
Abstract
Background:
Sexual function and satisfaction are 2 important components of sexual health. Both sexual function and satisfaction of women are influenced by various internal and external factors over their life cycle. This study aims to explore the factors of sexual function and satisfaction among nonworking married women in Bengaluru using a qualitative exploratory study.
Materials and Methods:
This is a qualitative exploratory research study that adopted an inductive thematic data analysis. In-depth qualitative interviews were conducted with 11 nonworking working married women of Bengaluru. The interviews were audio recorded, and the transcribed data were analyzed with ATLAS.ti software. The results were presented thematically.
Results:
It was found that somatic and personal factors such as health and appearance, pregnancy and postpregnancy issues, compatibility between couples, and spousal qualities; psychological factors such as stressors and stabilizers that related to emotional and mental health; and situational and extrinsic factors such as pressure to conceive, child-rearing, types of family, traditional beliefs and practices, societal stigma and taboo, daily schedules of couples, and ambiance and privacy were influencing the sexual function and satisfaction of women.
Conclusion:
The study could find positive and negative factors of sexual function and satisfaction. These factors need further exploration with larger studies from other cultures and groups.
Introduction
Sexual health is a part of well-being and is described as the state of physical, emotional, mental, and social well-being concerning sexuality, and not merely the absence of disease and dysfunction. 1 It is having a respectful sexual relationship with a pleasurable sexual experience, free of coercion and violence, and protecting the sexual rights of an individual. 1 Sexual function and satisfaction are 2 important indicators of sexual health that determine the quality of relationship between the married couple. 2 The normal sexual function among women includes 5 dimensions: desire and subjective arousal, lubrication, orgasm, satisfaction, and pain/discomfort. 3
The literature on sexual functioning reports that psychological and interpersonal factors influence sexual function. Psychological factors of sexual function in adults are stress, depression, anxiety, guilt, fear of intimacy, unreasonable expectation, impaired self-image, and attachment anxiety.4-6 Interpersonal factors of sexual function of adults were poor emotional intimacy, poor communication, romantic attachment, body appreciation, partner performance, partner-prescribed sexual perfectionism, partner’s personality traits (optimism), emotional support from partner, and relationship satisfaction.5–8 Restricted upbringing, disturbed family relationships, level of education, and socioeconomic status also indirectly influence sexual function.5,9
Sexual satisfaction is an effective response arising from one’s subjective evaluation of positive and negative dimensions associated with one’s sexual relationship, 10 and it is closely related to and depends on the sexual function and relationship of couples. 2 Studies reported several factors of sexual satisfaction, such as intrapersonal, interpersonal, clinical, sociocultural, and family factors. Intrapersonal factors include sexual motives, psychological well-being, menopausal symptoms, poor sexual self-esteem, poor sexual function, relationship satisfaction, and no previous information about sexuality.11-14 It was also observed that aging, the age difference between couples, diabetes, rheumatoid arthritis, menopause, urinary incontinence, genital tract surgeries, obesity, infertility, depression, anxiety, miscarriage/recurrent pregnancy loss, and substance abuse are significant factors of sexual satisfaction among adults.15,16 Interpersonal factors of sexual satisfaction of adults were poor partner communication, 12 good interpersonal communication skills, social skills, conflict resolution skills, mutual pleasure, marital satisfaction, frequency of sex, and relationship adjustment.12,14,15,17 Sociocultural and family factors of sexual satisfaction are beliefs and attitudes about sex, sociocultural taboos, lower economic level, number of children, family responsibilities, perception of sexual talk as taboo, educational status, and working status.13,15,18
Studies found that there is a high prevalence of sexual health-related problems in India, especially among women.19,20 Some researchers have recommended that there is a need for more studies to explore factors of sexual function and satisfaction among women.5,15,21 A few studies have reported that the working status has a significant impact on sexual function and satisfaction.15,22 Hence, this study aims to explore various factors of sexual function and satisfaction among nonworking married women.
