
Abstract
Background:
Sexual satisfaction is a complex concept influenced by physical, psychological and socio-cultural factors. However, there is a lack of research on what determines sexual satisfaction among non-working married women in India. This gap hinders our understanding of how traditional gender roles, economic dependence and cultural norms affect the sexual well-being of this group. This study aims to explore the factors associated with sexual satisfaction among non-working married women in Bengaluru, India.
Materials and Methods:
A cross-sectional survey was conducted among 180 non-working married women. Data were collected using the New Sexual Satisfaction Scale, the Psychological Distress Scale, the Subjective Happiness Scale and a self-prepared questionnaire on various factors related to sexual satisfaction. Descriptive statistics and multiple regression were used to analyse the data.
Results:
Factors significantly associated with non-working women’s sexual satisfaction include physical factors (menstrual health difficulties, reproductive health issues and urogenital problems), psychological factors (psychological distress and subjective happiness) and socio-cultural factors (education, knowledge of sexual health at the time of marriage, type of marriage, age, age difference between couples and duration of marital life). Family-related factors (type of family, family pressure for children and exhausting household work) and couple-related characteristics (spouse’s smoking/drinking patterns and relationship with the spouse) were also significant. Together, these factors explained 78.6% of the variability in sexual satisfaction among non-working married women.
Conclusion:
The findings highlight the need for health interventions to promote healthy lifestyles and suggest changes in sexual health practices. They also indicate the need for training health professionals to address the sexual health aspects of women. Further longitudinal studies with larger samples are required to better understand the relationship between these predictors and sexual satisfaction.
Keywords
Introduction
Sexual satisfaction is an important indicator of sexual health. It is an affective response arising from one’s subjective evaluation of the positive and negative dimensions associated with one’s sexual relationship. 1 As this definition indicates, sexual satisfaction has both affective components, such as happiness, and evaluative components, such as a sense of success. 2 Sexual satisfaction is closely related to relationship satisfaction. 3 The Interpersonal Exchange Model of Sexual Satisfaction proposes that greater sexual satisfaction in a long-term heterosexual relationship is predicted by greater relationship satisfaction, a higher level of sexual rewards (what partners receive), less level of sexual costs (what partners contribute), comparison levels for sexual rewards and sexual costs and the perceived equality of sexual rewards and sexual costs.1,2 It is also closely related to relationship characteristics, personal values and sexual knowledge. 4 Mutual pleasure is a key element of sexual satisfaction, which derives from positive sexual experiences and not from the absence of any dysfunction. 3 Sexual satisfaction has two main aspects: ego-centred, which includes personal experience, and partner/sexual activity-centred, which includes the partner’s sexual behaviour/reactions, diversity and frequency of sexual activities. 5 Both of these aspects are understood based on sexual sensations, sexual presence/awareness, sexual exchange, emotional connection/closeness and sexual activity. 5
Sexual satisfaction varies among individuals based on gender, age and various other factors.6–8 Such factors can be intrapersonal, interpersonal, relationship-related or external.7–9 It has also been observed that heterosexual women have lower sexual satisfaction than men and have suggested more studies to explore various biological, cultural and psychological factors of sexual satisfaction. 6 The existing literature reveals that sexual satisfaction in adults is influenced by both favourable and unfavourable factors.8,10 Another study recommends that more quantitative studies are required to understand the individual, partner and relationship-related predictors of sexual satisfaction in adults. 11 A systematic review on predictors of sexual satisfaction among women pointed out that most of the studies focused on demographic and socio-cultural factors, while fewer studies found predictors such as sexual practices and physical health. 8 However, cultural differences in the predictors of sexual satisfaction are possible, as most of the studies included in this systematic review were from North America. 8 An international cross-cultural study explored demographic, psychological, socio-cultural and pathophysiological factors of sexual satisfaction among adults across different relationship statuses. 12 In a longitudinal study, 13 relationship satisfaction was identified as a significant predictor of sexual satisfaction among mixed-sex couples, with an average age of 34 years and an average relationship duration of 9 years.
