
Abstract
Background:
Sexual dysfunction and marital intimacy and quality are found to have a reciprocal relationship. Examining this relationship in couples seeking help for sexual dysfunctions in the cultural context of India is worthwhile.
Aim:
This study aims to explore the nature of sexual functioning, sexual interaction, sexual communication, and marital intimacy and quality in couples with sexual dysfunction. Further, relationship between the above variables is also examined.
Methods:
A cross-sectional, single-group exploratory design was adopted. A sample of 155 married heterosexual individuals, with a clinical diagnosis of sexual dysfunction in either of the spouses, was included in the study. The tools used included MINI neuropsychiatric interview, Marital Quality Scale, Marital Intimacy Questionnaire, Dyadic Sexual Communication Scale, and Sexual Interaction Inventory.
Results:
Erectile dysfunction and premature ejaculation in men and hypoactive sexual desire disorder in women were the most common sexual dysfunctions. Majority of the sample were young adults. About 82% of the sample had moderate-to-severe levels of marital distress. Mood disorder was the most common psychiatric disorder reported in the sample. High levels of intimacy problems were seen with no significant gender differences in the overall marital quality or intimacy. Difficulty in the overall sexual interactions was found; however, higher levels of dissatisfaction with the frequency of sex and lower self-acceptance was reported by men compared to women. Significant interrelationships were found between marital quality and intimacy, sexual interaction, and sexual communication.
Conclusions:
Sexual dysfunctions and marital distress are closely related. Sexual interaction and sexual communication play a significant role in marital quality and intimacy.
Keywords
Introduction
Sexual dysfunctions are highly prevalent, affecting both men and women; however, research has focused largely on men compared to women. 1 The level of education seems to influence the reporting of sexual dysfunction. In an epidemiological study from Southern rural India it was reported that the prevalence of sexual dysfunction decreased with an increased level of education in men and increased with an increased level of education in women. 2 The literature on heterosexual couple indicates that women most frequently experience desire and arousal dysfunctions, whereas men experience premature ejaculation and erectile dysfunction.3–4
Sexual dysfunctions affect the interpersonal functioning and overall quality of life significantly in both men and women. 5 Marital quality is largely dependent on the satisfaction in the sexual relationship of the couple.6–8 Alternatively, marital distress is associated with lower sexual satisfaction and increased chances of sexual dysfunction. 9
Strong correlation has been found between satisfaction in marriage and sexual satisfaction and this association is further found to help couples in consolidation and preservation of stability in relationship. 10 A satisfying sexual relationship is characterized by absence of sexual dysfunction, satisfaction with the quality and frequency of sex, feelings of love, 11 marital happiness, 12 and lower levels of marital conflict. 13 However, research has demonstrated that the association between sexuality and marital satisfaction is not universal, meaning that marital satisfaction can exist in the absence of sexual satisfaction and vice versa. 14
Sexual functioning is considered an integral facet of intimacy. 15 Ferreira et al 16 found that intimate emotional connection and self-integrity are crucial for sexual desire within marriage or in long-term relationships. Lower levels of intimacy, satisfaction, and quality of intimacy have been observed in individuals with hypoactive sexual desire disorder (HSDD), than in controls. 17 Women are reported to engage in sexual relationships because they provide emotional intimacy and increased well-being which are rewarding for them.18, 19
The quality of communication between spouses has been identified as an important factor in relational satisfaction. Sexual self-disclosure and openness between the partners on their sexual preferences are identified as a few key aspects of sexual satisfaction. 20
In clinical research, determination of whether or not the sexual dysfunction is accompanied by marital distress is relevant since both may influence the mental health of the individuals. The role of gender in the association between marital distress and sexual dysfunction is an unexplored-area. Though there are indications for close associations between intimacy and sexual functioning, in view of variations with gender and culture, it is worthwhile to understand the nature of their association in the Indian context. In addition, the role of sexual communication in marital and sexual satisfaction would help in addressing both sexual dysfunctions and marital distress in therapy with couples. Thus, the study aims to explore the nature of sexual interaction, sexual communication, marital intimacy, and marital quality in couples with sexual dysfunction. Additionally, the relationship between the above variables is also examined.
Methods
A cross-sectional, single-group exploratory study design was adopted. The participants were recruited from 3 setups of a Metropolitan city in India: (a) the outpatient and inpatient clinical services of a tertiary psychiatric hospital, (b) clinical services of psychiatrists/clinical psychologists in private practice, (c) psychiatry, gynecology, urology, and dermatology outpatient departments of general hospitals.
