidity.
Additionally, Capogrosso et al 31 reported that comorbid ED and PE are more common in patient presenting with ED in less than 40 years of age compared to the patients presenting with ED after 40 years. Our sample consists primarily of patients less than 40 years of age; hence, this comorbidity is more common. Dhat syndrome is a common sexual neurosis reported by patients with sexual dysfunction in Southeast Asia. Patients concerned with sexual dysfunction try to explain their problems due to Dhat syndrome as this is one of the most common cultural explanatory models for sexual dysfunction in India. 32
The most common psychiatric comorbidity was depression, followed by anxiety symptoms. Depressive symptoms were reported by 69.6% (N = 70) of the participants, out of which 40.2% (N = 41) reported mild severity as per the HAM-D scoring, and 23.4% (N = 24) reported moderate symptoms. This was comparable to the study by Nordin et al 15 ; hence, depression is commonly comorbid with ED. Several other studies have earlier reported them to be associated together. Depression has been reported to be an etiological factor for ED, and ED has been reported to be causing or exacerbating depression resulting in bidirectional causation. 5 Depression may also complicate the assessment and management of the ED. A detailed clinical evaluation may help assess which disorder was first developed, relative severities, and their impact on life. This may help in deciding management priorities.
Regarding substance use, 56.9% (N = 58) of participants reported some form of substance use. Alcohol and tobacco are the most commonly used substance in the Indian population. In our study, 37.3% had tobacco dependence and 6.9% had alcohol dependence. Higher smoking and alcohol consumption has been linked to ED.26,33,34 The exact etiopathology of ED in substance use disorder remains poorly understood. However, impairment of endothelium-mediated smooth muscle relaxation is commonly implicated. Stopping cigarette smoking is a factor that rapidly improves penile tumescence and rigidity in patients treated for ED. Reduction of smoking and alcohol use is considered an important harm reduction strategy for ED. 35 Medical comorbidities were not common in our study. Obesity was commonly reported. Other metabolic dysfunctions were less commonly found. The predominant sample of this study consisted of young adults. Obesity is a common precursor of other metabolic dysfunctions. However, other metabolic comorbidities and related medical illnesses like dyslipidemia, diabetes, and hypertension may develop later. Hence our sample, although it had a high prevalence of obesity, other metabolic comorbidities were notably lesser. ED is considered an early manifestation of cardiovascular (CV) disease. Current recommendations suggest that men with ED should be carefully assessed for CV disease to prevent significant CV events. Effective management of CV risk factors reduces the risk of major CV events in the future and improves ED in longterm. 36
The scores of the ASEX scale show lower value in the domain of “sex drive” and “arousal” (2.85 ± 1.04) and (2.93 ± 1.01) while scoring high in the domain of “penile erection,” ability to orgasm, and satisfaction was 4.81 ± 0.58, 4.99 ± 0.78, and 5.06 ± 0.75, respectively. Similar findings had been reported in studies where mean scores for penile erection, ability to orgasm, and satisfaction were 4.2 ± 0.7, 4.2 ± 1.0, and 4.2 ± 1.0, respectively. 37 During the sexual response, sexual drive and subjective arousal are important predecessors of penile erection. This is marginally affected in the patients of ED in this sample. However, other areas of sexual functioning like orgasm and satisfaction were significantly poor in our sample, as is expected in patients having ED. This group of patients is likely to have a higher prevalence of psychogenic ED. Relatively younger age of the sample and lesser medical comorbidity is also suggestive of this possibility. In psychogenic ED, sexual drive and arousal may not be affected significantly. Hence, this sample patient’s sexual drive and subjective arousal was relatively spared.
The study also has several limitations. The study’s sample size was small, limiting the power of the findings and generalization of results. Self-report-based tools were used in the study, which is considered subjective measures to estimate the prevalence of ED. Investigations like cavernosometry and color penile Doppler ultrasound could not be used in our study due to logistic difficulties and resource constraints. Although self-perception is the most common way of studying ED, it may sometimes give erroneous findings. We could not establish a causal relationship between the various sociodemographic and clinical variables we studied with ED. At best, we were able to arrive at correlational conclusions. The findings can be generalized to a sample of a population similar to our study population only.
Conclusion
The majority of the participants in this cross-sectional study were young males who were married and overweight, and about one-third of them used tobacco. The most common sexual and psychological comorbidities were PE and depression. Often patient presents with moderate and severe ED, and other sexual and psychiatric comorbidities are relatively common. Hence, clinicians must remain aware that ED is not only a problem affecting aged people but a good number of young people are also affected. Therefore, whenever a young person is visiting to seek treatment for ED, a comprehensive evaluation including a detailed psychological assessment is likely to be beneficial for proper management planning.
Future Directions
Future studies should aim to assess the etiology of EDs in young patients in India. Additionally, prospective followup of such patients will inform about the outcome and course of the illness. This knowledge might help to improve the management guidelines for young people presenting with the ED in clinics.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.