
Abstract
Background:
Previous studies showed the association of female sexual dysfunction (FSD) with various specific organic, psychiatric, and social factors separately, but rarely evaluated the extent of association of various disorders all together in cases of FSD.
Aim:
This study was conducted to explore the comorbidities associated with FSD from physical, psychiatric, and social perspectives.
Materials and Methods:
All female patients aged between 18 and 60 years reporting sexual problems to the psychiatry outpatient department were evaluated with Arizona sexual experiences scale for females. Their assessment included detailed medical and psychiatric history including the history of social contributing factors and medicine intake followed by physical and mental status examinations. Relevant biochemical investigations and hormonal assessments were done. Data were analyzed using Pearson correlation coefficients, linear regression analysis, and independent samples t tests.
Results:
Seventy-three females were diagnosed as cases of FSD according to the Arizona sexual experiences scale in one year. Among them, 1.37% had no comorbidity and the rest 98.63% had psychiatric comorbidities which were combined with physical comorbidities (mostly hypothyroidism, hyperprolactinemia, and abnormal menstrual cycle) in 35.62% cases and social contributing factors (mostly husbands’ substance abuses and various family-related problems) in 32.88% cases. The duration of FSD predicted its severity.
Conclusion:
The severity of FSD increased with duration. Thus, all cases of FSD should be assessed early in detail for physical, psychiatric, and social contributing factors to treat them holistically. Psychiatrists should play a key role in assessing, diagnosing, treating, and referring them to the appropriate treatment providers.
Introduction
Sexual function is an essential component of life and thus, the presence of sexual dysfunction can lead to a negative impact on the well-being of both men and women equally. 1 In females, it can present as difficulty during any stage of normal sexual activity such as physical pleasure, desire, arousal, or orgasm. 2 Female sexual dysfunction (FSD) has been classified most recently into 4 types: interest, arousal, orgasmic, and pain disorders. 3 The actual epidemiology of FSD is difficult to determine and varies considerably as per different studies and places.1,4,5 Despite these variations, there is reasonable consensus that the prevalence of women who report one reasonable sexual dysfunction ranges from 40% to 50% irrespective of the age and is more prevalent in the reproductive age group with much higher rates in infertile females.2,3,5-8 These prevalence estimates vary widely in India for hypoactive desire, arousal, and orgasmic disorders while the pain disorders or dyspareunia comprise the majority of sexual dysfunction which women complain of.3,8,9 The origin of FSD may stem from a biological or organic, a psychological, and/or a social condition. 6 Meta-analysis of more than 40 studies noted an association between FSD and physical health, emotional condition, and social factors as well as race, ethnicity, and religion.1,10
Psychiatric disorders or psychological factors have been documented as one of the most important factors for FSD which is more strongly linked to mental health and stress than to physical function or age itself. 11 Various types of FSD have been found in depression, obsessive-compulsive disorder (OCD), generalized anxiety disorder (GAD), and other anxiety disorders.11,12 A clear relationship between severity of depression and prevalence of sexual dysfunction has already been established and it has been found to be the independent risk factor for FSD too.9,11,13 Very high prevalence of sexual dysfunction was found in women with psychotic disorders such as schizophrenia and schizophrenia spectrum disorders, bipolar disorder because of the disorder itself, and also as a result of antipsychotics, antidepressants as well as benzodiazepines and lithium combination used for their treatment.11,14 In addition, psychological issues such as self-esteem, body image, a prolonged period of abstinence from sex, a strained relationship with the partner, childhood sexual abuse, chronic stress all have an impact on sexual function and also seem to be associated with FSD.15,16 However, each study assessed the association of FSD in case of a specific condition, but the reverse evaluation was not done to find out the association of all these in cases of FSD.
Among the medical comorbidities, FSD has been found to be associated with vascular risk factors including hypertension (HTN), coronary heart disease, metabolic syndrome, obesity, diabetes and lung disease. 10 Women with diseases involving the central nervous system may experience decreased sexual desire whereas diseases of the peripheral nervous system may cause orgasmic disorders but local pathologies are responsible for dyspareunia.10,15,17 FSD is significantly more frequent in diseases affecting multiple systems such as thyroid dysfunction or both type 1 and type 2 diabetes and chronic diseases like psoriasis too.1,12,17,18 Hypothalamic-pituitary-axis dysfunction, surgical or medical castration, natural menopause, premature ovarian failure, and chronic oral contraceptive pill (OCP) use have been found to be important causes of hormonally based FSD.16,19 But the studies did not evaluate the extent of these associated risk factors in a sample of FSD.
Irrespective of the presence or absence of organic disease, age, education, socioeconomic status, marital status, emotional and relational issues significantly affect sexual arousal and functioning. 1 Studies revealed that spouse- or partner-related factors such as impaired physical and mental health of the partner, undesirable drinking behavior, illicit drug dependence, and male partner’s sexual dysfunction as well as family-related issues such as parity, family size, daily stressors, chronic stress in the family, and domestic violence at any point of a life of a female can lead to FSD.20-26 Even cultures have an influence on the overall sexual functioning and thus FSD also varies across cultures.3,27,28 Again each study assessed the association of FSD in case of a specific condition separately, but the evaluation was not done to find out the association of all these factors in cases of FSD.
Despite having an array of factors that are often associated with FSD, only a few studies have considered more than one comorbidity, mostly limited to 2 or 3 only and often failed to provide a complete picture.2,10,15,29 Therefore, there is a need to assess all possible medical and psychosocial factors implicated in FSD together to get a complete picture of the comorbidities involved and establish an accurate diagnosis from a biopsychosocial perspective for their proper treatment. This study aims to focus on medical as well as psychosocial comorbidities involved in FSD.
