
Abstract
Background:
Sexual dysfunction, a potential side effect of selective serotonin reuptake inhibitors (SSRIs), can lead to marital dissatisfaction in remitted depression patients, affecting their quality of life (QOL), and all of these are risk factors for treatment noncompliance. We aimed to estimate the proportion of female sexual dysfunction and its subtypes compared to the general population and correlate it with various factors, including marital satisfaction and QOL, in remitted depressive patients on SSRI treatment.
Methods:
This analytical cross-sectional study assessed 116 women, comprising 58 patients aged 18– to 45 years with rsemitted depression on SSRI monotherapy for a minimum of six weeks and their age-matched comparative group. Hamilton Depression Rating Scale was used to assess depression severity and Female Sexual Functional Index, to assess sexual dysfunction. Couple Satisfaction Index and WHOQOL-BREF version were used to assess marital satisfaction and QOL, respectively.
Results:
In total, 56.89% of the patients had sexual dysfunction, compared to 39.65% in the general population. Exploratory analyses revealed that overall sexual functioning had a significant positive correlation with education (P = .002), marital satisfaction (P < .001), and QOL (P < .01), and a significant negative correlation with the age of onset of depression (P = .004), total marital duration (P = .02), and duration of current treatment (P = .02).
Conclusion:
Sexual dysfunction is common in remitted female depression patients on SSRI treatment, which may further impair their marital satisfaction and QOL. Hence, routine screening for sexual dysfunction is necessary for them.
More than half of the remitted female patients of depression on SSRIs experience sexual dysfunction. Overall sexual functioning had a significant positive correlation with marital satisfaction and QOL.Key Messages:
Healthy sexual functioning is important to an individual’s physical and emotional health. Any problem in normal sexual functioning can affect emotional and overall well-being. Female sexual dysfunction is a disorder of sexual desire, arousal, orgasm, or sexual pain resulting in significant personal distress. 1 Globally, the prevalence of female sexual dysfunction ranges from 38% to 63% because of varied causes, predominantly medical, surgical, iatrogenic, and psychological.2–4 Among individuals with depression, it can be a symptom of the illness per se or an adverse effect of antidepressants. Sexual dysfunction is a potential side effect of antidepressants seen in 30% to 65% of individuals5, 6 and is more common with selective serotonin reuptake inhibitors (SSRIs), with a range of 25% to 70%.1, 7–9 SSRIs downregulate and desensitize 5HT1A receptors involved in regulating sexual motivation and, through activation of 5HT2A and 5HT2C receptors, indirectly alter other neurotransmitters associated with sexual functioning.10, 11 Patients on SSRIs have reduced libido, inadequate lubrication, anorgasmia, and poor arousal.9, 12
Marital satisfaction is important in women because women desire emotional closeness before sexual intimacy can occur. 13 In them, sexual dysfunction is associated with psychological and social consequences, such as marital conflicts, feelings of guilt, anxiety, and socio-occupational dysfunction, leading to poor quality of life (QOL).14, 15 Poor marital satisfaction and QOL are risk factors for depression; so, in females with depression under remission, they can increase the chance of poor compliance to medications 13 and, thereby, the risk of relapse. 5
Global studies on SSRI-emergent sexual dysfunction have found a prevalence range of 25% to 70%1, 7,8 and noted more sexual dysfunction in depressive patients on SSRIs than in the general population, whereas Indian studies have shown a prevalence of around 45%.9, 16 However, they did not correlate SSRI-induced sexual dysfunction with marital satisfaction or QOL. Hence, we aimed to estimate the proportion of female sexual dysfunction and its subtypes in comparison to normal controls, study the various factors associated with it, and determine its correlation with marital satisfaction and QOL in remitted depressive patients on SSRI treatment.
Materials and Methods
This cross-sectional, comparative, and nonblind study was conducted in the Department of Psychiatry in a tertiary health care center in south India for six months (from August 2018 to January 2019). It was approved by the Institutional Human Ethical Committee. A total sample size of 116 subjects, i.e., 58 patients and 58 normal controls as a comparison group, were recruited using convenient sampling.