Materials and Methods
Ethics
This study is approved by the Institutional Review Board (CU: RCEC00075/7/19). Written informed consents were sought from all the participants before the study. Participants were given the right to withdraw from the study at any point during the study. Participants’ identities were anonymized during the data storage and transcription by giving pseudonyms, and the data were stored in a password-protected drive that has access only to the authors.
Study Design
This is a qualitative exploratory study. It has adopted inductive thematic data analysis. 24 Though there are studies21,23 exploring the sexual function and satisfaction among clinical population, but there is a dearth of literature on nonworking married women. Hence, to explore this gap, we have adopted an exploratory research with the inductive thematic analysis. 24
Study Setting and Participants
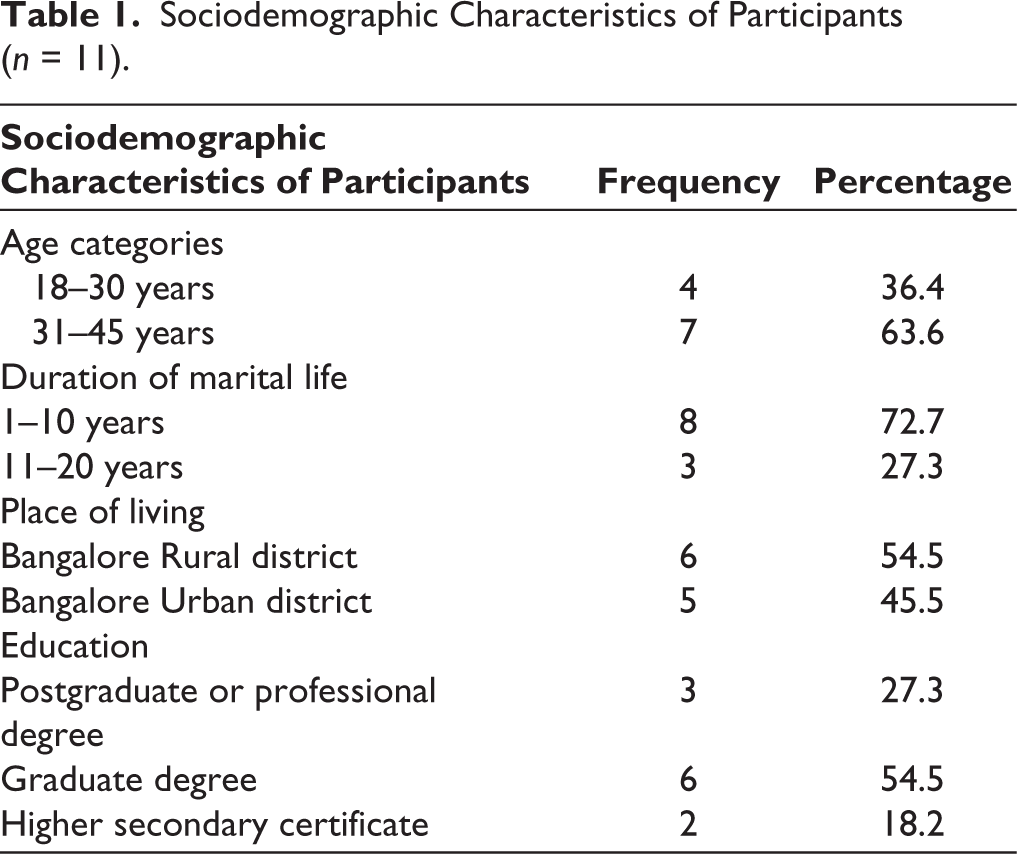
The study was conducted in Bangalore Urban and Rural districts among nonworking married women who were above 18 years old and living with their spouses. The women who had any clinical conditions, reached menopause, were divorced or separated, and were married for less than 6 months were excluded for the study. The study’s information was disseminated through social media and the personal contacts of the first author. Initially, 2 participants were purposively selected from Bangalore Rural and Urban districts based on the inclusion criteria. Subsequently, these 2 participants were asked to introduce or provide contacts of nonworking married women who potentially met the selection criteria. When a participant introduced or provided the contact information of another potential study participant, the first author screened them to rule out any of the exclusion criteria. Women who had been diagnosed with physical or mental illnesses were excluded from the study, as were their spouses if they had also been diagnosed with any physical or mental illnesses. A total of 13 participants were eventually screened and 2 were excluded for not meeting the criteria. Initially, 2 participants were purposively selected from both Bangalore Rural and Urban districts based on the inclusion and exclusion criteria. Later, additional samples from each category were chosen through their contacts. We used 2 criteria to determine data saturation. The first criterion involved the frequency count of codes, where a code repeated a total of 3 times during the coding process. 25 The second criterion was an a priori stopping point for data saturation. 26 According to this criterion, once all codes were adequately explored (with a minimum frequency count of 3), we conducted an additional 2 interviews to conclude the data collection. Data saturation was reached after the ninth participant, but we collected 2 more samples as per the data saturation criteria outlined in the “Data Analysis” section. Subsequently, further data collection was discontinued. The sociodemographic characteristics of the participants are given in Table 1.