Materials and Methods
The study was conducted at the psychiatry outpatient department (OPD) of an ESIC hospital situated at Rohini, Delhi, India. It is a 300-bedded government general hospital and has got all basic specialties. The catchment area of this hospital is the whole northern part of Delhi. Patients are the employees at various industries and their family members who are referred from various dispensaries in this part of Delhi or from various other departments of the hospital for psychiatric consultation. The subjects were recruited by purposive sampling technique over a period of one year from November 2016 to October 2017 to assess the profile of comorbidities in cases of female patients with sexual dysfunction. Prior consent was taken from each patient and clearance was taken from the hospital ethics committee for conducting the study.
Female patients referred from either dispensaries or various other departments of the hospital to the Psychiatry OPD for sexual problems as well as the patients who were found to have sex-related problems during initial assessment in psychiatry OPD had been evaluated subsequently by a female psychiatrist throughout the study maintaining privacy and confidentiality. First, they were assessed with Arizona sexual experiences scale (ASEX) for females. 30 The patients who had sexual dysfunction according to the scale (on the ASEX female version) were included in the study. The patients who did not have sexual dysfunction according to the scale (on the ASEX female version), as well as the patients aged below 18 years and above 60 years, were excluded from the study. Sex-related problems, sociodemographic parameters, history of menstrual cycle, breastfeeding, and contraceptive use were recorded in a specially designed proforma. It also included the history of 9 social/family issues that might have been associated with FSD, ie, the number of children, the total number of family members, availability of separate room for the couple, staying with the partner or not, sex-related problem of the partner, substance abuse and other psychiatric disorders of the partner, physical disease of the partner, domestic violence, and any other family-related problem/stressor. Their detailed medical and psychiatric history including medicine intake, if any, the findings of physical examination and mental status examination were noted in the psychiatric case record file. If the patients were on any medication, the duration of medications and side effects were also noted. The diagnosis of psychiatric disorders as well as FSD was made according to the International Classification of Diseases (ICD)-10 Diagnostic Criteria for Research (DCR). 31 During the physical examination, special emphasis was given to secondary sexual characters and blood pressure, which were noted on the proforma. Biochemical investigations and hormone assessments that were available in the hospital were done to get the profile in terms of fasting blood sugar level, thyroid function test, and serum prolactin levels.15,16 Physical diseases were either already diagnosed by the other departments prior to the referral or they were diagnosed based on the findings of physical examination, biochemical investigations, and hormone assessments.
The ASEX Scale
The ASEX is a brief and five-item questionnaire designed to measure sexual functioning over the past week in the following 5 domains: sexual drive, arousal, penile erection, or vaginal lubrication, ability to reach orgasm, and satisfaction with orgasm. It consists of a six-point scale from 1 to 6 to rate the items toward increasing severity. Total scores vary from 5 to 30 and higher scores indicate more severe sexual dysfunction. A total score of >18 or a score of ≥5 on any single item or individual scores ≥4 on any 3 items suggests clinically significant sexual dysfunction. The scale has one version for males and another for females where only the third question differs and mentions penile erection and vaginal lubrication for males and females respectively. The scale may be utilized to evaluate the current level of sexual functioning as well as to assess the changes in sexual functioning resulting from clinical interventions over a period of time. The scale has very high test-retest reliability and strong validity too. Both heterosexual, as well as homosexual populations, can be assessed with this scale and it can be used even for the persons without sexual partners. 30 The female (Hindi translated) version of the scale was used to diagnose FSD and its severity.
Statistical Analysis
Descriptive analysis was done for sociodemographic and clinical data. We computed Pearson correlation coefficients for the patients (n = 73) between the ASEX scale score and other parameters like age, education, duration of marriage, number of children, the total number of family members, duration of FSD, and duration of psychiatric disorder. Subsequently, linear regression analysis for the patients with FSD (n = 73) with ASEX scale score as dependent variable whereas the duration of FSD (parameters with significant correlation) as independent variable was performed using separate entry and stepping meth-od with F value of 3.84 for entry and 2.71 for removal. The patients were divided into 5 groups: group A = FSD without any comorbidity, group B = FSD with psychiatric comorbidities, group C = FSD with physical comorbidities, group D = FSD with social comorbidities, and group E = FSD with all types of comorbidities (psychiatric + physical + social comorbidities). Various groups were compared on the ASEX scale score using independent samples t tests. P < .05 was considered as statistically significant. Statistical analysis was done using Statistical Package for Social Sciences (SPSS) version 23 (International Business Machines Corporation, New York, USA).
