
Abstract
Background:
Sexual satisfaction in marriage is paramount and key to marital satisfaction and happiness.
Aims:
This study is aimed at determining the prevalence and impact of marital sexual relationship-focused premarital counselling on sexual satisfaction among married women.
Setting and Design:
A total of 473 married women participated in this cross-sectional survey design; data was generated online utilizing Google form.
Method and Material:
Sexual satisfaction sub scale of Female Sexual Function Index was used in collecting data.
Statistical analysis used:
Chi-square and Univariate Analysis of Variance were used in testing the hypotheses in this study at 0.05 significance level.
Results:
Findings revealed high prevalence of marital sexual relationship focused premarital counselling among married women, with 73.6% of the married women in the study counselled on marital sexual relationship prior to their marriage, χ2 = 105.135, p = 0.0001 (p < 0.05). Similarly, outcome of hypothesis two revealed significant difference in terms of prevalence of people that render marital sexual relationship focused premarital counselling, with 29.6%, 26.6%, 8.0%, 4.9%, 3.0%, 0.6%, 3.0%, 0.4% and 0.4% respectively, that were educated by pastors, mother, female friend, aunt, grandmother, mothers’ friend, step mother and Imam, χ2 = 540.918, p = 0.0001 (p < 0.05). Finally, result of hypothesis three revealed that marital sexual relationship focused premarital counselling have significant impact on sexual satisfaction, means; 1.57, 1.44, F (1,471) = 5.923, p = 0.015 (p < 0.05). Participants that were counselled on marital sexual relationship had mean sexual satisfaction score of 1.57, while those that were not counselled had mean sexual satisfaction score of 1.44.
Conclusions:
Findings of the study is an implication for marriage counsellors and other professionals that handle marriage related issues to be intentional in addressing marital sexual relationship issues during premarital counselling and there is need to develop marital sexual relationship premarital counselling guide which can help in addressing issues concerning marital sexual relationship during premarital counselling.
Keywords
Introduction
Sexual satisfaction in marriage is paramount and key to marital satisfaction and happiness. However, some couples are dissatisfied with their sexual life because of sexual dysfunction. Prevalence of sexual dysfunction is on the increase globally; unfortunately, most couples suffer from sexual dysfunction without knowing what exactly they are suffering from. Sexual dysfunction and inadequate knowledge of marital sexual relationships affect couples’ sexual life, especially in the area of sexual satisfaction. 1 Sexual satisfaction is defined as emotional satisfaction and satisfaction in sexual activity. Also, 2 defines sexual satisfaction as experiencing positive feelings and pleasant sexual experiences after sexual intercourse. According to 3 sexual satisfaction is significant in determining marital life stability. Most couples consider sexual satisfaction as a personal matter and an important factor in marriage. 4 Among spouses, one of the determinants of marital satisfaction is satisfied healthy sexual relationship. 5 This implies that dissatisfied marital sexual relationship affects marital happiness and satisfaction. Thus, 6 recommends development of premarital counselling and continuous educational programs.
The quality of sexual satisfaction and sexual relationships among couples is improved by marital counselling. 7 Among Iranian couples, 8 discovered that group psychoeducation increases sexual functioning. In marital dissatisfied sexual relationships among couples, sexual counselling is used for intervention. 5 Premarital counselling and sex education can improve sexual satisfaction. 9 Individuals acquire knowledge and information about their sexual attitudes, issues, values and beliefs through sexual counselling. Sexual counselling helps in improving marital health, healthy sexual development, affection, closeness, interpersonal relationship, gender roles and body image. 10 Quality of marital life and sexual satisfaction can be improved by sexual health educational and counselling programs. 11 Premarital counselling raises levels of a couple’s sexual health knowledge. 12 Among newlywed Iranian women in a quasi-experimental study, 13 reported that sexual health-focused premarital counselling and educational intervention help in improving marital relationships of the couples.
In a randomized trial conducted among women in Hamadan Heath Centre, counselling was found to be successful in improving libido and sexual satisfaction. 14 Furthermore, sexual counselling improves sexual intimacy and sexual satisfaction among breastfeeding women. 15 Among women with sexual dysfunction, 16 recommend the implementation of counselling in increasing levels of sexual satisfaction. Among married individuals in Ebonyi State University, Nigeria, 17 discovered that couple’s attitude towards sex, amount of physical affection, intimacy; foreplay, coital and orgasm frequency were perceived to significantly improve sexual satisfaction. According to 18 among women sexual concerns are some of the common issues reported to health professionals. Thus, 19 recommends that women suffering from sexual disorders should be encouraged not to die in silence but to seek professional intervention.