Sample size was estimated using mean and variance of marital quality scale through paired “t” test, 95% confidence limit was used for the purpose of the current study. Sample size was estimated at 112, a margin of error of ±4. The total sample included in the study was 155 married individuals.
Married persons (socially/legally) with a clinical diagnosis of sexual dysfunction in either of the spouses, women who are 18 and above, and men who are 21 years and above (as per legal marriageable age in India), those in the first 4 family lifecycle stages namely married couple without children, child bearing families, families with preschool children, and families with school-going children and those with working knowledge in English/Kannada/Tamil/Telugu were included in the study. Those with clinical diagnosis of substance dependence, psychosis, mental retardation, epilepsy, terminal illness in either spouse; those who were not living with the spouse at the time of the study were not included in the study. The tools were translated into Kannada, Tamil, and Telugu using the standard procedures.
Tools
The scale is a sensitive and accurate measure of sexual dissatisfaction in couples. Internal consistency coefficient ranges from 0.79 to 0.93 and test-retest reliabilities range from 0.53 to 0.90. The inventory is able to discriminate between clients with dysfunction and those without.
Procedure
The study was approved by institute ethics committee. Out of 153 married couple with the diagnosis of sexual dysfunction, those who met the inclusion criteria (119) were approached for recruitment. Of these, 37 could not be recruited for the following reasons: 16 refused consent, 3 missed appointments, 2 got better, 11 could not be contacted, and 5 could not participate due to distance. Among the rest of the 82, 73 were couples (146 individuals) and 9 individuals participated without their spouse. In total, 155 individuals were administered the tools selected for the study.
Assessments were carried out at the family psychiatry center or at the center for well-being. Those who consented were administered the sociodemographic sheet followed by the quantitative measures used in the study, that is, Marital Quality Scale, Marital Intimacy Questionnaire, Dyadic Sexual Communication Scale, and Sexual Interaction Inventory in that order. Each of the spouses were assessed individually by the researcher. Assessment lasted approximately for 90 min with each spouse.
Analysis
Statistical Package for Social Sciences Version 16.0 was used for analysis. Confidence level was set at 95%. Two-tailed tests of significance were used. The scores on quantitative measures were tested for normalcy through Shapiro-Wilk test. Sociodemographic, family/marital, and clinical profile of the sample was analyzed using descriptive statistics such as mean, range, standard deviation, frequencies, and percentage. Age and duration of marriage did not follow normal distribution. Partial correlation was carried out controlling for age, childlessness, use of psychotropic medication, and presence of psychiatric and physical illness to study the relationship between the variables in the study. Nonparametric Spearman’s rho test was used to assess correlation as variables followed non-normal distribution.