Results
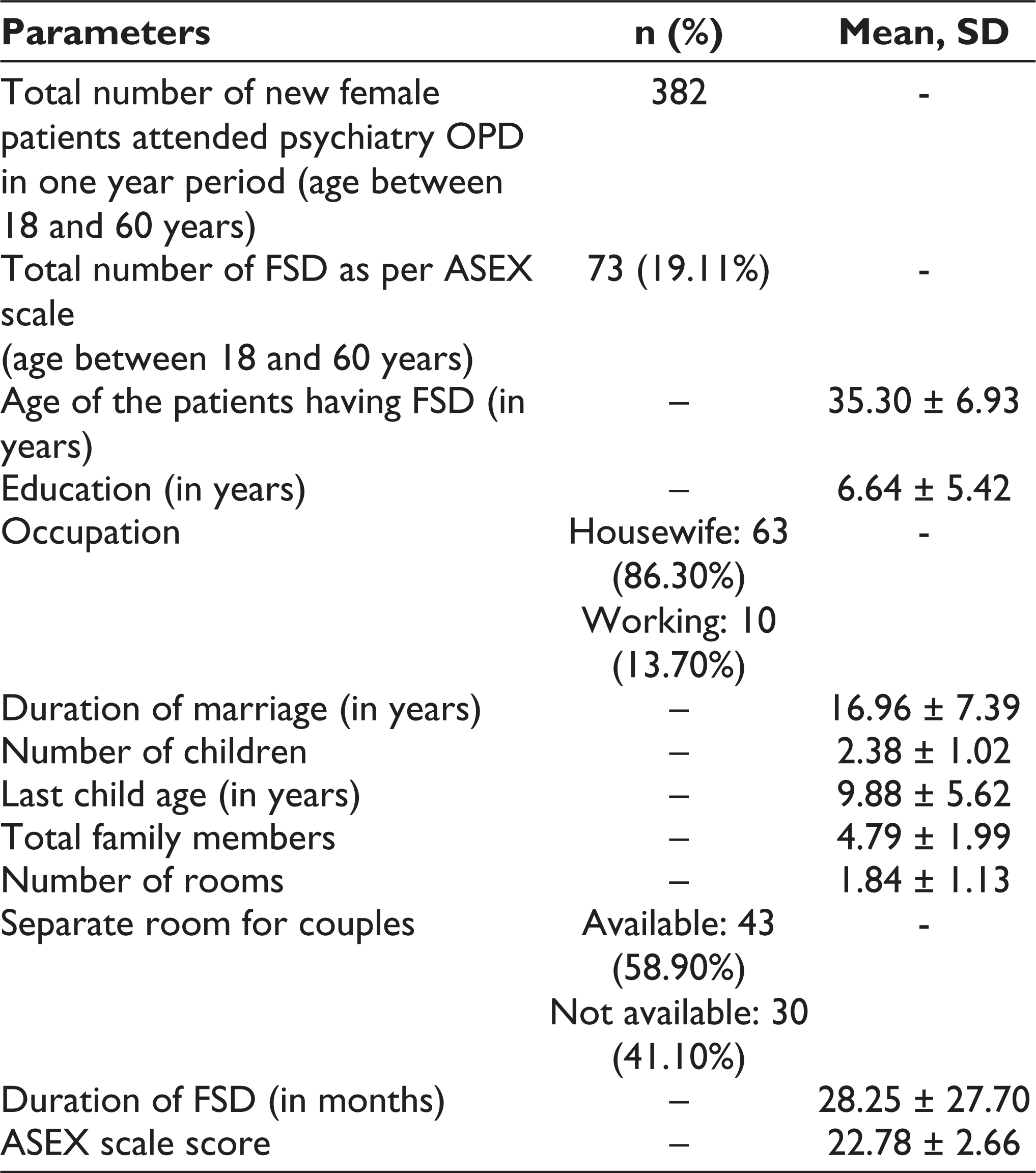
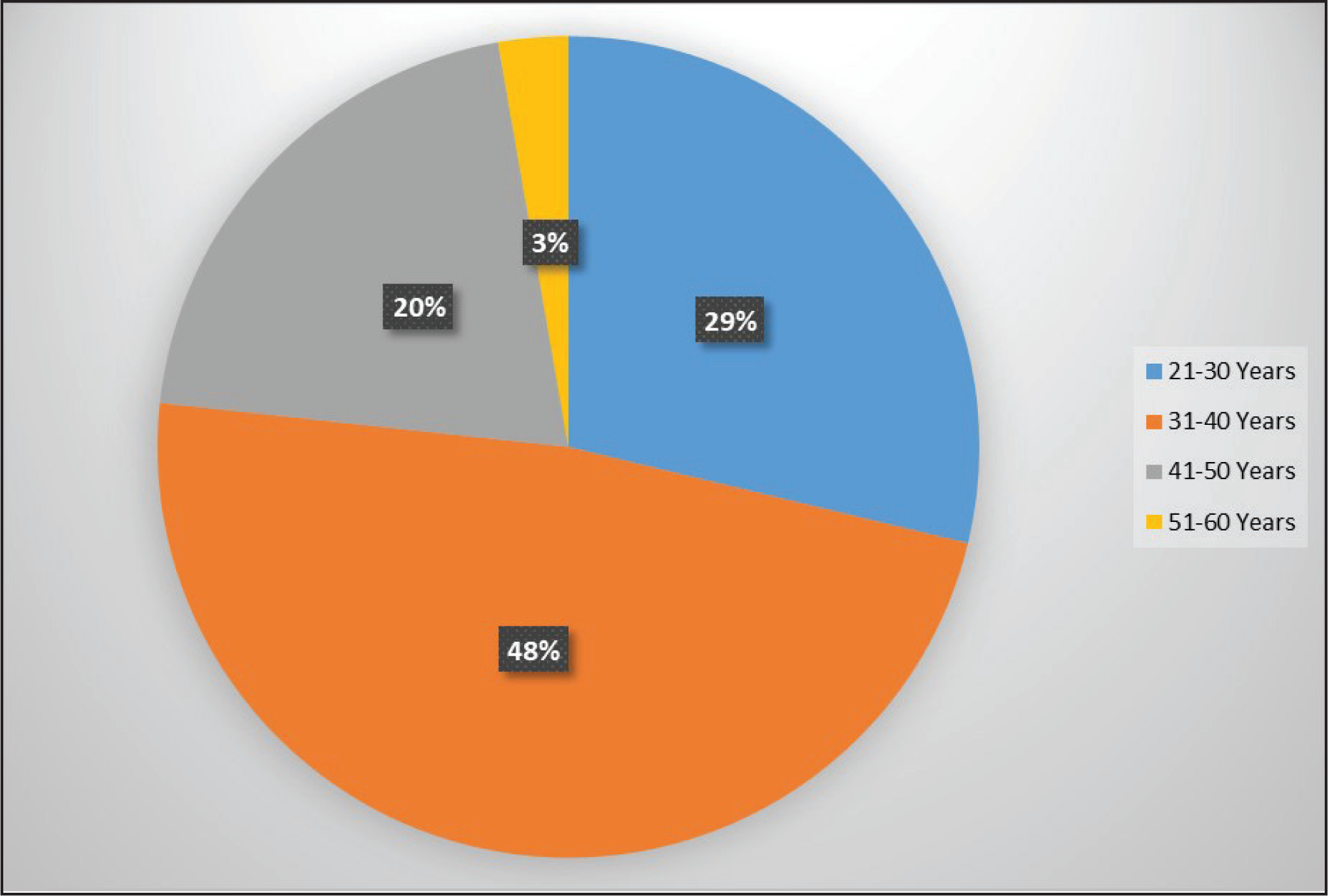
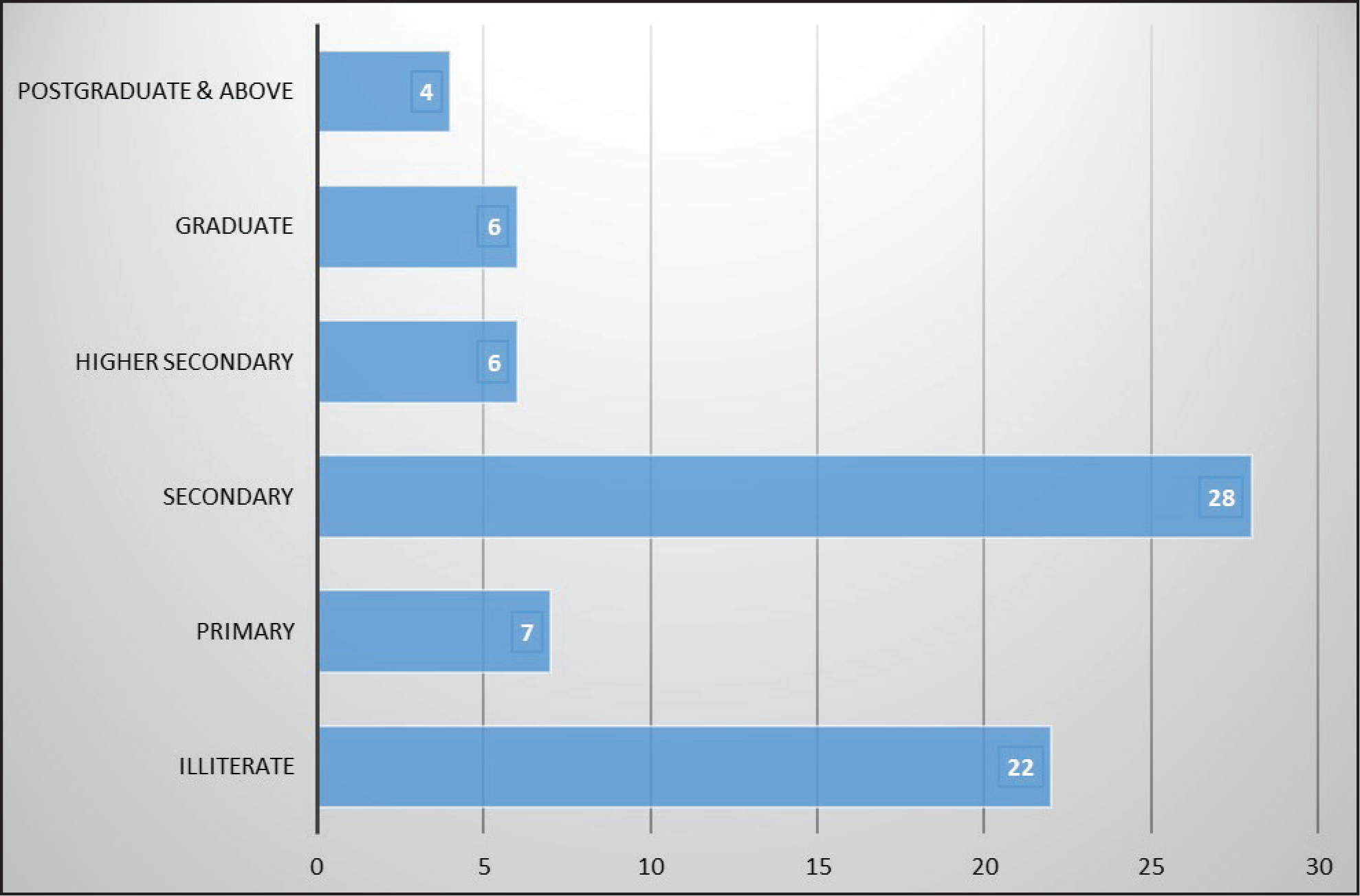
Seventy-three patients were diagnosed as cases of FSD according to the ASEX scale in one year. Age varied from 23 years (minimum) to 51 years (maximum) and most of them were either the employees or the wives of the persons employed in industries or business organizations at various lower positions and belonged to lower socioeconomic status. Various particulars of the patients have been summarized in Table 1. Age- and education-wise breakups of the patients have been shown in Figure 1 and Figure 2, respectively. Two patients were on antihypertensive drugs (Amlodipine and Enalapril) for about 11 and 5 months, respectively, one patient was on an oral hypoglycemic drug (Glimepiride) for 7 months, and 2 patients were on Levothyroxine for the last 2 years and 9 months, respectively. None of them reported any side effects of drugs. All the patients were married and none of them was pregnant or continuing breastfeeding. Most of the patients (97.26%) were staying with their husbands continuously except for 2 of them (2.74%) who stayed intermittently. None of the patients was on depot contraceptives or OCP; mostly barrier methods of contraception were used by their husbands.