Subjects
Females aged 21 to 45 years, with a minimum of 1 year of marital life, who could read or understand English, were willing to give written informed consent were recruited. Those with a diagnosis of depressive disorder (F32) or recurrent depressive disorder (F33) according to International Classification of Diseases (ICD-10) and under remission for at least one month, 17 on SSRI monotherapy for at least six weeks, were recruited into the patient group. Age- and sex-matched individuals who were attenders of patients visiting general medical and surgical specialties were taken up for the comparison group. Subjects with any other psychiatric illness or mental retardation; those with a history suggestive of diabetes mellitus, endometriosis, or pelvic inflammatory disease; and those on medications like diuretics, beta-blockers, statins, or other psychotropic medications that are known to alter sexual functioning were excluded from both the groups. Those who had sexual dysfunction before the onset of depression or as a symptom of depressive disorder and those who are single, divorced, or separated were also excluded.
Assessment
ICD DCR 10th edition manual was used to diagnose the depressive disorder in the patients. 17
Schedule for Clinical Assessment in Neuropsychiatry (SCAN): SCAN was developed through a collaboration between the WHO and the National Institute of Mental Health. Its advantage is that it can be used to compare psychiatric diagnoses made across the world. 18 . It was used to rule out other psychiatric illnesses in both groups.
Hamilton Depression Rating Scale (HAM-D): HAM-D is a 17-item questionnaire, with total scores of 0 to 50, to assess the symptoms of depression. 19 Based on the score on HAM-D, depression is graded into mild (8–13), moderate (14–18), severe (19–23), and very severe (>24). Subjects with a score <7 (in remission or normal) were taken into the study.
Female Sexual Functioning Index (FSFI): It is a self-reported questionnaire with 19 questions grouped under six subdomains. The cutoff scores of each subdomain are as follows: sexual desire (<4.28), arousal (<5.08), lubrication (<5.45), orgasm (<5.05), satisfaction (<5.04), and pain (<5.51). The overall score ranges 2 to 36. All those with an overall score <26.55 on FSFI were considered to have sexual dysfunction.20, 21 It was used in both groups to quantify sexual functioning.
Couple Satisfaction Index (CSI-16): CSI-16, a 16-item questionnaire with a cutoff score of 51.5, was used to assess marital satisfaction. Those with a score <51.5 are said to have notable relationship dissatisfaction. 22