Results
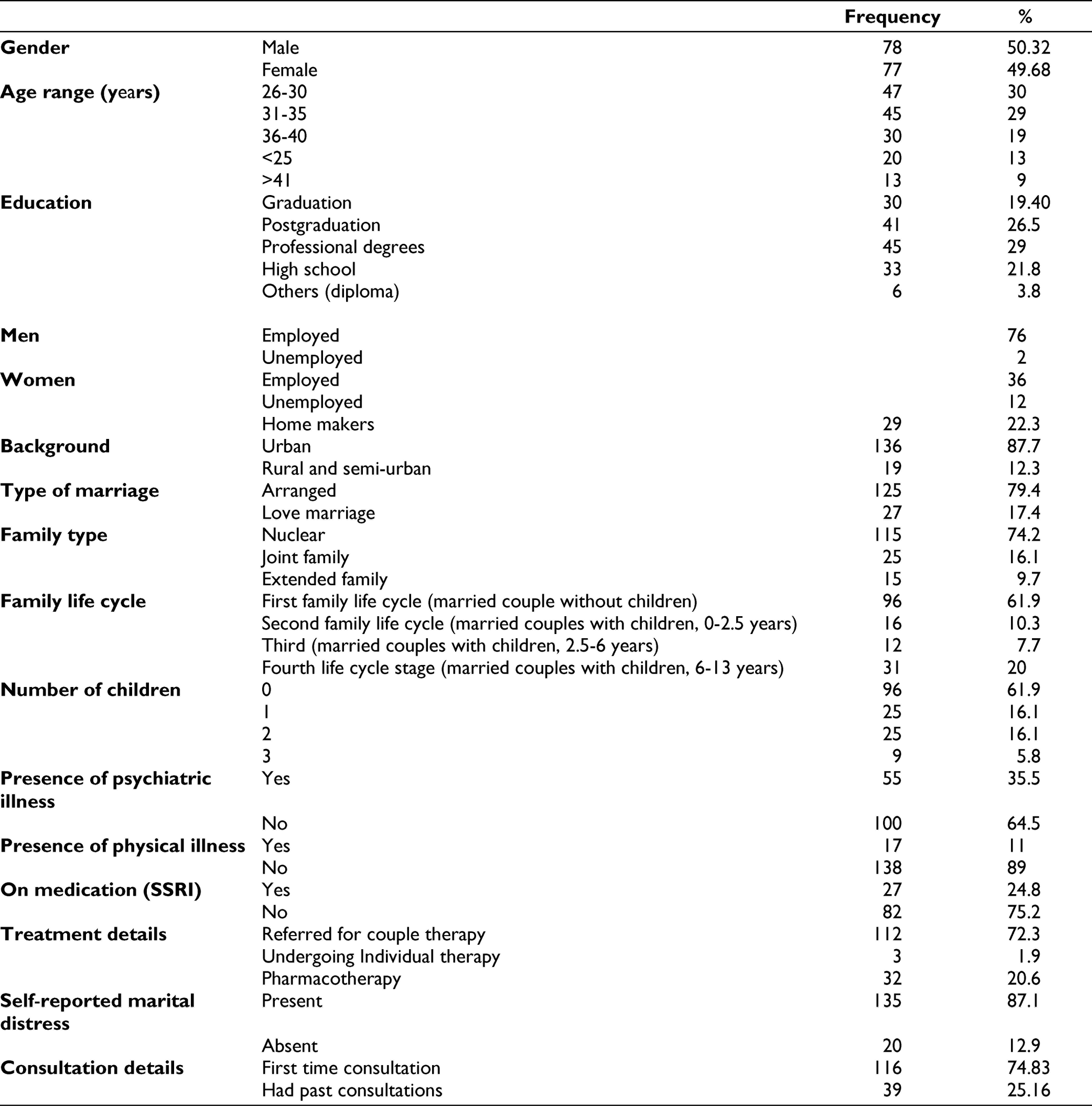
The age of the sample ranged between 18 and 56 years (Table 1). Mean age of the sample was 32.19 years. More than two-thirds of the sample was under 35 years of age and about 28% of the sample was 36 years of age or above. With regard to the occupation of the sample, 72.3% of the sample was employed. Most of the families belonged to middle-income group (80%) whereas 10% belonged to an upper socioeconomic status. Most of them were seeking treatment on an outpatient basis (89.6%) and 10.3% were inpatients. Majority were referred for couple therapy for marital distress to family psychiatry unit. Infertility issues were reported by 14.2% (n = 22).
Sociodemographic and Clinical Details of the Sample (N = 155)
Out of the total sample (n = 155), 75 individuals reported sexual dysfunction and their spouses did not report sexual dysfunction. Table 2 shows that erectile dysfunction is the most common condition in men followed by premature ejaculation. On the other hand, in women HSDD is the most common in this sample, followed by sexual aversion disorder and vaginismus.
Frequency and Percentage of the Sample With Diagnoses of SD (N = 75)

On MINI, about half of the sample did not get any diagnosis (64.5%). The most common condition among the rest of them was major depression, with about 40% of the sample fulfilling criteria for current (13.55%), past (15.48%), or recurrent depressive disorders (9.03%). An additional 5.81% of the sample reported of experiencing suicidality. About 8% of the sample met criteria for various anxiety disorders. Three-fourth of the sample denied experiencing any physical ailment either at present or in the past. The most common condition reported was polycystic ovarian disease (7.10%). About 15% of the sample reported experiencing other physical ailments such as diabetes, hypertension, asthma migraine, hypothyroidism and so on.
The mean total score on MQS is more than 2 SD higher than the norms provided by the author. 25 (Table 3). The subscale scores and their comparison with norms indicate that except for the score on the dominance subscale, all the other subscale scores fall above the normative mean and 1 SD. Total scores ranging between 60 and 180 suggest that the sample comprises of couples experiencing a wide range of marital distress levels. With respect to the severity of marital distress, more than half the sample (58%) experienced severe levels of distress, 24% experienced moderate distress, 12% mild, and 6% no distress. There were no gender differences with respect to MQS total score as well as on subscales.