Details of the Patients (n = 73)
Age-wise Breakup of the Patients (N = 73)
Education-wise Breakup of the Patients (n = 73)
Profile of Comorbidities (n = 73)
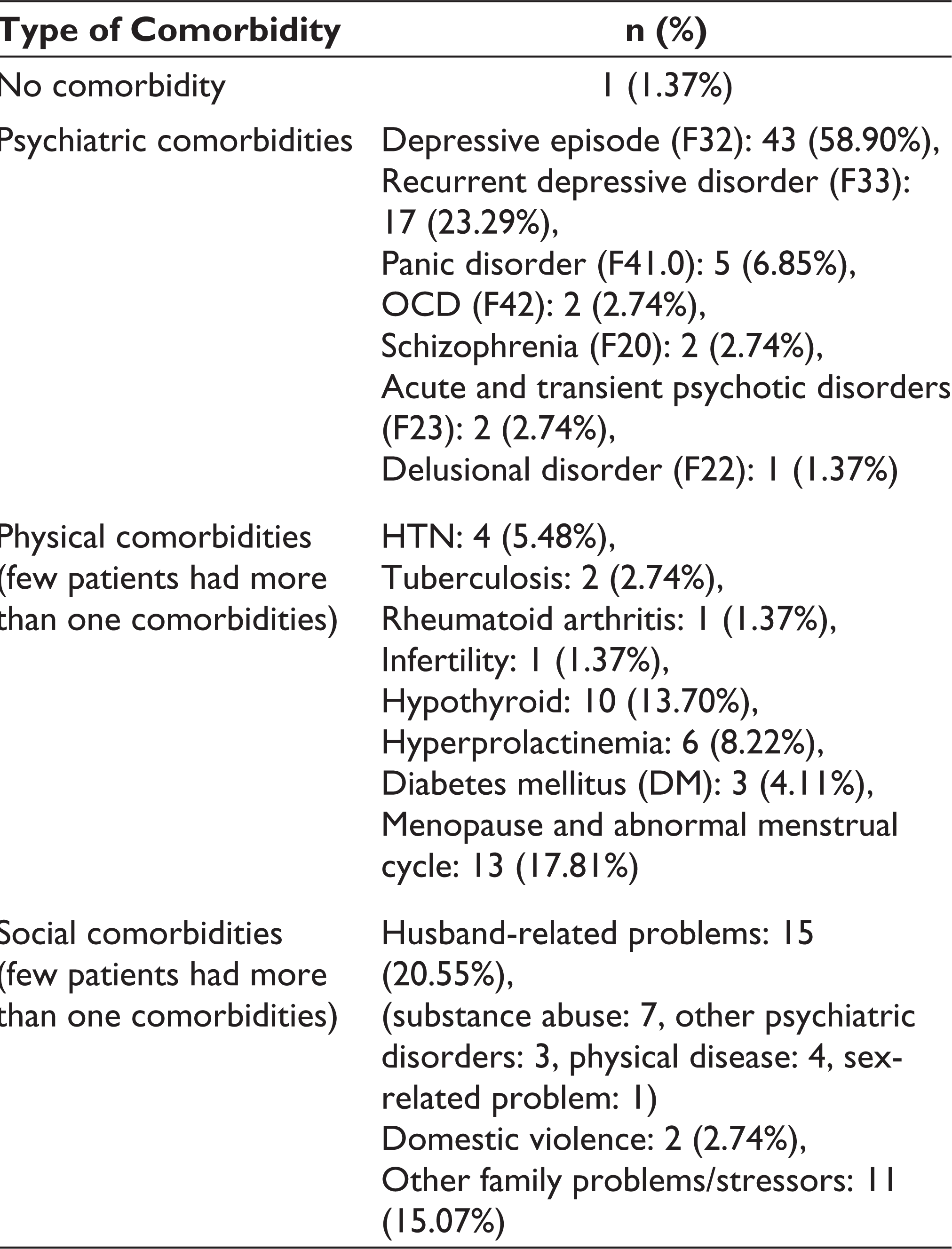
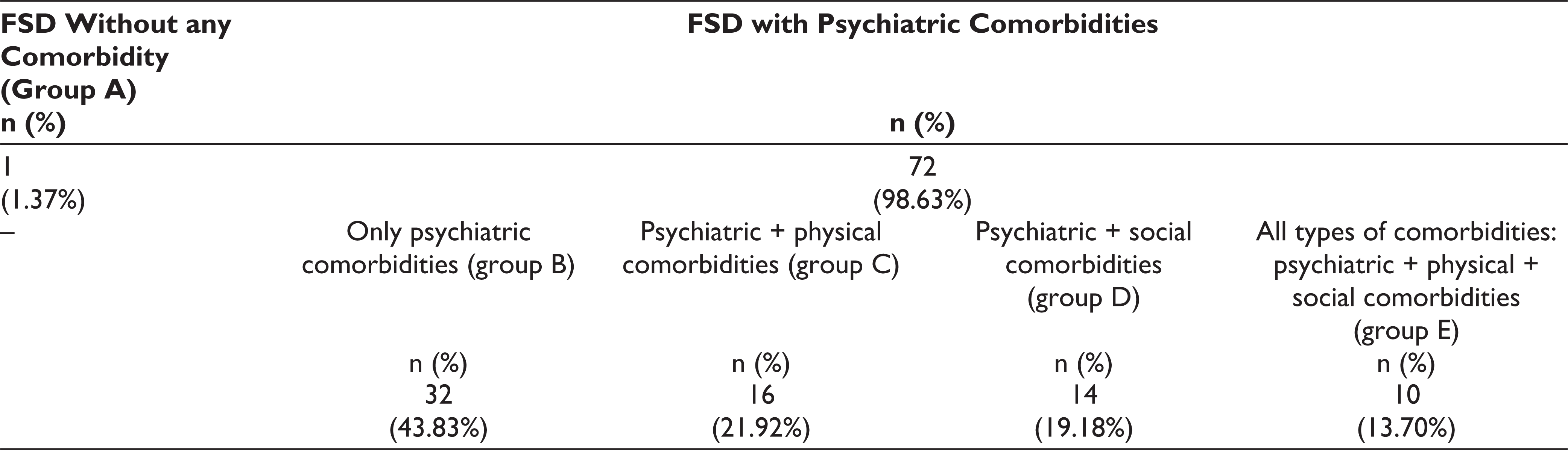
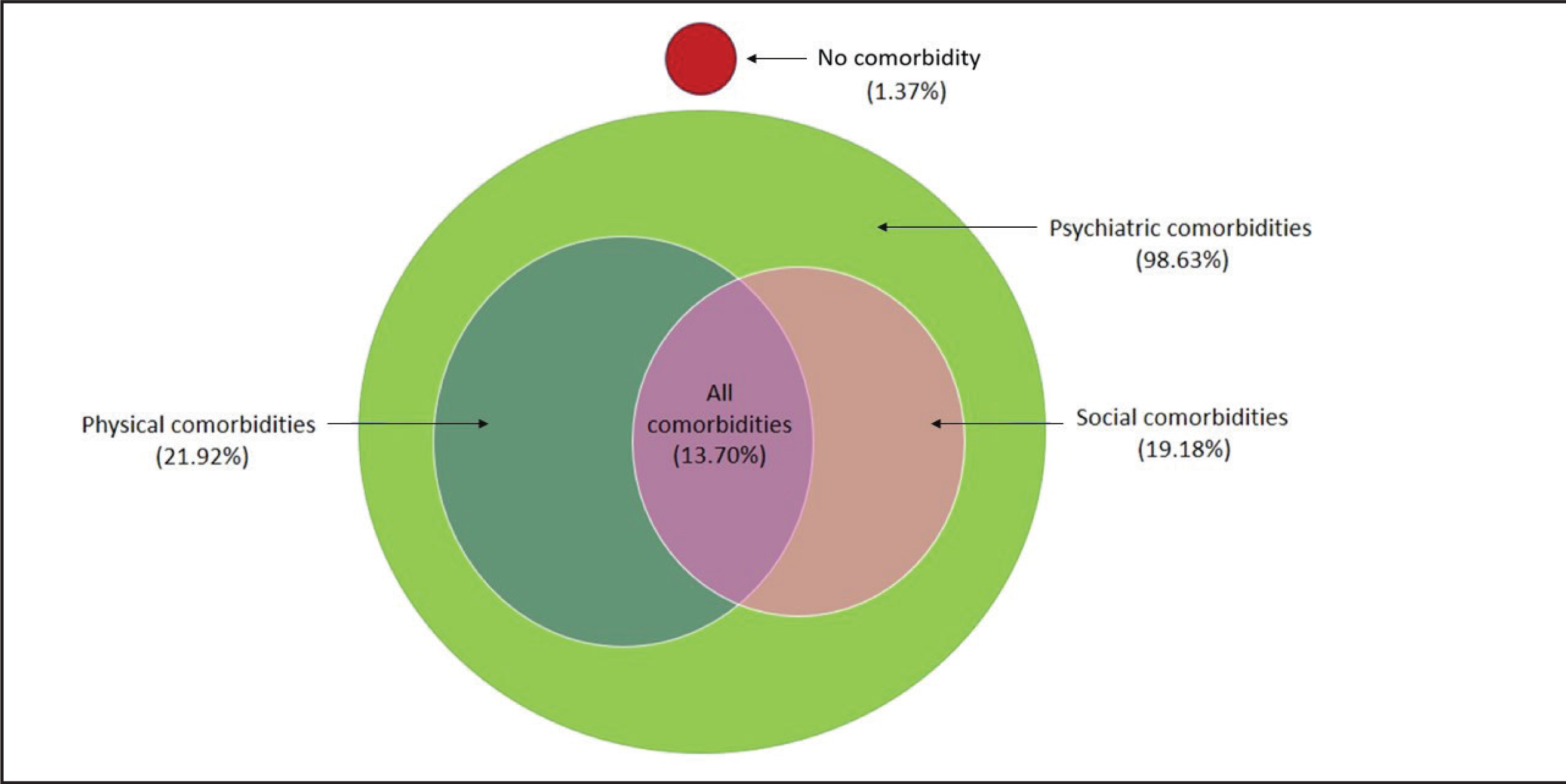
The profile of comorbidities has been shown in Table 2. Out of these 73 patients, only 1 patient (1.37%) had FSD without any comorbidity and the rest 72 patients (98.63%) were diagnosed as FSD with psychiatric comorbidities (Table 3). These 72 patients with psychiatric comorbidities have been subdivided into 4 groups: (i) with only psychiatric comorbidities (group B); (ii) with physical comorbidities (group C); (iii) with social comorbidities (group D); and (iv) with all types of comorbidities (group E: psychiatric + physical + social