WHOQOL-BREF Scale: It is the brief version of the original WHO-QOL 100-item scale. It contains 26 questions to assess the QOL in four subdomains (physical health, physiological health, social relationship, and environment). 23 Scoring is based on the respective transformed scores for the given raw score in each subdomain.
Study Procedure
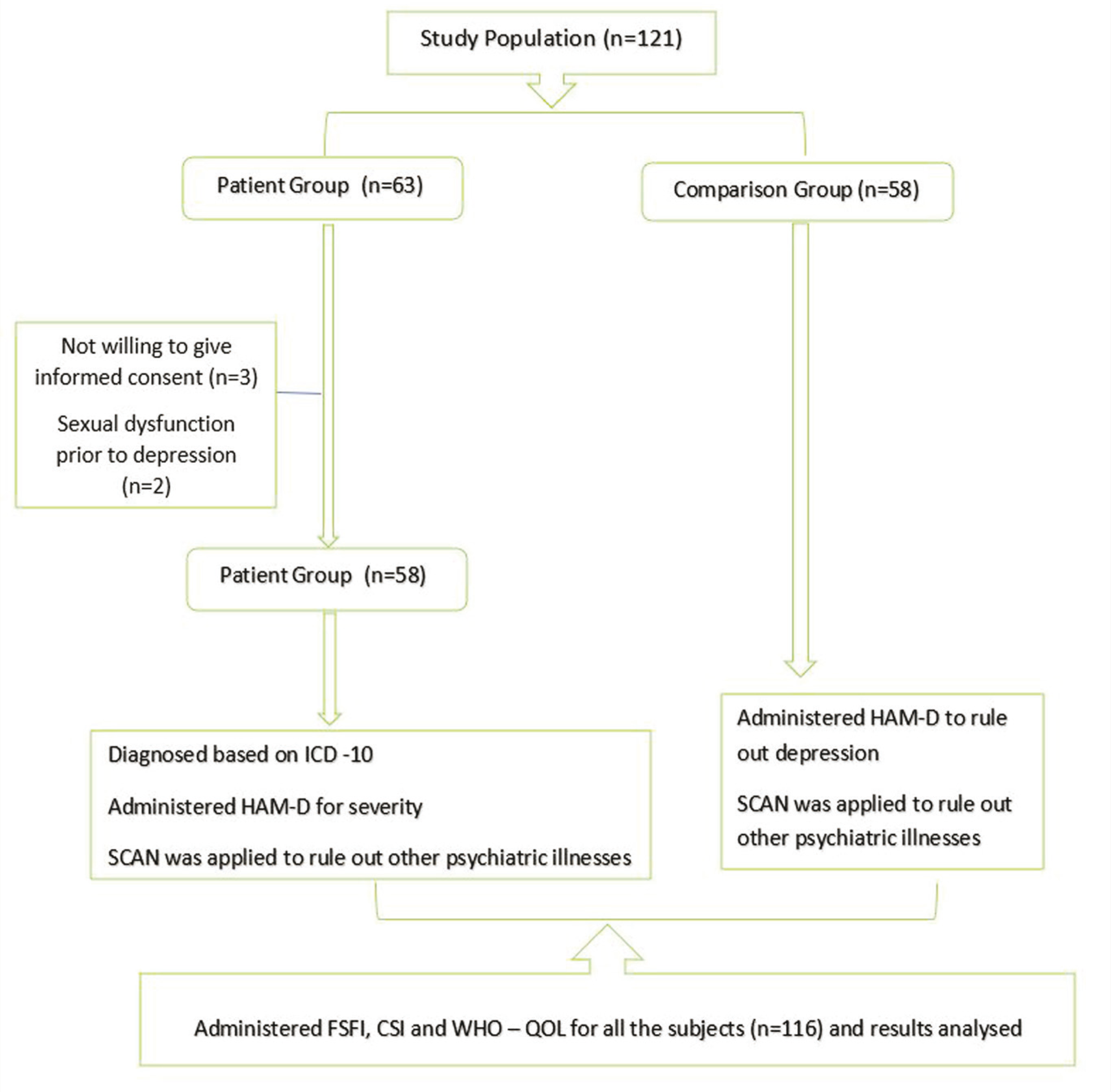
All participants were interviewed and rapport was established. They were ensured adequate privacy during the interview and confidentiality regarding the data to be collected. The study was conducted as per the procedure explained in Figure 1.
Overview of Study Procedure
Statistical Analysis
Collected data were subjected to descriptive statistics using frequencies, and percentages of different variables were calculated. Parametric statistics such as Student’s t-test and nonparametric statistics such as the Chi-square test were used to compare the two groups. In each group, the correlation between various parameters was obtained using Pearson’s correlation or point biserial correlation (r-value). A P value of <.05 was considered statistically significant. Statistical Package for the Social Sciences (SPSS v.22) (IBM Corp., Armonk, NY, USA) software was applied to analyze the data.