Sociodemographic Characteristics of Participants (n = 11).
Procedures
An in-depth interview guide was developed based on the review of the literature and consultation with experts working in the field. It included a set of semistructured and open-ended questions about the various determinants of sexual function and satisfaction of women. 27 However, it has not been restricted to only the interview guide, but the emerging issues during the interview were explored through the dialogue between the interviewer and interviewee. The study was conducted during the COVID-19 pandemic lockdown in June and July 2020. Telephonic interviews were conducted with the participants on the prior schedule by following the guidelines proposed by Whiting with an audio recording. 28 The duration of the interviews ranged from 30 to 45 minutes.
Data Analysis
The audios were listened to multiple times to get familiarity with the language. They were transcribed and translated by the first author. Later, they were checked for consistency by the second author. The inductive thematic analysis was conducted 24 using ATLAS.ti (Student Licensed) qualitative data analysis software. The first author listened to the audio and transcribed the recordings into text in a verbatim format. The second author trained the first author in managing transcriptions using the software and the coding process before data analysis. The second author cross-checked the audios against the transcriptions to ensure the retention of the essence of the participants’ narratives and to maintain consistency. As the first step, a coding framework was developed based on the first 2 transcriptions. Both the first and second authors read the first 2 transcriptions line by line together multiple times to become familiar with the data and generate initial codes. Factors related to sexual function and satisfaction, prevalent in the text segments, were carefully identified and coded. Any disagreements related to code names were resolved through discussions. On the basis of this initial coding framework, the first author continued concurrent coding with data collection for subsequent transcripts. The second author supervised the coding process throughout the data analysis. Data saturation occurred with the ninth participant, as indicated by a frequency count of codes, 25 and we concluded data collection after adding 2 more samples with stopping criteria, 26 which are explained in the “Study Setting and Participants” section. Subsequently, the second author rechecked the codes against the transcriptions to ensure the retention of the participants’ narratives’ essence. Any deviations from the participants’ narratives were identified, discussed, and resolved between the authors. Therefore, 2 rounds of code revisions were conducted before finalizing all the codes and merging redundant codes with those having similar meanings. Later, these codes were grouped according to their meanings and collated with other codes to derive themes. These themes were reviewed, defined, and named based on their specific and distinct characteristics. Finally, the themes and codes were checked against transcriptions to see whether the essence is retained. Later, the themes were presented with participants’ excerpts. To report the study and its findings, standards for reporting qualitative research guidelines were followed. 29
Results
Three global themes were found from data analysis: (a) somatic and personal factors, (b) psychological factors, and (c) situational and extrinsic factors with specific organizing and basic themes.
Somatic and Personal Factors
These factors are related to one’s own body and the characteristics of couples which have either positive or negative influence or direct or indirect influence on their sexual function and satisfaction. Under this global theme, 2 organizing themes were found: physical factors and couple’s characteristics that are purely intrinsic.
Physical Factors
The participants described various physical factors of their sexual function and satisfaction and grouped them under personal health and appearance and pregnancy and postpregnancy issues.