A Korean study found that sexual frequency, marital satisfaction and cognitive function are key factors for sexual satisfaction in older men, while marital satisfaction, sexual frequency, absence of depression, age and length of marriage are key factors for older women. 14 It was also reported that morale and physical functions are significantly associated with the sexual satisfaction of older adults. 15 In Spanish older adults, sexual satisfaction was negatively correlated with age, low education, psychopathological symptoms and relationship length, while it was positively correlated with better physical health and relationship satisfaction. 16 These findings underscore the complex interplay of physical, psychological and relational factors that influence sexual satisfaction across various age groups and sexual orientations.
Though there is existing evidence for predictors of sexual satisfaction in women, studies particularly in the Indian context are lacking in the available literature. Additionally, this review pointed out that most of the studies consider single variables or one aspect of sexuality, which leads to inaccurate or inadequate evidence on the various possible factors of sexual satisfaction. 8 Another review on factors affecting sexual satisfaction in women particularly suggests that more studies need to be conducted to deepen the understanding of various socio-cultural contexts. 17 There is a gap in the literature regarding the factors influencing women’s sexual satisfaction in India. It is essential to explore the individual characteristics, partner dynamics, cultural influences, familial contexts and biopsychosocial factors that affect the sexual satisfaction of women in the Indian context.
This article aims to identify the significant predictors of sexual satisfaction among non-working married women in Bengaluru. The predictor variables for this study were initially selected based on the theoretical assumptions, evidence from the existing literature and findings from a qualitative study. 18 Based on the significant results of the bivariate analysis, the menstrual health difficulties, reproductive health issues, urogenital problems, psychological distress, subjective happiness, knowledge of sexual health while married, relationship with spouse, smoking (nicotine use) of the spouse, alcohol use of the spouse, type of family, family pressure for children, exhausting household work, education level of women, socio-economic status, type of marriage, age, age difference between couples and duration of marital life were selected as predictor variables for this study from the explored factors of sexual satisfaction from the qualitative study.18,19 Thus, this article aimed to answer the research question of how much these predictor variables explain the variance in sexual satisfaction among non-working married women. As the employment status of women has a significant influence on working women’s sexual satisfaction,17,20 and there is a dearth of literature on sexual satisfaction among non-working women, this study focuses on the predictors of sexual satisfaction in non-working women.
Methods
Ethical Considerations
The entire study was conducted with all ethical aspects considered at each phase to ensure the rights of participants, the rights of the academic and research community, and adherence to standards of reporting and publication. 19
Settings and Participant
The study used a cross-sectional survey research design 21 among 180 non-working married women above 18 years old, living with their spouses in Bangalore, India, selected through a mix of quota 21 and snowball 21 sampling methods. Recruitment was conducted through personal and professional connections, and participants were contacted in person. The total number of samples selected for quantitative data collection was 180 participants, of which 84 were from Bangalore Rural District and 90 from Bangalore Urban District. From each category, the researcher purposively selected the required samples based on the inclusion and exclusion criteria. The women who belonged to any clinical population, who had reached menopause, who were divorced or separated and who were married for less than 6 months were excluded. Additionally, the researcher tried to include women from different religions, castes and educational and occupational groups in both Bangalore Urban and Bangalore Rural Districts. The minimum and maximum ages of the participants were 21 and 45, respectively, with a mean age of 33.05 ± 5.71 years. The participants’ marital life duration ranged from 1 year to 11 years, with a mean of 9.73 ± 6.18 years. The age difference between the couples varied from 1 year to 11 years, with a mean of 3.89 ± 2.01 years. The socio-demographic characteristics of the participants are given in Table 1.
Socio-demographic Characteristics of Respondents (N = 180).