Satisfied sexual life determines satisfaction with life and marital satisfaction among married women. 20 No wonder, a study in Anambra state Nigeria, 21 recommends that premarital counselling should be compulsory for intending couples which will help them in handling marital issues. Similarly, 22 recommends that importance of premarital counselling should be emphasized by churches and religious bodies. Higher sexual satisfaction was found among men and women in experimental group that attend premarital sex counselling compared to those in the control group. 23
Sexual satisfaction is an important factor in determining happiness among couples. Premarital counselling by trained professionals to handle sexual-related issues plays a significant role in determining satisfied sexual relationship in marriage. However, marriage counselling mostly in Nigeria is conducted by clergies and or people who are not trained to do so such as parents of the intending bride on most occasions. Even among the clergies most of them are not trained to handle sex-related issues in marriage such as sexual dysfunctions and sexuality in general. Some of the bride’s mother and sometimes friends attempt to address sexual-related issues but in an unprofessional way. In most cultures in Nigeria, intending couples most especially women are counselled on submission to their husband in marriage, this enlightenment is mostly done by the women folks. Although, it seems that the area of marital sexual relationships is neglected or little is done in that area during premarital counselling. The aforementioned is the problem identified in this study
6
recommend developing premarital counselling and continuous education programs. While
19
recommends that women should not die in silence but seek professional intervention. Thus, this study is aimed at determining the prevalence and impact of marital sexual relationship-focused premarital counselling on sexual satisfaction among married women. Therefore, the following hypotheses were tested;
Prevalence of marital sexual relationship-focused premarital counselling will be high. Prevalence of people that counsel the bride-to-be regarding marital sexual relationships will significantly differ. Marital sexual relationship-focused premarital counselling will have a significant impact on sexual satisfaction among married women.
Method
Design
This study was designed as a cross-sectional survey conducted among a sample of Nigerian married women who were married between few days of marriage to twenty (20) years of marriage. Snowball sampling technique was utilized in data collection, the questionnaire was designed using Google Forms, and participation consent form was attached to the online Google form. The link to the questionnaire was sent to participants that met the inclusion criteria through WhatsApp via their mobile phones and each participant was requested to also forward the link to their married female friends that met the inclusion criteria.
Inclusion/Exclusion Criteria
Only married women that were married between few days of marriage and twenty (20) years of marriage were eligible to participate in the study. Married women who were married for more than 20 years and those who were singles were excluded from the study.
Participants
A total of 473 married women with mean age of 33.52 participated in this cross-sectional study. Majority 137 (29.0%) have only one child each, 116 (24.5%) have two children each, 89 (18.8%) had no child. Furthermore, 71 (15.0%) have up to three children, respectively, 42 (8.9%) have four children each, 9 (1.9%) have five children each, 8 (1.7%) have six children each and only 1 (0.2%) have up to seven children. In relation to religion, most 417 (88.2%) identify their religion as Christianity while 56 (11.8%) identify their religion as Islam. Majority 348 (73.6%) responded yes to the question ‘were you counselled on marital sexual relationship before you got married?’ while 125 (26.4%) said they were not counselled. In response to the question ‘who educated you on marital sexual relationship?’ among those that were educated on marital sexual relationships, majority 140 (29.6%) said they were educated by their pastor, 126 (26.6%) by their mother, 38 (8.0%) by their female friend, 23 (4.9%) by their aunt, 14 (3.0%) by their grandmother, 3 (0.6%) by their mother’s friend and 2 (0.4%) by their stepmother and imam, respectively. In terms of duration of marriage, majority 367 (77.6%) were married between a few months to 10 years while 106 (22.4%) were married between 11 years and 20 years.
Instruments of Data Collection
Demographic Information Questionnaire
Demographic information questions were designed to record the demographics of participants which include age, duration of marriage, number of children, religion, you were counselled on marital sexual relationships before you got married? Who counselled you on marital sexual relationship before you got married? If no skip to the next question; the demographic information questions were attached to the online Google form that was sent to participants.