comorbidities; Table 3). It has been observed that pure group C (with physical comorbidities only) and pure group D (with social comorbidities only) were not available and both the groups were also having psychiatric comorbidities (Figure 3).
Division of the Cases with Various Types of Comorbidities (n = 73)
The Relation Among the Cases with Various Types of Comorbidities (n = 73): FSD Without any Comorbidity; FSD with Psychiatric, Physical, Social, and all Types of Comorbidities (Psychiatric + Physical + Social). FSD, female sexual dysfunction
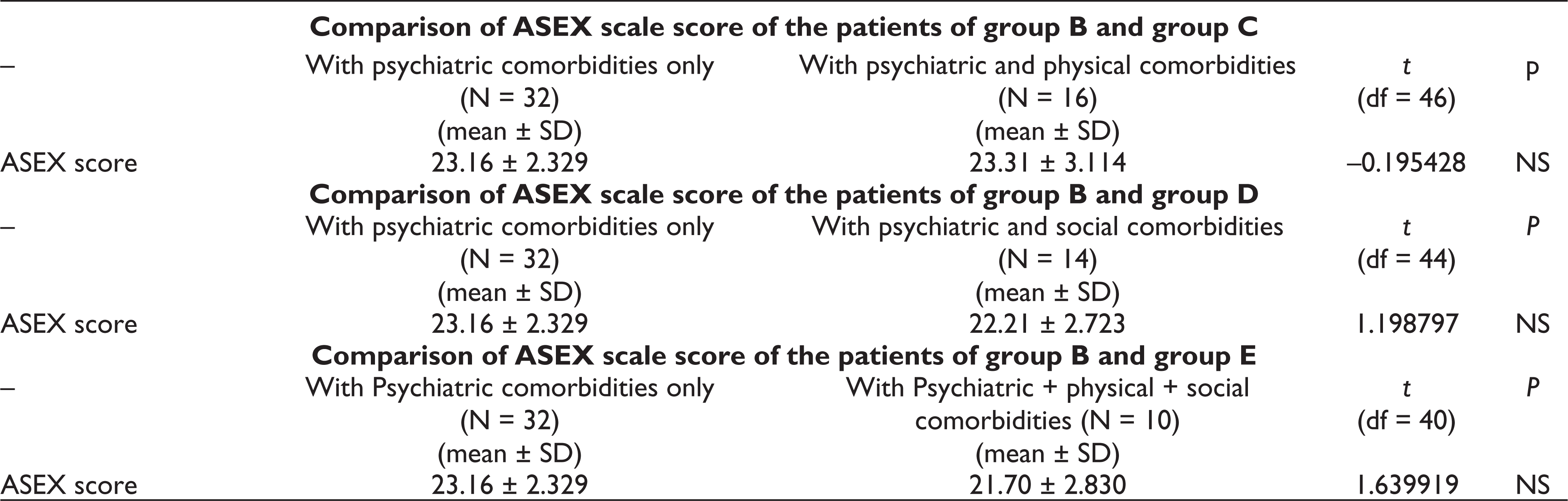
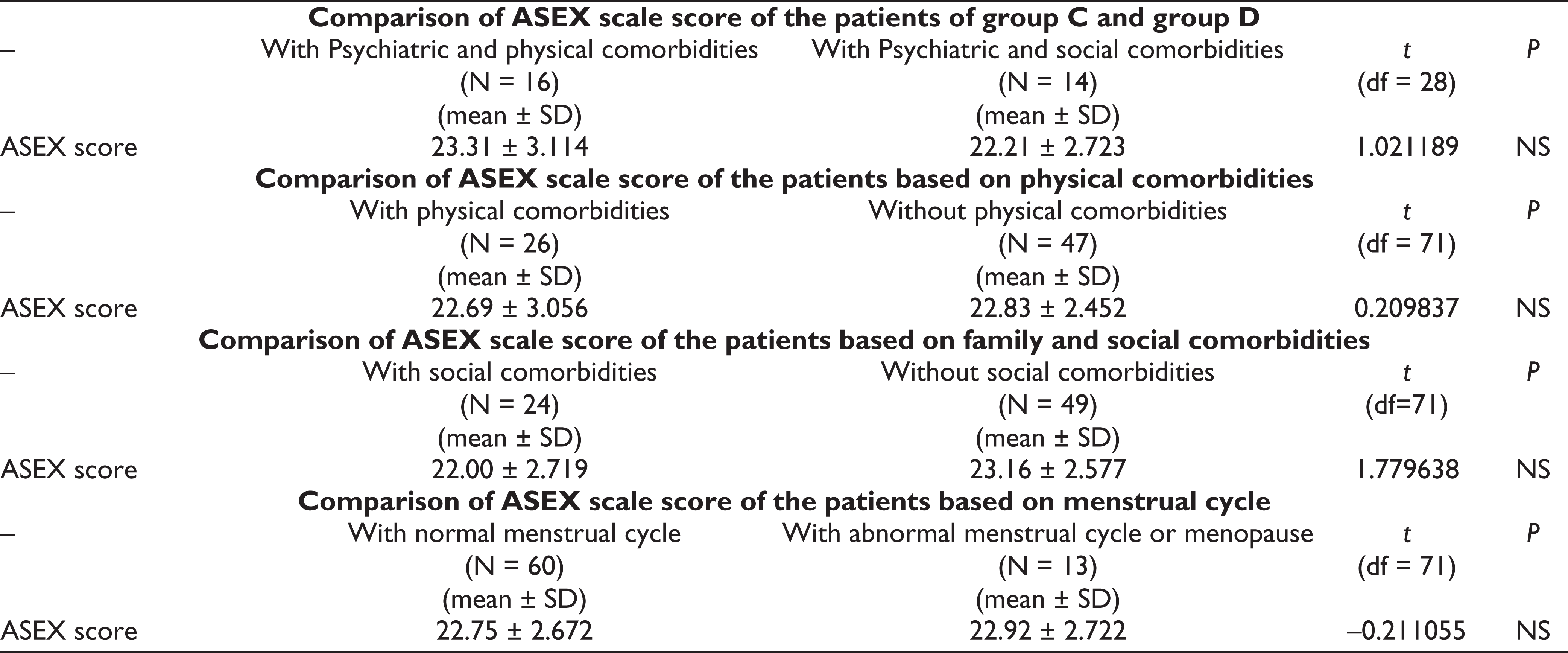
ASEX scale scores were compared between the patients of group B and C, group B and D, group B and E, group C and D as well as based on the menstrual cycle and presence of physical and social comorbidities separately. But none of them were found statistically significant (Table 4).
Comparison of ASEX Scale Score of the Patients Based on Various Comorbidities
Correlation and Regression Analysis
ASEX scale score of the patients showed a significant correlation with duration of FSD in months (r = 0.334; P = 0.004) and linear regression analysis found duration of FSD in months (R = 0.334; Constant = 21.874; P = 0.004) as a predictor variable for ASEX scale score (n = 73). ASEX scale score of the patients also showed a trend of correlation with the duration of psychiatric disorder in months (r = 0.228; P = .054; n = 72). However, no significant correlation was found between the ASEX scale score and other parameters like age, education, duration of marriage, number of children, and the total number of family members.