Tools for Data Collection
A detailed socio-demographic tool was used to collect the basic profile, health profile, couple’s characteristics and family profile. It was developed based on the identified factors of sexual satisfaction among non-working married women from the initial qualitative study 18 and was cross-checked for its cultural applicability through a pilot study. The sexual satisfaction of the women was measured using Stulhofer’s New Sexual Satisfaction Scale. This is a 20-item scale, and the internal consistency reliability of the scale is above 0.80 in various samples. The scale has test–retest reliability ranging from 0.72 to 0.84 over 4 weeks, with well-established construct validity. 5 The sexual satisfaction score can be obtained by adding the row score, which ranges from 20 to 100, with a score of 20 indicating lower sexual satisfaction and a score of 100 indicating higher sexual satisfaction. Kessler’s Psychological Distress Scale is used to measure psychological distress. It is a five-point Likert scale with 10 items and has good reliability and validity. The scores range from 10 to 50, with high scores indicating a high level of psychological distress and low scores indicating a low level of psychological distress. 22 The Subjective Happiness Scale with four items was used to measure subjective happiness. The scores ranged from 1 to 7, and the average score ranged from 4.5 to 5.5. The Subjective Happiness Scale has good reliability and validity. 23
Data Collection Procedure
The data were collected using the above-specified tools through personal interviews from November 2020 to February 2021. The personal interview was scheduled with each participant by prior appointment at their convenience. The duration of each personal interview ranged from 45 min to 1 h. The first author administered all the tools one by one to each participant after explaining the process in detail and obtaining their written consent. Out of the total data collected (N = 180), 26 responses were collected through Google Forms, as data collection was carried out during the COVID-19 pandemic.
Data Analysis
The obtained data were analysed using descriptive statistics and bivariate analysis such as the independent samples t-test, one-way analysis of variance, and Pearson’s product moment correlation tests initially with jamovi version 2.3.24,25 The predictor variables for the multiple regression of sexual satisfaction were initially selected based on the theoretical assumptions and evidence from the existing literature, and the final selection was done based on the significant results of the bivariate analysis of sexual satisfaction18,19 (refer to Tables 1–3 in the Supplementary Files). Then, the data were checked for the assumptions of multiple linear regression using the appropriate statistical analysis (refer to Tables 4–7 and Figures 1 and 2 in the Supplementary File). Multiple linear regression was conducted with the selected predictor variables to determine the prediction and variances caused by the sexual satisfaction of non-working married women.24,25
Results
The multiple regression results for the outcome variable, sexual satisfaction of non-working married women, with the predictor variables such as psychological distress, subjective happiness, menstrual health difficulties, reproductive health issues, urogenital problems, type of family, family pressure for children, type of marriage, exhausting household work of women, smoking (nicotine use) of the spouse, alcohol use of the spouse, knowledge of sexual health while married, relationship with spouse, education level of women, socio-economic status of women, age, age difference between couples and duration of marital life are presented in Table 2.
Multiple Regression of Sexual Satisfaction of Non-working Married Women (N = 180).