Scores of the Group on Marital Quality (MQS) and Marital Intimacy (MIQ) (N = 155)
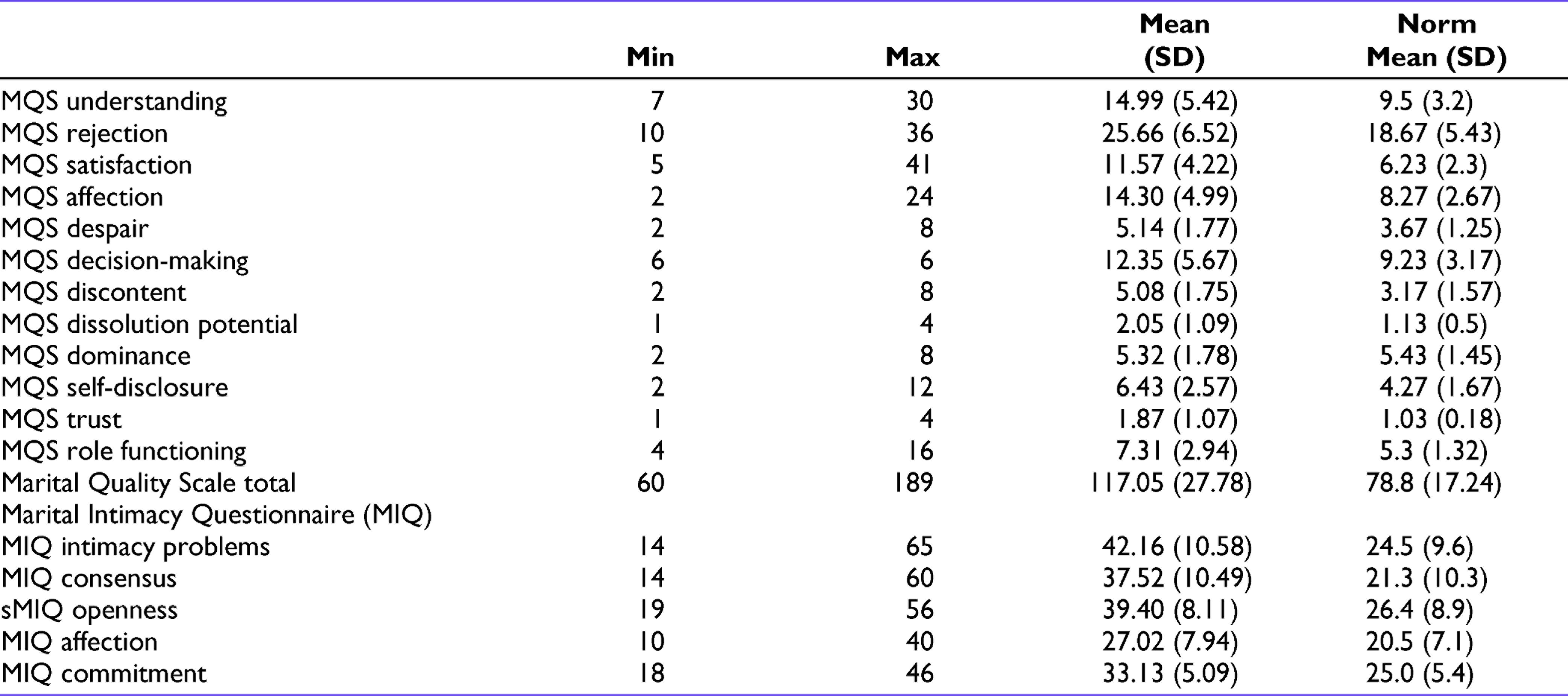
Findings of the sample on MIQ suggest that the current sample has very high scores on the domain of intimacy problems which is about 2 SD above the norms provided for a sample with marital distress. 24 However, scores obtained by the sample on all the other domains are lower than the norms for distressed couple. There were no gender differences on MIQ domains.