Female Sexual Function Index
Sexual satisfaction sub-scale of female sexual function index developed by 24 was used for data collection in this study. The scale was designed to assess different domains of female sexual dysfunction (desire/arousal, lubrication, orgasm, satisfaction and pain). The scale can discriminate between nonclinical and clinical populations. 24 Cronbach’s alpha values of 0.82 and higher were reported. Overall test-retest reliability was relatively high for all of the domains (r = 0.79–0.86) and for the total scale (r = 0.88). 24 Female sexual function index score was correlated with Locke-Wallace, satisfaction subscale (r = 0.57) has the strongest overlap with marital adjustment test. The scale has a divergent validity of (r = 0.41). 23
Ethical Consideration
Consent to participate in the study was sought individually, each participant that participated in the study consented to after reading the consent form attached to the online Google form. Participant’s confidentiality was assured as their responses would be anonymous. Participants were assured that information they provide is for research purposes only, as such participation is voluntary. WhatsApp was used to ensure participants’ confidentiality; this application is secured by end-to-end encryption; participants were informed that once they clicked submit their responses went online to the database without knowing the participant’s identity.
Procedure
Data for this study was collected utilizing online Google forms, the questionnaire link was sent to married female contacts of the researcher that met the inclusion criteria via WhatsApp and they were requested to forward the link to their married female friends that met the inclusion criteria, that is, women that married between few days of marriage and twenty (20) years of marriage. WhatsApp was used to ensure participants’ confidentiality; this application is secured by end-to-end encryption. Snowball sampling technique was utilized; each married woman whom the questionnaire link was forwarded to was also requested to forward same to her married female friends that met the inclusion criteria. Those that had responded already were instructed not to respond again in case the link is re-forwarded to them as participation is only once. On average, it takes about five minutes to complete the questionnaire. Upon completion of the questionnaire, each participant click submits and their responses are submitted anonymously to the database.
Data Analysis
Descriptive and inferential statistics were tested in this study. Chi-square and Univariate analysis of Variance (ANOVA) were used in testing the hypotheses in this study at 0.05 significant level. Hypotheses 1 and 2 were tested utilizing Chi-square and hypothesis three was tested with ANOVA. All data were analyzed using SPSS version 21.
Result
The result revealed that prevalence of marital sexual relationship-focused premarital counselling is high among married women, with 73.6% of the married women in the study educated on marital sexual relationships prior to their marriage, χ2 = 105.135, p = .0001 (p < .05). The hypothesis is supported. This implies that a high number of the women were counselled on marital sexual relationships before their marriage. Table 1 shows the details of the result.
Chi-square of Prevalence of Marital Sexual Relationship-focused Premarital Counselling Among Married Women.

The result of hypothesis two revealed that prevalence of people that render marital sexual relationship focused premarital counselling significantly differ, with 29.6%, 26.6%, 8.0%, 4.9%, 3.0%, 0.6%, 3.0%, 0.4% and 0.4% were educated by pastors, mother, female friend, aunt, grandmother, mothers’ friend, stepmother and Imam respectively, χ2 = 540.918, p = .0001 (p < .05). The hypothesis is supported. This implies that prevalence of people that render marital sexual relationships significantly differs. Results showed that majority of the women were counselled on marital sexual relationships by the pastors and mothers, respectively. Table 2 shows the details of the result.
Chi-square of Prevalence of People that Render Marital Sexual Relationship-focused Premarital Counselling.