Results
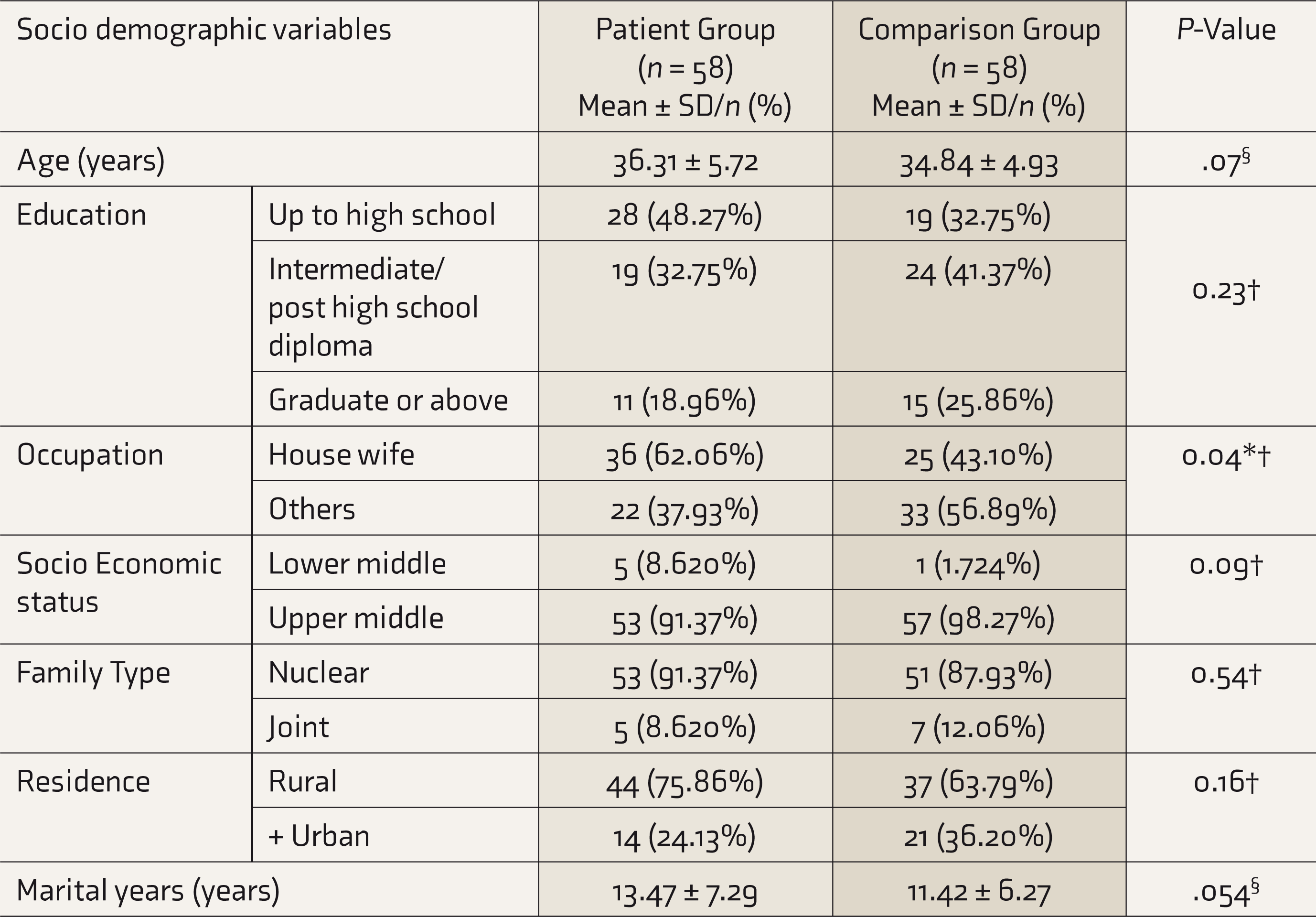
The mean ± SD age of the patient group (n = 58) was 36.88 ± 6.09 years. The majority of them were from a rural background (75.86%), middle to upper socioeconomic status (91.37%), and nuclear families (91.37%), including below undergraduate education (80.21%) and housewives (62.06%). The mean duration of marriage was 13.47 ± 7.29 years, and 17.24% of them had a family history of depression. There was no significant difference in age or other sociodemographic details (except occupation) between the patient and the comparison groups (Table 1).
Comparison of Sociodemographic Details Between Patient Group and Comparison Group (N = 116)
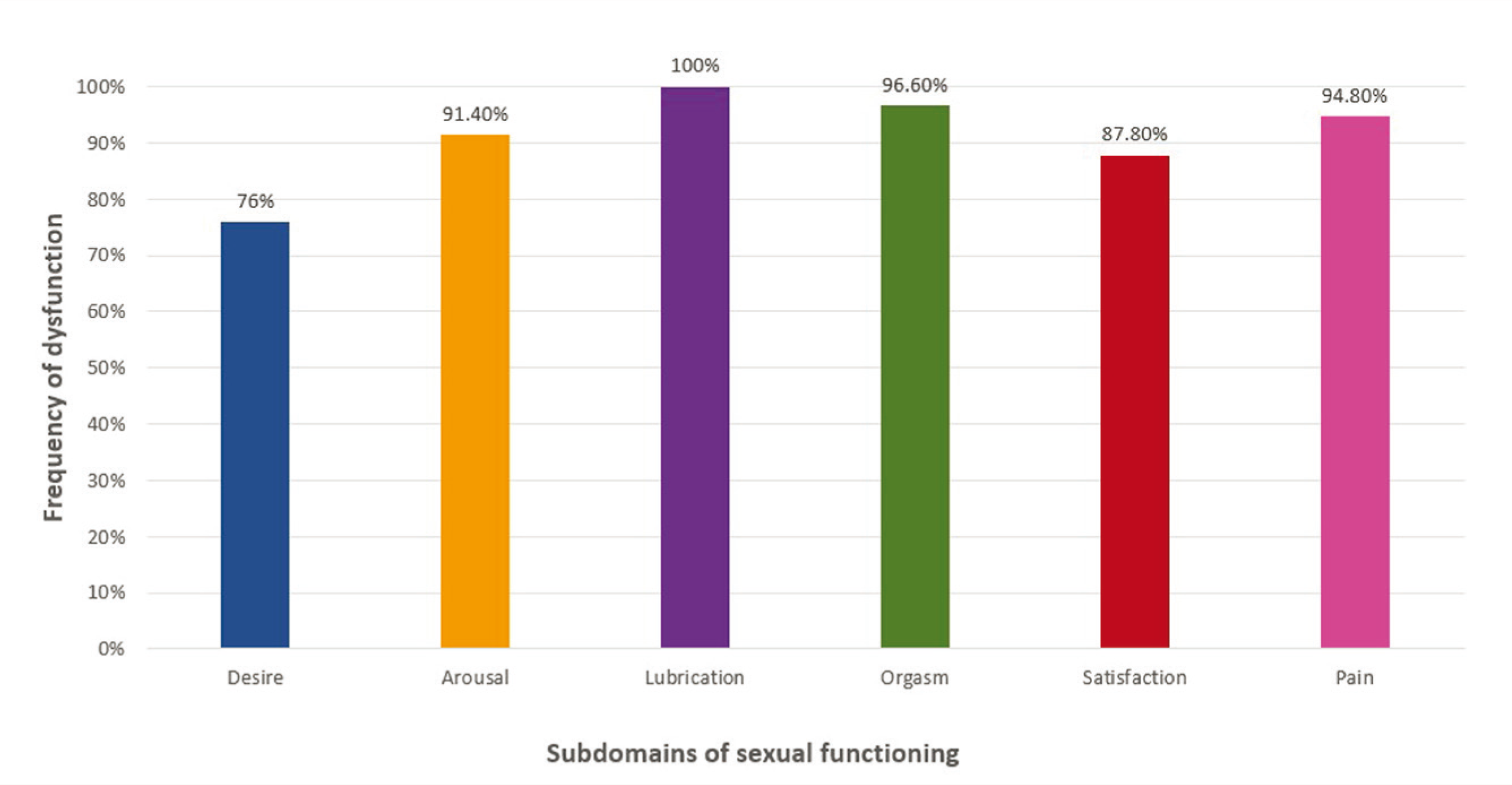
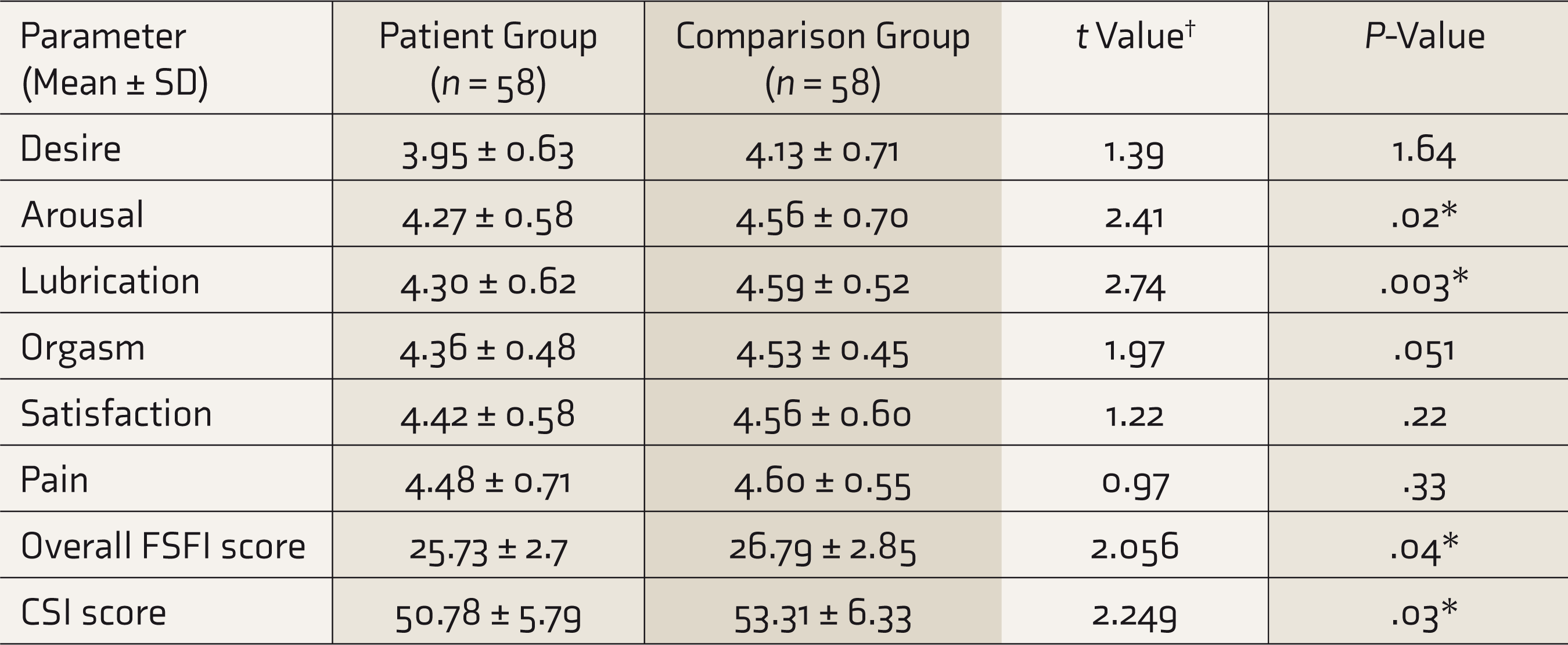
Sexual dysfunction was considered the primary outcome variable. The proportion of sexual dysfunction in the patient group was 56.89% and in the comparison group was 39.65%; the difference was not statistically significant (χ 2 = 3.45, P = .06). The mean scores of the FSFI total and CSI in the patient group were significantly lower than in the comparison group (P = .04 and .03, respectively; Table 2). Although mean scores of all subdomains