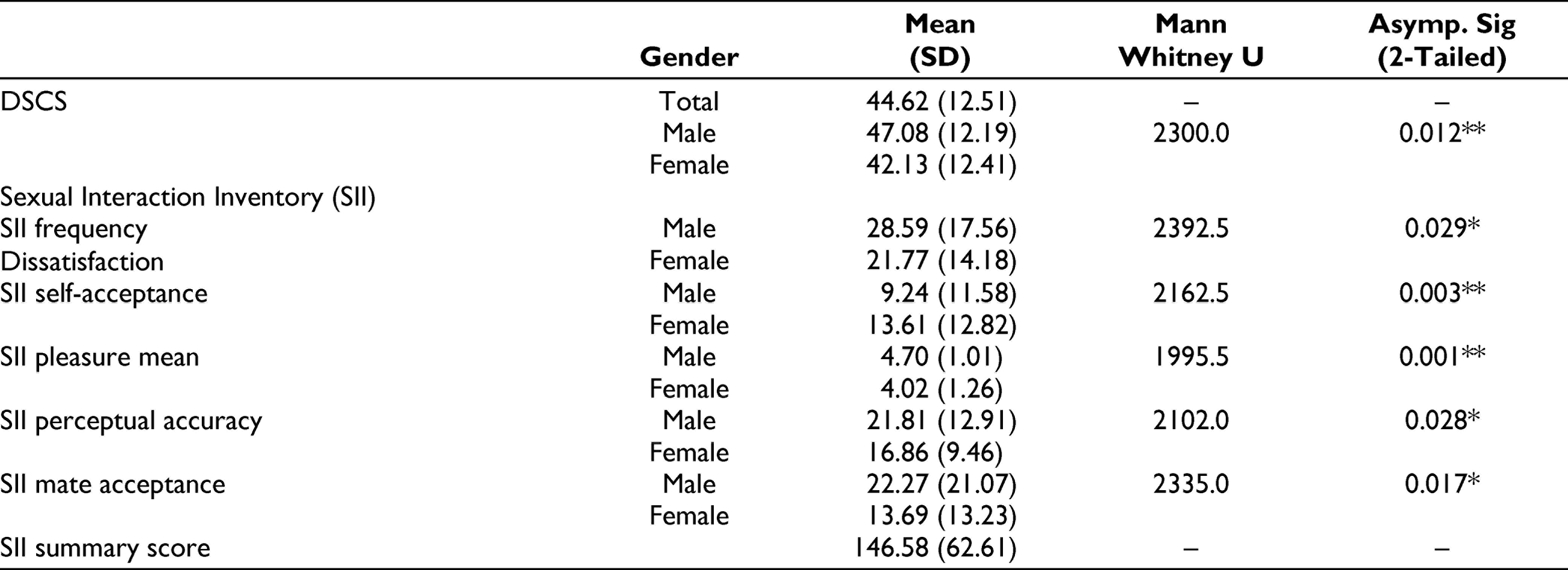
The scores of the sample on the scale DSCS range from 15 to 78 (Table 4). Higher scores on DSCS are indicative of better sexual communication between the spouses. Difference between husbands and wives is significant and suggests that the husbands in the study find the sexual communication in their marriage to be better than what is reported by the wives. Scores on SII and their comparison with the norms provided by the author 22 indicate that the sample in the current study is experiencing very high levels of difficulty in all the domains assessed by the scale. Gender-wise analysis reveals significant difference between the genders on all the subscales of SII. The direction of difference shows that the husbands have higher levels of dissatisfaction with regard to the frequency of sexual interaction and are less accepting of themselves. However, the pleasure experienced, perceptual accuracy of the partner’s pleasure, and mate acceptance is higher in males compared to females.
Scores of the Sample on Dyadic Sexual Communication and Sexual Interaction Inventory (N = 155)
Partial Correlations Between MQS, MIQ, and DSCS-1 (N = 103)
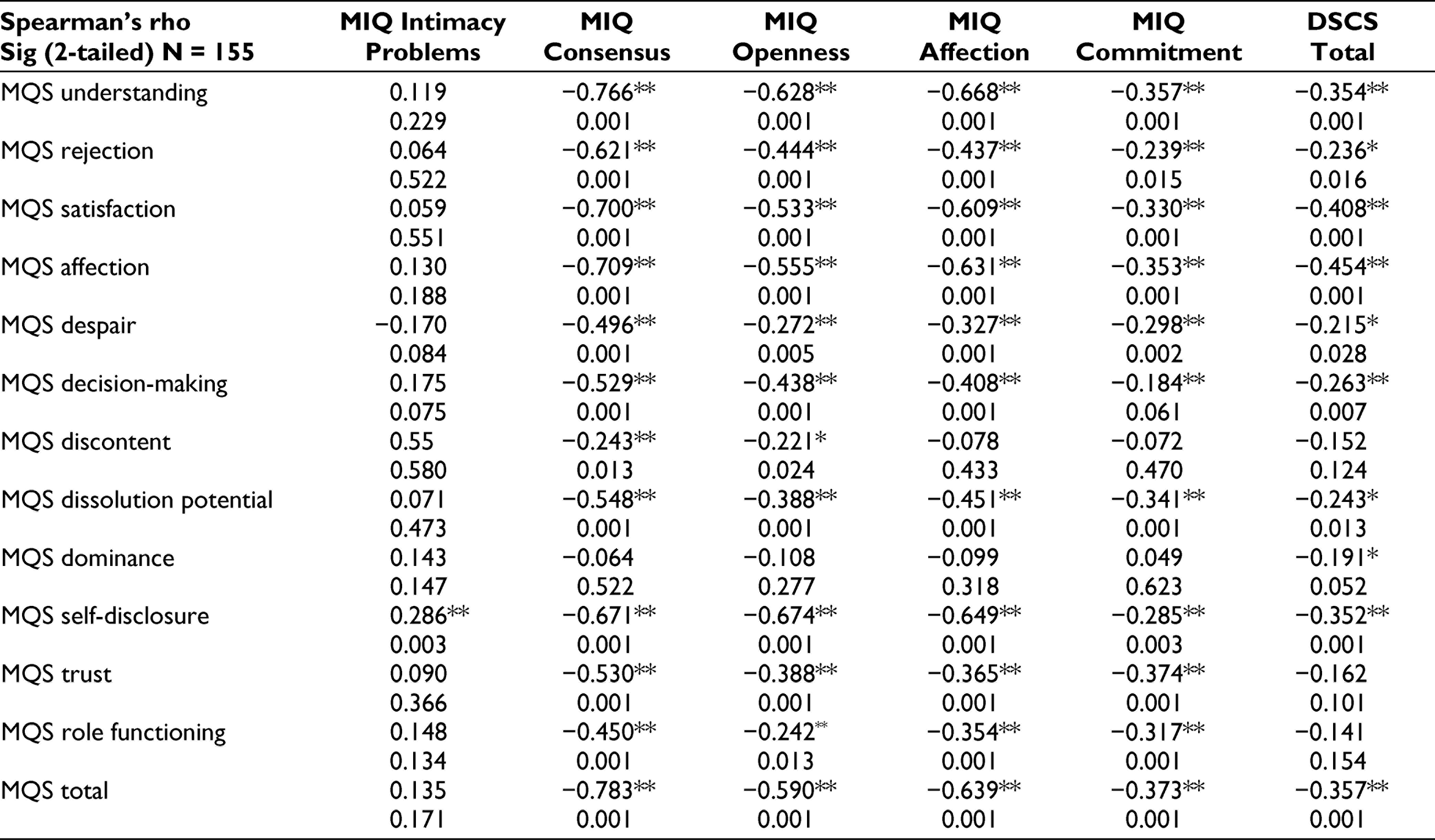
There is significant correlation between the subscales of MQS except subscale dominance with the domains of MIQ. Indicating that distress on MQS is also indicative of distress on the different domains of MIQ. However, intimacy problem subscale was not associated with most of the subscales of MQS except for self-disclosure. The higher problems in marital quality were associated with dyadic sexual communication except for marital discontent, trust, and role functioning.
The correlation between MQS and SII shows that self-acceptance subscale on SII is negative and correlated with rejection (r = −0.290, P = .004) and affection (r = −0.243, P = .02) subscales as well as with total score on MQS (r = −0.234, P = .02). Similarly, MQS trust was associated with pleasure on SII (r = 0.213, P = .04). MQS satisfaction was positively correlated with the mate acceptance (r = 0.335, P = .001), and perceptual accuracy (r = 0.231, P = .02) subscales and the total score on SII (r = 0.205, P = .04).