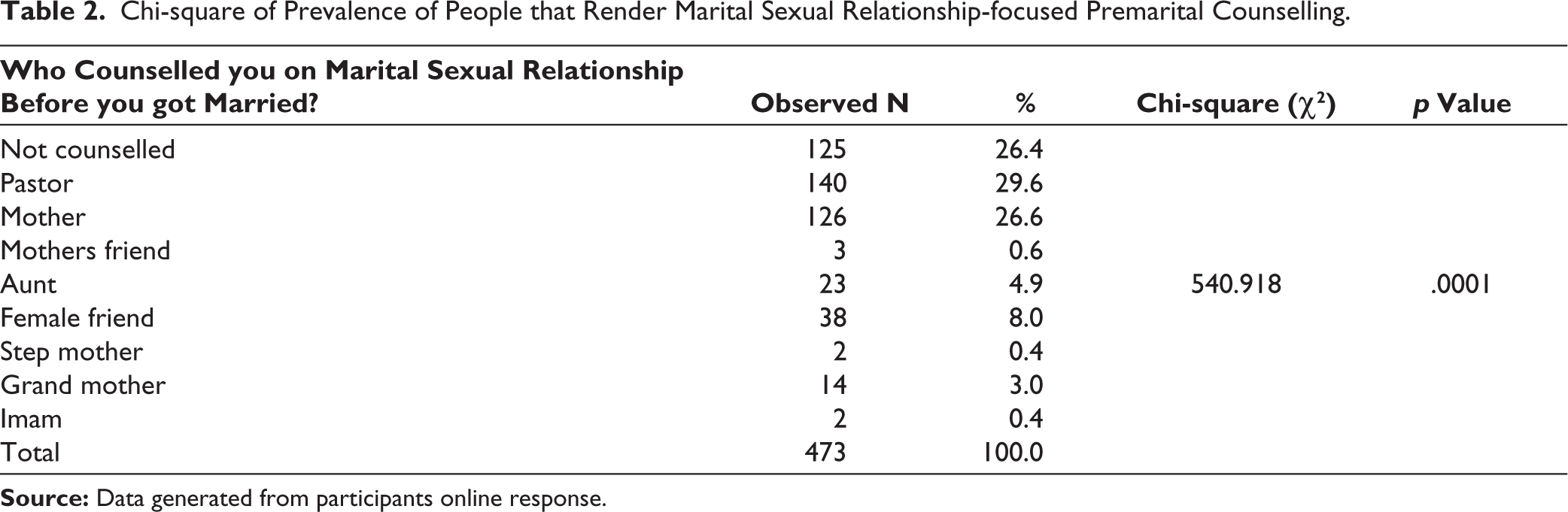
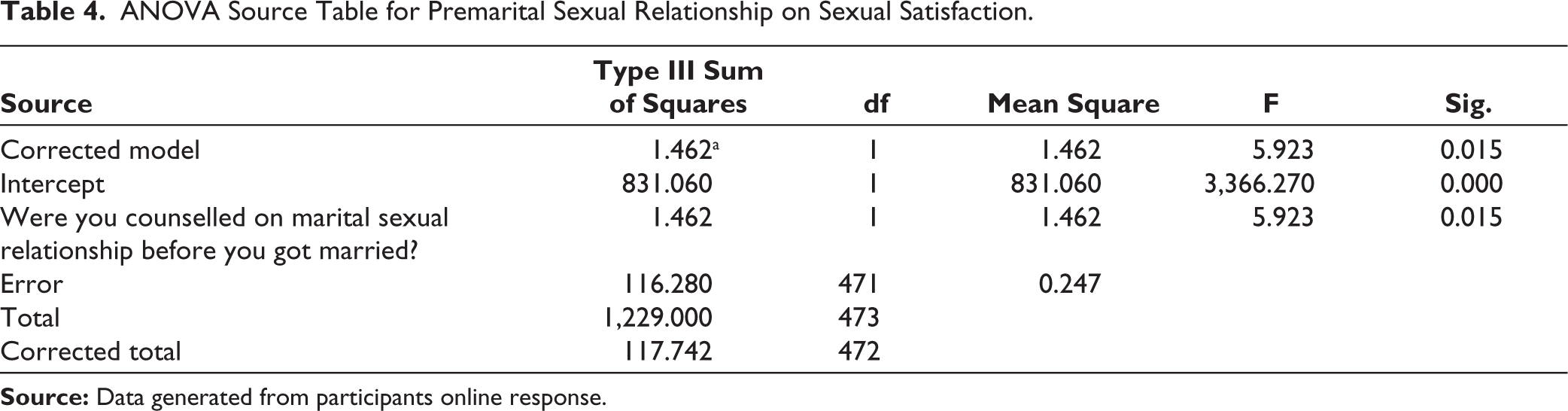
Table 3 reveals the mean, standard error, and the lower and upper bound scores on sexual satisfaction across marital-focused sex counselling. The table reveals that participants who were counselled on marital-focused sexual relationships had mean sexual satisfaction of 1.57, with 95% of participants that were counselled having scores ranging 1.514–1.618 (lower and upper bound). Participants who were not counselled had mean sexual satisfaction of 1.44, with 95% of participants that were not counselled having scores ranging from 1.353 to 1.527 (lower and upper bound). Participants that were counselled on marital sexual satisfaction before marriage had higher mean sexual satisfaction scores compared to those who were not. The result of Table 4 revealed that marital sexual relationship-focused premarital counselling has a significant impact on sexual satisfaction, means; 1.57, 1.44, F (1,471) = 5.923, p = .015 (p < .05). The hypothesis is supported.