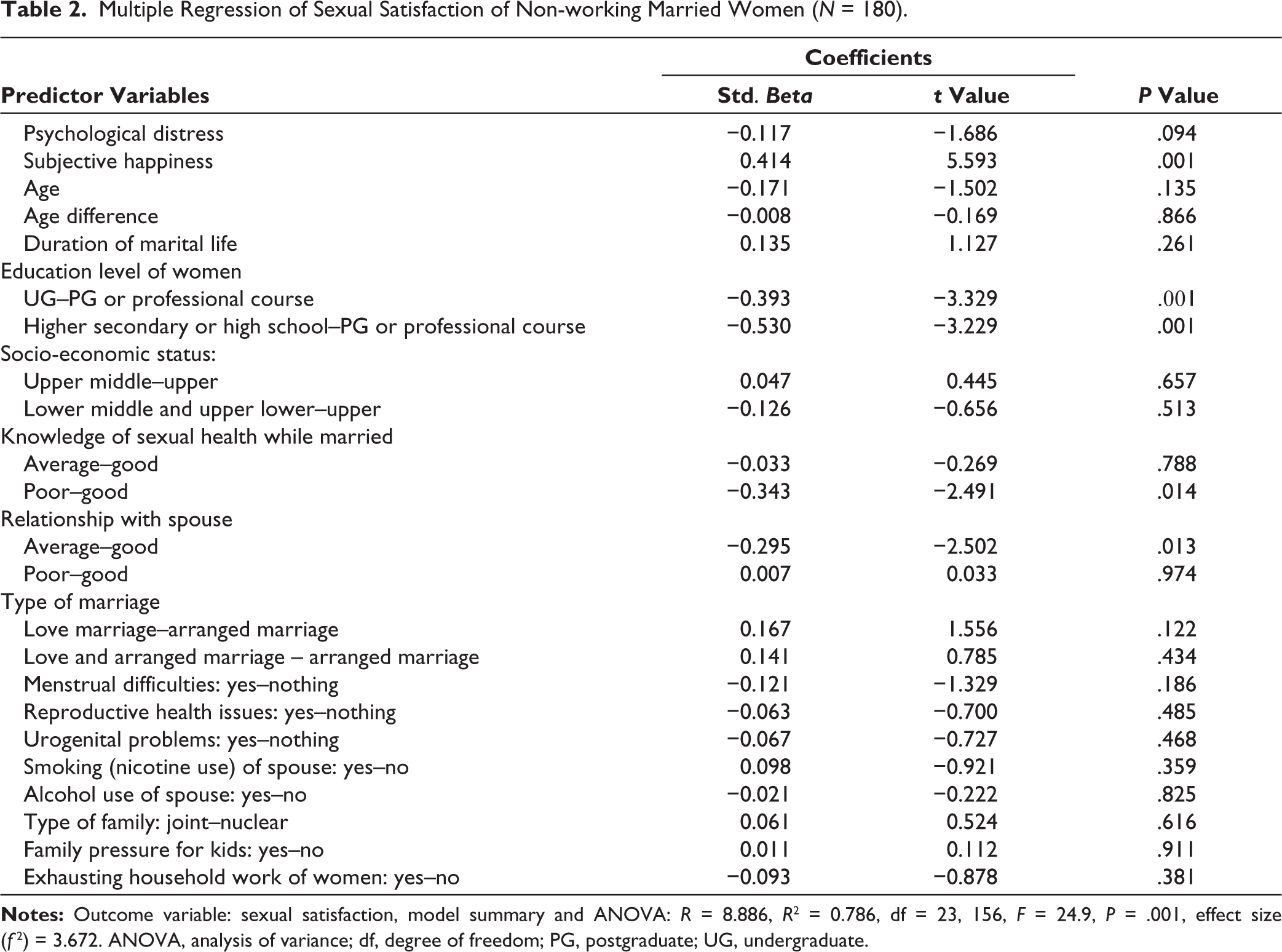
The multiple regression model summary shows that psychological distress, subjective happiness, menstrual health difficulties, reproductive health issues, urogenital problems, type of family, family pressure for children, type of marriage, exhausting household work, the smoking (nicotine use) of the spouse, alcohol use of the spouse, knowledge of sexual health while married, relationship with spouse, education level of women, socio-economic status of women, age, age difference between couples and duration of marital life together predict the sexual satisfaction of non-working married women, F (23, 156) = 24.9, P = .001, and the model is significant. Accordingly, all predictor variables together contribute 78.6% of the variance in Sexual Satisfaction (R2 = 0.786) with a large effect size (f 2 = 3.672). Subjective happiness (P = .001), higher education levels (P = .001), knowledge of sexual health at the time of marriage (P = .014), and a strong spousal relationship (P = .013) were the only significant positive predictors in the regression model individually when the other variables were kept constant, as indicated by the P values along with standardised Beta coefficients and t values in the regression model.