Correlation between the scales MIQ and SII shows that a higher level of openness is negatively associated with overall score on SII (r = −0.213, P = .03). Perceptual accuracy on SII was negatively associated with DSCS score (r = −0.221, P = .03), and sexual interaction summary score was also negatively associated with DSCS (r = −0.344, P = .001). Indicating that higher the dyadic communication problems, lower will be the perceptual accuracy on sexual interaction. Similarly, higher communication problems are also associated with lower overall sexual interaction.
DSCS total score is positively correlated with consensus (r = 0.495, P = .001), openness (r = 0.587, P = .001), affection (r = 0.501, P = .001), and commitment (r = 0.255, P = .01) subscales and negatively correlated with intimacy problems subscale (r = −0.237, P = .02) of MIQ suggesting that adequate sexual communication is associated with better levels of marital intimacy.
Discussion
Demographic and Clinical Characteristics of the Sample
The study largely comprised of young couples, indicating that sexual dysfunctions probably emerge in the beginning years of the marriage and have significant effect on the marital relationship (Table 1). It is also identified early in the marriage owing to the expectations of the extended family and society in a collectivistic culture like India of the couple to procreate. 26 Most of the sample was educated up to graduation which might not be representative of couples in this age range; however, this perhaps is representative of the couples who seek help from mental health professionals for marital and sexual problems. Also, the sample was recruited from centers in urban Bengaluru and from middle-class background which also might explain the education characteristics of the sample.