Mean, Standard Error, Lower and Upper Bound Score of Sexual Satisfaction Across Marital Focused Sex Education.

ANOVA Source Table for Premarital Sexual Relationship on Sexual Satisfaction.
Discussion
Three hypotheses were tested in this cross-sectional study titled prevalence and impact of marital sexual relationship focused premarital counselling on sexual satisfaction among married women. Findings of the first hypothesis (see Table 1) revealed that prevalence of marital sexual relationship focused premarital counselling is high among married women. Outcome of the study showed that majority of the married women that participated in the study were counselled and or educated regarding sexual relation in marriage prior to their marriage (premarital counselling). Earlier, 23 had reported that individuals in experimental group that attend premarital sex counselling had higher sexual satisfaction compared to their counterparts that did not. Implementation of counselling has been recommended 16 increasing levels of sexual satisfaction. Result of the second hypothesis revealed that prevalence of people that render marital sexual relationship-focused premarital counselling significantly differs. Furthermore, findings of the study (see Table 2) showed that majority of the women that participated in this study were counselled on marital sexual relationships by the pastors and the women’s mothers, respectively. Only 125 (26.4%) of the study population said they were not counselled on marital sexual relationships prior to their marriage. No wonder, 22 recommends that the Church and religious bodies should emphasize the importance of premarital counselling. While 21 recommends that among intending couples premarital counselling should be made compulsory.
Outcome of hypothesis three (see Tables 3 and 4) revealed that marital sexual relationship-focused premarital counselling significantly impact sexual satisfaction. Women that were counselled on marital sexual relationships prior to their marriage had high sexual satisfaction mean score compared to those that were not. Earlier,7,10,13 reported that marital/sexual health-focused premarital counselling improves sexual satisfaction among couples. 6 recommend development of premarital counselling and continuous educational programs. Earlier, 9 concluded that premarital counselling and sex education can improve sexual satisfaction. Findings of this present study showed that married women that were counselled regarding marital sexual relationships irrespective of who counselled them had better sexual satisfaction compared to those who were not counselled.
Conclusion
In this study, the author concludes that, prevalence of marital sexual relationship focused premarital counselling is high, prevalence of people that render premarital sexual relationship focused premarital counselling significantly differ, and marital sexual relationship premarital counselling had significant impact on sexual satisfaction among married women. This study is limited due to the fact that only married women participate in the study and only online platform was used in data collection. Thus, men’s experience is not included in this study likewise women who do not have access to internet and or android phones could not participate which limits large number of women whose experiences could have been part of this study. However, findings of the study is an implication for marriage counsellors, psychologists and other professionals that handle marriage-related issues to be intentional in addressing marital sexual relationship issues during premarital counselling and there is a need to develop marital sexual relationship premarital counselling guide which can help in addressing issues concerning marital sexual relationship considering that mostly, marriage counselling in most communities is handled by lay helpers (those who are not trained marriage counsellors and or those not trained to handle marital sex-related issues). This implies that most individuals that render premarital counselling do that based on their personal experience which may be harmful depending on the lay counsellor’s negative or positive experience. Marital sexual relationship-focused premarital counselling is highly recommended for intending couples.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Participation in the study was purely voluntary and so an informed consent was obtained from each participant. Only those that consent to participate in the study were included. Aim of the study was clearly communicated to participants; their privacy and confidentiality were respected and ensured. Each participant was informed that she had the right not to participate and to discontinue participation at any time she wanted, without adverse consequences considering that participation in the study is purely voluntary.
Funding
The author received no financial support for the research, authorship and/or publication of this article.