of female sexual functioning were lower in the patient group, statistical significance was observed only in arousal and lubrication subdomains (P = .01 and .003, respectively; Table 2). The frequency of individual subdomains of sexual dysfunction in the patient group is shown in Figure 2.
Frequency of Sexual Dysfunction in Various Subdomains in the Patient Group (n=58)
Comparison of Various Subtypes of Female Sexual Functioning and Couple Satisfaction Between the Study Groups (N = 116)
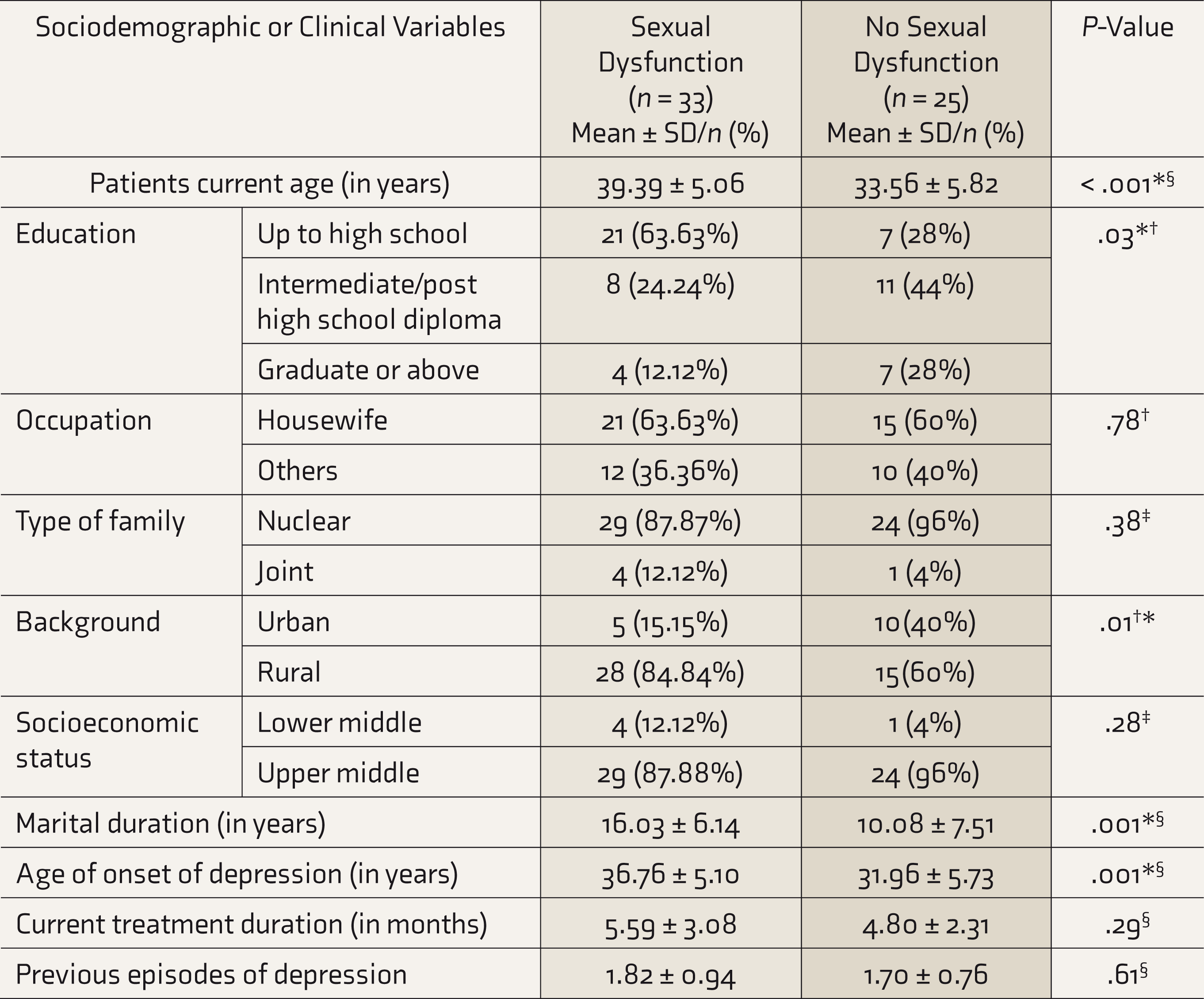
Exploratory analyses were done to compare the patients with and without sexual dysfunction on different variables. The mean age of those with sexual dysfunction was 39.39 ± 5.06 years, which was significantly higher (P <.001), and the majority of them were educated up to high school (63%, P = .03), belonged to the rural background (84.84%, P = .01), and were married for longer duration (16.03 ± 6.14 years, P <.001). No significant difference was noted among other variables. Although clinical parameters like age of onset of depression, the mean number of previous episodes, and duration of current treatment were more in patients with sexual dysfunction, these were not statistically significant (Table 3).
Comparison of Sociodemographic Details of Patients with and Without Sexual Dysfunction (N = 58)
Exploratory analyses were also done to find the associations of sexual functioning with different sociodemographic and clinical variables in the patient group. Age of onset of depression was significantly negatively correlated with total sexual functioning (P = .004) and subdomains of desire (P < .001), lubrication (P = .04), and satisfaction (P = .03). Patients residing in urban habitat had significant better overall sexual functioning (P = .02) and lubrication subdomain scores (P = .028). Level of education was significantly positively correlated with overall sexual functioning (P = .002) and the subdomains of desire (P = .002), lubrication (P = .002), orgasm (P = .04), and satisfaction (P = .004). Total duration of marriage was significantly negatively correlated with overall sexual functioning (P =.02) and subdomains of desire (P <.001), lubrication (P = .03), and orgasm (P = .03). Current treatment duration was significantly negatively correlated with lubrication subdomain (P = .03) and overall sexual functioning (P = .02). Type of the family or number of previous episodes of depression were not significantly associated with any of the subdomains or the overall sexual functioning (Table 4).