Personal Health and Appearance
Personal hygiene, physical well-being, physical discomfort, menstrual difficulties, infections, and body image were the emerged factors under this theme. They narrated that personal hygiene and physical well-being are favorable factors, whereas physical discomforts because of thyroid issues, fatigue, and various medications are unfavorable factors.
Participant “Vaishnavi,” a 39-year-old woman, said, “Having hygiene is very important. I will never get involved unless I am feeling good enough that I am.”
Menstrual difficulties, urinary tract infections, and body image act as the major block to sexual life especially. The analysis pointed out that physical beauty, attractiveness, and neatness are important in sexual life.
Five participants told “menstrual difficulties, which include physical and psychological issues like pain, PMS, mood swings and anger, etc.” cause, tough times for women and it directly or indirectly affects their sexual health.
Pregnancy and Postpregnancy Issues
Pregnancy and postpregnancy issues, such as pain, vomiting, mood swings, and medications, act as obstacles in sexual life. Similarly, the drastic changes in the body after pregnancy and childbirth cause serious concerns about their body image. This leads to a low drive for intimacy and sex for a while.
Couple’s Characteristics
Couples’ characteristics such as compatibility between couples, spousal qualities, and sexual health awareness among couples have a direct or indirect influence on women’s sexual health.
Compatibility Between Couples
The participants narrated that mutual understanding is an important factor that means knowing and sticking to each other’s comfort level, feelings, emotions, and needs. It has a positive impact on their overall sexual health. Mutual decision-making, interest and consent in sexual life, cordial relationship and intimacy, admiring and honesty, and open communication are other important factors highlighted by the participants.
Participant “Swati,” a 30-year-old woman, described that “we stick to what we know and we stick to each other’s comfort level. If I am not comfortable, he does not force me to do that. And it goes vice versa. Hence, we decide mutually and we know each other well.”
Spousal Qualities
Participants revealed that the husband’s certain qualities such as compassion and concern about sexual intimacy as positive factors and verbal abuse, comparing with others, criticizing in others’ presence, and lying as negative factors have a direct influence.
Participant “Nithya,” a 25-year-old woman, said “The spouse should have positive regard for his wife. He should understand what the other person is feeling, what is her comfort, all those things are favorable for women.”
Psychological Factors
Under this global theme, the participants discussed emotional/mental health factors including both stressors and stabilizers.
Emotional/Mental Health
The emotional/mental health factors are grouped into stressors (favorable factors) and stabilizers (unfavorable factors).
Stressors
According to the participants, stressors that act as the negative factors of sexual function and satisfaction are stress, mood swings, and anger. Six participants of the study strongly revealed that stress is the major factor that affects their overall sexual health and indirectly affects their physical and mental health, and it gradually leads to bad sexual health.
Participant “Revati,” a 34-year-old woman, said, “Stress and strain are the negative factors in my life which are negatively influencing my sexual life.”
Stabilizers
Participants narrated that emotional stability and happiness are important positive factors in their sexual health. It helps to have a healthy life, especially with the sexual relationship and intimacy with their spouse.
Situational and Extrinsic Factors
The third global theme includes the factors present in the environment and have any kind of influence on the sexual health of women. These are not related to any internal aspects of couples and are extraneous, grouped into 3 organizing themes such as family, sociocultural, and environmental factors.
Family Factors
These are the factors related to the immediate or extended family of couples who have any influence on their sexual health, including pressure to conceive, child-rearing, and type of family.
Pressure to Conceive
According to the participants, pressure to conceive, the intrusion of family members in a couple’s life, and expectations and demands from families act as major barriers to their overall sexual health.
Participant “Shahla” a 34-year-old woman, described “after marriage the pressure for kids was high from both families. The pressure was too much and a really bad experience that affected our sexual health.”
Child-rearing
In this, factors such as parenting responsibilities, changes in routine owing to children, and tiredness and stress associated with the same have either independent or combined effects on women’s sexual health. With child-rearing factors, women need to be more occupied with and for children and need to provide more attention and time to children than the initial period of their marital life. This leads to having less personal time and freedom for the women and becoming more tired and stressed.