Discussion
In our sample, around one-fifth (19.11%) of all new female patients, aged between 18 and 60 years, had sexual dysfunction. The figure is substantial and indicates that in a psychiatry OPD, sexual history should be explored in the case of all adult females. Although most of the studies mentioned the prevalence of FSD in the range 40% to 50% irrespective of age, there are variations in a few studies.2,3,6,8,9,32 Our data show that a large number of young patients presented with sexual dysfunction compared to patients aged more than 40 years (Figure 1). It might be because of more young patients visiting our psychiatry OPD with previous studies showing a similar trend.2,7,8,33 The duration of FSD showed a significant correlation with the ASEX scale score and it could predict the scores on the ASEX scale suggesting a significant increment of the ASEX scale score with an increase in the duration of FSD. Because of the paucity of studies in this area of FSD, our finding is a new one. The absence of statistically significant comparison of ASEX scale scores between the patients of various groups based on the presence of psychiatric, physical, and social comorbidities (Table 4) might be because of the presence of psychiatric comorbidities in all the groups and the lack of availability of pure physical and social groups for analysis. Even the absence of significant correlations between ASEX score and various sociodemographic parameters as per our study is supported by mixed findings from previous studies; with some showing positive correlation, while others showing no correlation at all. 2
In our study, almost all patients (98.63%) were diagnosed as having sexual dysfunction with psychiatric comorbidities whereas 43.83% had only psychiatric comorbidities and the rest had other comorbidities too (Table 3). It may be explained by the lack of awareness about psychiatric disorders and reluctance to get them treated. It also indicates that any female patient reporting sex-related complaints should be sent to a psychiatrist for evaluation first.11,12 Moreover, one key finding is that 82.19% of patients had depression in the form of a depressive episode or recurrent depressive disorder. In comparison, very few patients had panic disorder and OCD while only 6.85% had psychotic disorders. Previous studies found that depression, anxiety, and sexual dysfunction in women are interrelated but the causal pathway is unclear. Depression and anxiety lead to sexual dysfunction or sexual dysfunction is a cause of mood disorder is debated as bidirectional with the third possibility of all the 3 resulting from an underlying vulnerability to both psychiatric disorder and sexual dysfunction.11,12,34,35 Even psychosis can also lead to FSD because of positive and negative symptoms, poor interpersonal relation, stigma, and antipsychotic medication. 11 We suggest that depression should be ruled out first as it is the commonest psychiatric disorder implicated in FSD and associated with more severe sexual dysfunction compared to OCD and GAD and thus, specific treatment should be started for psychiatric disorders as early as possible.9,13,33,35
The most common physical comorbidity was hormone-related abnormalities (26.03%) in the form of menopause or abnormal menstrual cycles followed by hypothyroidism, hyperprolactinemia, and diabetes mellitus. Menopause and abnormal menstrual cycles were found to be related to hormonal abnormalities as per previous studies.16,18,36 FSD was also found to be significantly and more frequently associated with chronic diseases affecting multiple systems such as thyroid dysfunction and both type 1 and type 2 diabetes.15,17,18 In our study, HTN was diagnosed in 5.48% of cases only. Studies have already shown evidence of an association between FSD and vascular risk factors, including HTN, obesity, diabetes, and coronary heart disease.10,15,37 As hormonal abnormalities have got detrimental effects on the sexual functioning of females, the physicians dealing with them, primarily the gynecologists and the endocrinologists, should focus on their sexual complaints along with proper investigations for thyroid hormone, prolactin, blood sugar, and sex hormone levels to promote early detection and treatment.16,35,38
The most common social comorbidities were husband-related issues (20.55%) followed by other family-related problems (15.07%) and domestic violence (2.74%). It is already established that impaired emotional and relational issues as a result of male partner’s sexual dysfunction, psychiatric comorbidities, and drug dependence can lead to FSD.1,20-23 Family-related issues like daily stressors, chronic stress in the family, and domestic violence at any point of the life of a female were also found to be associated with decreased sexual desire, arousal, orgasmic disorder, and vaginismus.24-26
Out of 73 patients, only 1 patient (1.37%) had sexual dysfunction without any comorbidity and the rest 72 patients (98.63%) were diagnosed as having sexual dysfunction with psychiatric comorbidities with some of them having physical as well as social comorbidities too, ie, they were having at least one among psychiatric and physical/social comorbidities or their various combinations (Table 3). Moreover, 13.70% of patients had all 3 types of comorbidities ie psychiatric + physical + social comorbidities. Thus, female patients reporting sexual complaints should be assessed from a biopsychosocial perspective to identify various interlinked factors associated with FSD. The aim should be to explore psychiatric disorders and social contributing factors in addition to diagnosing physical diseases, if any, through proper physical examination, biochemical, and hormonal assessment.2,6,15 The psychiatrist should play a key role in managing FSD, and thus, after establishing a complete diagnosis from a biopsychosocial perspective, intervention (medication/counseling or both) should be started for both psychiatric and social factors with appropriate referral, wherever needed, for the physical diseases to be managed in liaison with other specialties.38,39 As far as this 98.63% of patients with various comorbidities are concerned, proper management of the primary medical conditions, psychiatric disorders, and social comorbidities might convert the more severe cases of FSD to less severe ones which again might lead to a significant improvement and even complete recovery in some cases as suggested by the previous studies.36,38 Thus, being aware and identifying these factors along with their effect is an essential aid for health care professionals (including the primary care physicians and gynecologists who are the first point of contact for many) in the prevention of significant morbidity, early diagnosis, and holistic treatment of sexual dysfunction as the severity increased with longer duration of FSD.6,38 For this, the authors feel that there is a need to train primary care physicians and gynecologists so that they remain unbiased while referring the patients with sexual issues to respective specialists (for the management of the physical comorbidities) and psychiatrists for specific intervention as most of the comorbidities can be treated while social issues can be managed by social intervention and counseling.39,40 Females often do not seek treatment and try to live with the problem because of the nature of the problem and its psychological consequences. In India, treating physicians often give less attention or importance to patients’ sex-related problems. 41 The influence of social and cultural issues and misconceptions about sexual functions cannot be denied and requires more research.27,28,42-44 However, the findings of the study indicate that exploration of comorbidities and targeting them during treatment in addition to accepted methods may increase the outcome of treatment of FSD.
Strengths and Limitations of the Study
In the absence of studies on a combined assessment of physical, psychiatric, and social comorbidities in FSD, the integrated approach in the assessment of all these factors for complete diagnosis and holistic treatment, use of a homogeneous group of patients, and assessment of the severity of FSD added credibility to our findings. However, in this study, we focused mainly on medical and psychiatric disorders with less exploration of lifestyle, psychological, and relationship factors. The investigations were restricted to the facilities available in our hospital. Future studies with bigger sample sizes and drug naïve or drug-free patients with inclusion of psychological and relationship issues, more social as well as lifestyle factors, and comparison with a control group might provide more robust evidence.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors to conduct the study and to prepare the manuscript. The study did not receive any outside support.