Discussion
This study found that the regression model of sexual satisfaction among non-working married women with 18 predictor variables is significant and contributes 78.6% of the variance. However, not all predictor variables make a significant individual contribution to the regression model, except for subjective happiness, education level of women, knowledge of sexual health while married and relationship with spouse. The study found that psychological distress is a negative predictor and subjective happiness is a positive psychological factor that predicts sexual satisfaction. Although there is no specific published evidence on non-working women exploring the predictors of sexual satisfaction, a few studies on women, including both working and non-working categories, have explored similar findings. Psychological well-being is a well-established predictor of sexual satisfaction in midlife women. 26 One of the previous reviews found that happiness is a positive factor, while stress, anxiety and depression are found to be negative factors. 17
In this study, menstrual health difficulties, reproductive health issues and urogenital problems are identified as negative predictors of sexual satisfaction among women. Previous studies have revealed that factors such as urinary incontinence, genital tract surgeries and infertility negatively affect sexual satisfaction among women; however, these studies were not specifically focused on non-working women.17,27–30 Additionally, menopausal symptoms have also been found to impact sexual satisfaction, as reported by one of the previous studies. 26 Family factors such as type of family (nuclear or joint family), family pressure for children, type of marriage (arranged or love marriage) and exhausting household work are identified as the predictors of sexual satisfaction in women. The analysis revealed that women in nuclear families and love marriages reported higher sexual satisfaction, while women with family pressure for children and exhausting household work reported lower sexual satisfaction. A review of factors affecting sexual satisfaction in women observed that the number of children and family responsibilities influence sexual satisfaction. 17
The spouse’s characteristics, such as smoking and alcohol use, and poor knowledge of sexual health at the time of marriage, are identified as unfavourable factors, while a good relationship with the spouse is found to be a favourable factor for sexual satisfaction among women. The existing literature has observed similar findings, such as a lack of previous information about sexuality decreasing sexual satisfaction in women. 9 Some studies have also observed that factors related to a couple’s relationship like marital satisfaction, frequency of sex, relationship adjustment and mutual pleasure are the predictors of sexual satisfaction in women.3,26,31 A systematic review found that relationship satisfaction is the most positive predictor of sexual satisfaction in women in general across the studies considered. 8 Additionally, a longitudinal study pointed out that relationship satisfaction is a significant predictor of sexual satisfaction in mixed-sex couples, averaging 34 years old and with an average relationship duration of 9 years. 13 However, these studies are not from the Indian context. It is evident from the literature that relationship satisfaction is a key determinant of sexual satisfaction among both heterosexual men and women.31,32
The higher education level is observed as an important predictor of sexual satisfaction in women in this study, but another study found that the level of education is not significantly related to sexual satisfaction among women. 33 Nevertheless, another study found that women with a higher education level have more sexual satisfaction than those who have less education, but this difference was not statistically significant. 34 In this study, demographic factors such as age, the age difference between couples, and the duration of marital life are found to be significant predictors of sexual satisfaction in women. However, evidence in the literature shows that age has a significant association with sexual satisfaction in married women. 34 Conversely, another study observed that age is not a significant predictor of sexual satisfaction. 11 The systematic review on predictors of sexual satisfaction among women observed that both age and relationship duration have a controversial effect on the sexual satisfaction of women, as some studies identified both as having a positive impact, while a few other studies found both to have a negative impact. 8 In another study, a shorter duration of marriage and a smaller age difference between couples tended to be associated with higher sexual satisfaction in women, but this association was not statistically significant. 34 All these indicate that the socio-demographic factors such as the education level of women, age, the age difference between couples and duration of marital life have a controversial effect on the sexual satisfaction of women.
The results indicate the need for preventive and promotive sexual health practices while working with women. The implications of the current study findings are as follows:
As the results suggest, sexual satisfaction of women is affected by menstrual and reproductive health difficulties. It is well understood that these issues are often associated with lifestyle changes and taboos prevalent in the community. Hence, there is scope for sexual health practitioners to work at different levels, such as micro, mezzo and macro. For example, identifying girls at risk for menstrual health issues in schools and colleges and providing them with the necessary education to improve their sexual health and hygienic practices.
It is important to promote existing sex education at the school level. School teachers need to be sensitised, and an appropriate curriculum on sexual health and healthy lifestyles should be adopted.