Types of Family
The influencing factors explored under types of families are orthodox and heterodox families. The participants from heterodox family backgrounds agreed that they got support and appropriate knowledge on sexual health at the right time, whereas participants from orthodox family backgrounds told, they did not. According to them, a heterodox family is a favorable factor, and an orthodox family is an unfavorable factor in their sexual life.
Sociocultural Factors
The sociocultural factors of the sexual health of women include traditional beliefs and practices and societal stigma and taboos.
Traditional Beliefs and Practices
The religious practices in the family, cultural beliefs and practices, the age difference between couples, and early marriage at the age of 18 to 21 are the major factors under this theme. According to the participants, cultural and religious practices have an indirect negative influence on their sexual life, as couples have to follow some strict rules and regulations. The huge age difference between couples determines the relationship, especially, the way of expressing love and affection to the partner acts as a negative factor in the sexual life of couples. It is also associated with the factor of early marriage at the age of 18 to 21 years and has a huge negative impact on the sexual health of women.
Participant “Bhavya,” a 26-year-old woman described, “I got married when I was 18, and in our tradition due to caste and cultural practices, and being a very orthodox family, they do our marriage within 21 years. At that age I was not prepared, I was studying, didn’t know anything about sexual and marital life, and was not prepared for marriage. Intimacy was not there between us because of all these and I was not interested in leading a sexual life.”
Societal Stigma and Taboo
This theme includes stigma from society toward sex, the cultural taboo about sex, and religious stigma toward sex that have an indirect negative influence on the sexual life of women as it acts as a barrier to early sexual health education for girls from family, schools, and religion.
Participant “Shahla” a 34-year-old woman, told “I didn’t get any advice about after marriage and sexual life, instead, I was advised on how I should treat my husband. The main factor in marital life is sexual life. But, our culture following orthodox beliefs and practices is not giving any importance to sexual life. It is something like you should not talk about sex and talking about sex is bad.”
Environment Factors
The daily schedule of couples and ambiance and privacy are the 2 basic themes that emerged under the third organizing theme environment.
The Daily Schedule of Couples
The lengthy and tiresome days, the work pressure of the spouse, and exhausting household work are unfavorable to the sexual function and satisfaction of women. According to them, these factors cause physical burden, tiredness, and back pain that badly affect their physical and mental health and gradually lead to bad sexual health. Also, the data reveal that the husband’s work pressure and heavy work, tired or bad or long days of couples (individually or together), busy life schedule, unevenness and imbalance in daily life, etc act as the adverse factors in the sexual life of women.
Ambiance and Privacy
According to participants, good ambiance and privacy are favorable factors of sexual function and satisfaction of women. The delightful atmosphere and comfortable places act as the positive factor, and women expect the same in their life.
Discussion
As presented in the results, the study found important factors that influence or impact sexual function and satisfaction. They are (a) somatic and personal factors, (b) psychological factors, and (c) situational and extrinsic factors.
Somatic factors such as personal hygiene and physical well-being positively influence sexual function. However, factors such as menstrual difficulties, urinary tract infections, body image, and pregnancy and postpregnancy health and body changes emerge as the unfavorable factors. Among the somatic factors, urinary incontinence is corroborated with a previous study. 15 All other somatic factors in this study are considered novel. Some of the previous studies have reported that thyroid-related issues impact sexual function.9,30 But none of the participants in this study have reported that it affects sexual function.
The personal characteristics of the couple such as mutual admiration and honesty, consense in sexual life, cordial relationship, mutual understanding and decision-making, open communication, compassion, and understanding emotions of each other are considered favorable for sexual function and satisfaction. Some of the previous studies supported that various aspects of physical and emotional intimacy between the partners are significant predictors of sexual function and sexual satisfaction among couples.31,32 Studies found that poor emotional intimacy, communication, and emotional support from the partner were considered adverse factors of sexual function.5,8 Some of the studies found that poor communication and lack of prior information about sexuality adversely impact sexual satisfaction.13,33,34 However, the literature also suggests that social skills and conflict resolution among couples were identified as favorable factors of sexual satisfaction.13,15 Among those factors, verbal abuse by the spouse was identified as novel.