In accordance with the trend in India, majority of the couple have had an arranged marriage which indicates the role of family in the marriages. 27 Majority were living in a nuclear family setup, which reflects on changing family structure in India. Family structure and living arrangements is known to influence the quality of marital and sexual relationship.28–30 Majority of the sample belonged to the first lifecycle stage (married with no children). Sexual difficulties might be reported more in the early phases of marriage as there is a threat of marriage dissolving, 31 probably owing to pressure from families to bear the child which is considered as essential part of a marriage to be considered as complete. 27 The percentage seeking help during the second and third life stages for sexual dysfunctions significantly reduce which may be due to their engagement with child rearing and their professional goals, further, a slight increase in the percentage of couples from fourth life cycle stage might reflect that the couple are refocusing on their own sexual issues once the child begins school. Inpatient treatment was sought by a small percentage mainly for their comorbid conditions and some of the outstation couples found it convenient to take therapy being in the hospital. Commonly reported comorbid conditions were anxiety and depression similar to the literature on individuals with sexual dysfunctions.32–33
Most of the sample was recruited from family psychiatry center where couple are referred for the marital distress as well sexual dysfunctions; the couple are recruited upon fulfilling the criteria of sexual dysfunction, which supports the literature that many couple with marital distress also experience SD.32, 34
Sexual Dysfunction, Marital Quality, and Marital Intimacy
In accordance with the previous literature, the most common sexual dysfunction in men was erectile dysfunction and premature ejaculation, and in women it was HSDD in our sample (Table 2).35, 36 Other common conditions diagnosed in women were sexual aversion disorder and vaginismus and a small percentage of men had HSDD. 37
With respect to marital quality, the sample on the whole falls under moderate marital distress category, and more than half the sample were experiencing severe marital distress and about quarter of the sample fall under moderate levels of distress (Table 3). The findings confirm the earlier studies conducted in India.38, 39 High levels of distress in the sample may be because the sample was selected from a mental health institute where couples seek help for relationship issues. Alternative explanation could be that presence of SD might further worsen marital quality compared to those who present with marital distress alone.6–9 This probably explains why a significant proportion of marriages are dissolved primarily owing to troubles in their sex life. 40 Another message from the finding would be that these couples perhaps might not benefit by management for SD alone.
High levels of intimacy problems were reported which is much higher than the norms provided for those with marital distress. This is expected as the sample had moderate marital distress; marital quality and intimacy are found to be positively correlated. 24 However, the domains of consensus, openness, affection, and commitment are similar to that of a martial nondistressed population, indicating perhaps that the profile of intimacy seen in Indian sample is unique wherein couples despite experiencing marital distress continue to be committed to the relationship, maintain affection towards the partner and strive towards consensus and openness in the marriage. Further research is required to explore the factors that might contribute to the same. One seminal study provides a possible explanation for higher marital satisfaction in Indian couples with arranged marriages. The study reported marital satisfaction as less dependent on verbal, nonverbal, and sexual communication. 41 The authors attributed higher satisfaction in these couples to submissiveness of the female partner, better levels of social support in arranged marriages; cultural influences of prioritizing family stability, commitment to the relationship, tendency to go along with each other’s decisions despite the disagreements as probable reason for discrepancy between the western norms and the scores in our Indian sample. With regard to marital intimacy and its association with sexual functioning, difficulties in intimacy is known to result in decline of sexual desire within marriage. 42
Sexual Communication and Interaction
Significant difficulties in sexual communication were noted in the sample compared to the norms for distressed couples provided by the author. 23 The findings are supportive of the earlier research where sexual communication has been found to be poorer in couples with sexual dysfunction compared to normal controls. 43 Sexual self-disclosure and openness between the partners on their sexual preferences are found to be key aspects of sexual satisfaction. Lack of knowledge about one’s sexual preferences and that of partner is found to be associated with persistent sexual dysfunction. 44 In an Indian sample of women with infertility problems, 45 about a quarter of the sample found inadequate sexual stimulation and sexual communication to be an issue in the relationship. Sexual dysfunction in the sample was found to be associated with sexual communication, knowledge about sex, and sexual stimulation.