It is crucial to address stigmatised attitudes in the community through awareness campaigns and health education programs in India.
Sexuality is a very sensitive and often less discussed topic in India. Hence, most of the issues related to sexual satisfaction are not discussed. Even among couples, this is a major barrier to effective communication. This could be addressed through premarital and marital counselling.
Sexual health practitioners need to be sensitive enough to address these issues and should be specifically trained in premarital, marital, couples counselling and sex therapy. These approaches can address sexual satisfaction among couples and also reduce the distress that may be interrelated with sexual satisfaction. However, there is a major challenge in training health practitioners, such as the lack of importance on sexual health issues and interventions in the curriculum. Additionally, there is poor training and supervision on these issues for health and allied healthcare professionals.
There is a lack of importance given to research on sexual health issues and interventions. Additionally, sexual health knowledge is scarce concerning various physical, psychological, social and family aspects. Hence, there is a need for health researchers to conduct research in this area to advance their knowledge.
The strength of this study was its methodological rigour in each phase, especially in tool development, data collection, data analysis and reporting, which ensured trustworthiness and transparency. Additionally, a thorough review of existing literature and prior qualitative studies enabled the identification of various predictors of the model without any biases. 18 Although the study focused only on Bengaluru, the samples were included from varied socio-cultural backgrounds to ensure the representative samples of the population of non-working married women in Bengaluru.
The major limitation of the study was the COVID-19 pandemic, as it influenced data collection immediately after the lifting of the lockdown in terms of the availability of samples, the feasibility of conducting in-person interviews, time requirements and the fear of spreading COVID among the population. As the samples were only from the non-working group, the interpretations are limited to the obtained data, and the results cannot be generalised to both working and non-working groups of women. Additionally, both quota and snowball sampling may introduce selection biases and limit representativeness, affecting the generalisability of the findings. Quota sampling was employed to identify samples from various categories based on their socio-demographic profiles, while snowball sampling facilitated the identification of additional samples by leveraging those initially identified through quota sampling. Being a very sensitive and personal topic, language may have been a barrier to data collection. If the data could have been collected in their mother tongue, richer data might have been shared by the participants.
Conclusion
In conclusion, sexual satisfaction in non-working married women is influenced by physical, psychological, familial, social, demographic and couple-related factors. It is also found that these factors influence sexual satisfaction either positively or negatively. As the sexuality of women is a very complex phenomenon, the influence of such factors varies from person to person over their life period, which implies the need for developing a support system for married women to address their sexual health concerns. It is also necessary to explore the influence of the working status of women on their sexual satisfaction by conducting further studies with both working and non-working women. More studies are required to find out the causal relationship between these predictors and the sexual satisfaction of women, with larger samples and a focus on preventive and promotive frameworks to address these issues.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Authors’ Contribution
The first and second authors contributed significantly to the study’s conception and the preparation of the study protocol. The first author collected and processed the data. Both the first and second authors participated in the quantitative data analysis. The third author contributed substantially to the quantitative analysis and its reporting by providing expert guidance and continuous suggestions for improvement. The first author prepared the first draft of the manuscript. All three authors have read the, revised and approved the final version of the manuscript. All three authors declare that there is no conflict of interest.
Data Availability Statement
Anonymised data will be available upon request from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
No generative AI tools were used for this manuscript to collect or gather data, produce images or graphs or write the manuscript. Authors assume full responsibility for the entire content of the manuscript.
Ethical Approval
The study was conducted in accordance with the principles of the Declaration of Helsinki (1964) and its latest amendments. The study proposal and related documents were approved by the Institutional Review Board of CHRIST (Deemed to be University), Bengaluru, India (Date: 19/07/2019; Ethical Approval No.: CU: RCEC/00075/7/19). The study has been registered with the Clinical Trials Registry, India (Trial Registration Number: CTRI/2020/06/025503).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The written informed consent was taken from all the study participants for participation in the study and publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.