Previous studies found psychological factors such as stress and anxiety are considered the negative factors of sexual function and satisfaction that are in tune with our results.4,5,9 The current study also found other factors, such as anger, mood swings, emotional stability, and happiness, may impact sexual function and satisfaction. Some of the previous studies reported that psychological well-being and stable mental health influence the sexual satisfaction of women 12 and psychological stress negatively associated with sexual function of women. 9
Sexual satisfaction also influences the family factors such as the number of children and family responsibilities. 15 The finding of this review article indicates that the sexual satisfaction of women is negatively affected by the increase in the number of children and various family-related responsibilities and demands. 15 However, the current study finds that some unique factors, such as pressure to conceive, child-rearing practices, and orthodox family background, negatively impact both sexual function and satisfaction.
Sociocultural factors such as traditional beliefs and practices and societal stigma and taboos are identified as the influencing factors. These findings are in tune with other studies.13,15 These studies found that such existing traditional cultural and religious practices and stigma and taboo on the sex topic were acting as a barrier in the sexual life of couples in terms of their satisfaction and relationship. Another empirical study observed that fewer beliefs related to sexual desire as a sin acted as a favorable factor of sexual function among heterosexual women. 35
However, this study finds a unique result that age differences between couples and age at the time of marriage are unfavorable factors for both sexual function and satisfaction. The situational and extrinsic factors such as the daily schedule of couples and ambiance and privacy of sexual function and satisfaction of women are unique since no literature found similar to these findings.
Strength and Limitations
Since the interviews were conducted by the first author who is a female, the participants were comfortable during the interviews and could share rich information that was very sensitive and personal to them. The researcher’s immersion in each phase of the study, especially interview guide development, data collection, data analysis, and reporting, ensured trustworthiness. The study was conducted with rigor—the audio recordings were listened to multiple times, transcribed, and translated. The transcriptions were then cross-checked against the audio to ensure consistency and the retention of essence. Additionally, both authors participated in the development of the coding framework, and the codes were checked against the transcriptions to ensure consistency and the retention of the essence of the participants’ narratives. As the study used an inductive approach, importance was given to the emergence of themes. Also, the codes were cross-checked by 4 participants and verified for consistency. All these contributed to qualitative rigor. However, the study has limitations, such as telephonic interviews where it was difficult to collect nonverbal data. Also, the study was conducted during the COVID-19 pandemic, which could potentially influence the participants’ narratives. Another limitation is that, despite including participants from both rural and urban areas of Bangalore, we were unable to conduct subgroup analysis. Therefore, future studies could explore differences between rural and urban populations, as well as between working and nonworking or homemaking women, to gain valuable insights. The other limitation is the absence of inter-rater reliability for code agreement.
Conclusion
In conclusion, the study could identify positive and negative factors related to sexual function and satisfaction among nonworking married women. The positive factors of sexual function and satisfaction are personal hygiene, physical and psychological well-being of women, and mutual interest. The negative factors are menstrual health issues, verbal abuse by the spouse, lack of sexual health awareness, and stress and emotional issues. However, these factors need to be explored further with larger studies from other cultures and groups.
Footnotes
Author Contributions
AAP and ACA have significantly contributed to the study’s conception and preparation of the study protocol. AAP collected the audio-recorded data and transcribed and translated it. Both AAP and ACA participated in the qualitative data analysis. AAP conducted the review of literature and prepared the first draft of the manuscript. Both AAP and ACA read the manuscript and revised and approved the final version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval
This study is a part of the PhD thesis of the AAP. It is conducted according to the principles of the Declaration of Helsinki 1964 and its latest amendments. The study proposal and related documents were approved by the Institutional Review Board of CHRIST (Deemed to be University), Bengaluru, India (Date: July 19, 2019; Ethical Approval No. CU: RCEC/00075/7/19). The study has been registered with the Clinical Trials Registry, India. Trial Registration No. CTRI/2020/06/025503.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.