Wives perceived the sexual communication in the marriage to be poorer than the husbands in our sample. Indicating a higher need for sexual communication in women, research shows that negative behaviors displayed during the discussion of a sexual problem were related to lower levels of relationship satisfaction for wives and not for husbands. 44
The sample on the whole shows significant levels of sexual dissatisfaction on SII in addition to husbands being more dissatisfied with the frequency of the sexual interaction than the wives (Table 4). One of the reasons for discrepancy between desired and actual frequency of sex may be the marital distress or sexual dysfunction reported by the sample; however, the study did not explore the details of the same. Self-acceptance is poor in men with respect to the sexual performance; however, they are better than females with respect to acknowledging the pleasure, mate acceptance, and accuracy of perception of the partners’ pleasure. Poor self-acceptance in men may be partly attributed to the presence of sexual dysfunction in this sample. Sexual performance is known to be associated with satisfaction in life and self confidence especially for men. 46
Association Between the Variables
The distress on MQS and on MIQ is significantly correlated (Table 4). Most subscales of MQS are correlated with MIQ except for dominance subscale, indicating that dominance may not be playing a significant role in the marital distress. Author of MIQ considers intimacy problems domain to be a behavioral domain where in difficulties experienced by the couple at a behavioral level are tapped. In a sample of couples predominated by marital distress, it is presumable that there will be problems in open communication, decision-making, conflict resolution, and role functioning. The association between intimacy problems and self-disclosure is understandable, when the couples do not share an intimate relationship, they may find it hard to share personal feelings, needs, and problems. Marital quality is reported to be associated with self-disclosure in intimate relationships. 47 Communication is the means through which couple could attain congruence between sexual desire of each partner and the sexual interaction. One study found that couples with an anorgasmic female partner had more problems in communication about sexual issues compared to controls. 48 Sexuality being a very sensitive topic of conversation, couples with marital distress perhaps might have difficulty expressing their dissatisfactions or their needs. In this study, significant association is found between sexual communication and marital quality. Association between sexual communication and marital quality has been recorded in couples with self-reported dyspareunia in female partners. 43 Marital quality has been found to predict sexual initiation, sexual activity, and sexual satisfaction in couples.41, 49 One of the interesting findings in our study is that sexual communication was not associated with marital discontent, trust, and role functioning. The finding might indicate that the couple go on to fulfil the roles within the relationship even when the sexual functioning is not adequate. It is probable that other factors such as personality, social, and emotional attachment are playing a role in marital satisfaction.14, 50
In the current study, overall marital quality and overall sexual satisfaction are not associated. This finding is not in accordance with earlier studies where marital satisfaction and sexual satisfaction have been found to be associated.39, 49 However, higher marital distress, rejection, and lack of affection is associated with lower self-acceptance, which means that feeling rejected by the partner and lack of affection results in higher marital distress. Higher satisfaction in the marital quality is associated with mate acceptance, perceptual accuracy, affection, and overall sexual satisfaction, which indicates that the satisfaction in the marital relationship is derived largely from the acceptance by the other partner. The finding is supported by another study which reported direct effect of the intimate partner acceptance on marital and psychological adjustment in couple. 51
Significant positive associations were found between Subscales on MIQ and overall score on DSCS suggesting that higher levels of marital intimacy and better sexual communication go together.
Examining the relationship between marital intimacy and sexual satisfaction shows that consensus, openness, and affection domains of MIQ are associated with better mate acceptance, better overall sexual satisfaction, and increased pleasure levels on SII, respectively. This could mean that higher levels of openness and the ability of the couple to come to an agreement with each other (probably through better communication and negotiation skills) lead to increased levels of acceptance of each other as a sexual being and increased levels of sexual satisfaction.20, 52 Low levels of affection, consensus, and openness between the couple could also be a consequence of sexual dysfunction in either of the spouses. However, this line of reasoning requires further investigations to obtain conclusive findings. Regression analysis could not be conducted in the current study owing to lack of strong correlations between the variables.
Some of the important strengths of the study are that the focus is on the relationship facilitating insight on the relationship ramifications of SD. Sexual dysfunctions in general, including male and female dysfunctions, are examined rather than limiting to a specific dysfunction. The sample size was adequate and included both the partners thus we could draw inferences about how sexual dysfunction affects marital relationships in India.
However, certain limitations of the present study include lack of objective assessment of sexual dysfunction across the sample, possibility of self-selection bias as couples could not be directly approached by the researcher in the medical clinics, the study could not understand the profile of patients who did not consent to be screened for inclusion criteria and lack of qualitative interviews due to space and time constraints. The role of past or current physical or psychiatric illnesses and drug treatments was not evaluated in causing and maintaining sexual dysfunctions, which can have implication in the treatment.
The important implications of the study are: the findings enhance the theoretical understanding of the interrelationship between sexual interaction of married couple and the marital relationship in general. Community research examining the interrelationship between the couple relationship and sexual relationship in a normal sample would throw light on the evolution of this interrelationship in order to develop a theoretical psychopathology model for the purposes of preventive work at the grass root level. The study also highlights the importance of assessing awareness of men and women about sexual functioning and satisfaction which might play a part in shaping communication, pleasure, and understanding the needs of the partner.
Conclusion
Couple with sexual dysfunctions experience marital distress and lack of marital intimacy. Sexual interaction and dyadic sexual communication plays an important role in the marital quality and intimacy. Thus, it is important to address the interaction and intimacy components in the intervention for couple with sexual dysfunctions while giving due importance to gender-related needs in sexual and marital intimacy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.