Correlation of Sociodemographic and Clinical Factors with Sexual Dysfunction Subdomains in the Patient Group (N = 58)
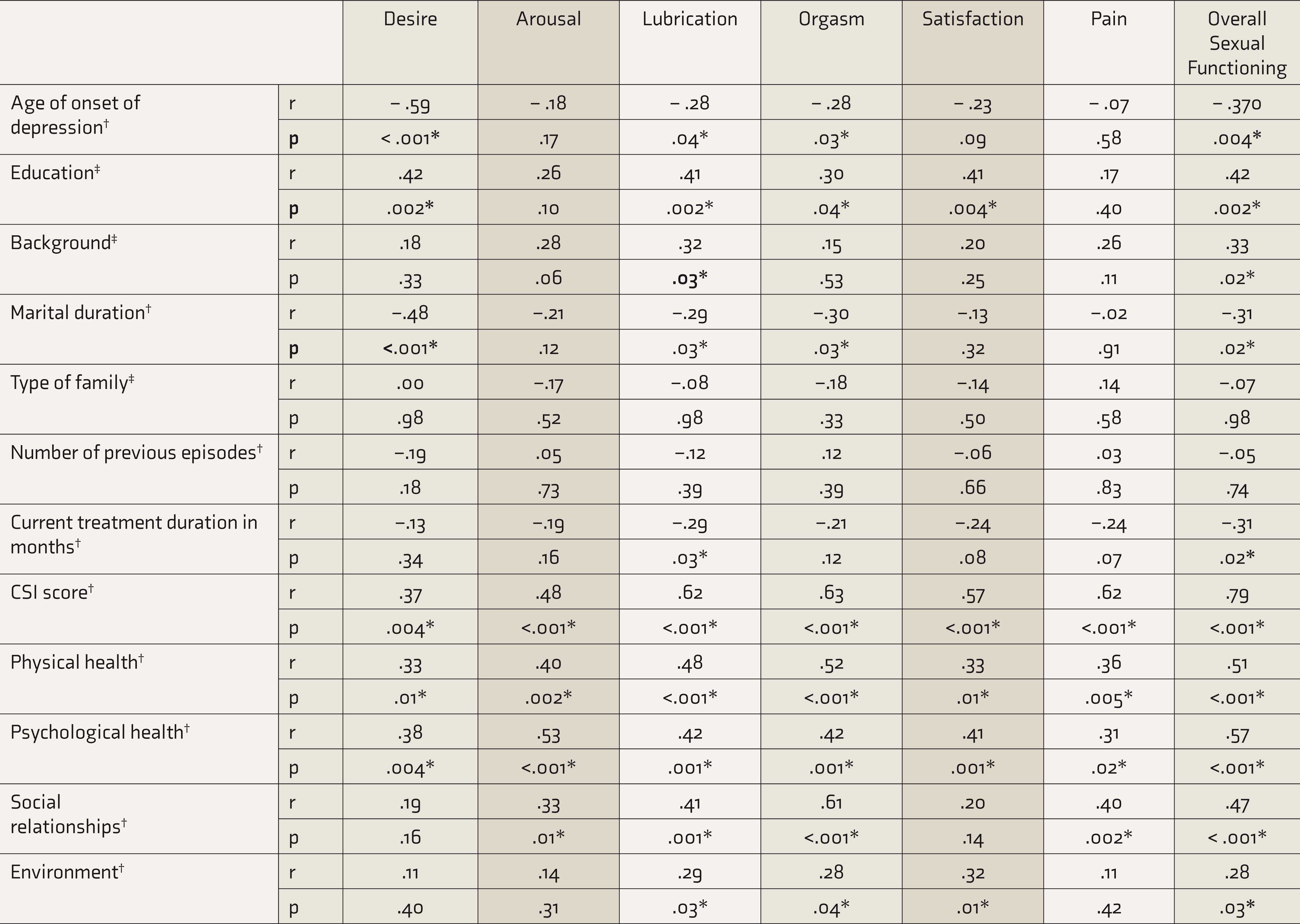
Couples’ satisfaction index scores were found to have a significant positive correlation with all domains of sexual functioning and the overall sexual functioning (P < .005). Exploratory analyses revealed that physical health and psychological health subdomains of QOL in the patient group were found to have a significant positive correlation with FSFI total (P < .001) and all subdomain scores (P < .05). Social relationship sub-domain of QOL was found to be significantly positively correlated with subdomains of arousal (P = .01), lubrication (P <.001), orgasm (P < .001), pain (P = .002), and overall sexual functioning (P < .001), whereas environment subdomain of QOL was significantly positively correlated with lubrication (P = .03), orgasm (P = .04) and satisfaction (P = .01) subdomains and the overall sexual functioning (P = .03; Table 4).
Discussion
Sexual dysfunction is a significant yet underreported problem in developing countries like India. The proportion of female sexual dysfunction in patients with depression on SSRI treatment in our study was 56.9%, which is in par with the average prevalence (40%–65%) given by a previous study. 8 The proportion of female sexual dysfunction in the comparison group also seemed high, around 39.7%, and a global study done in the general population had reported a similar prevalence rate. 24 However, there is a difference when compared to other Indian data, where the prevalence of female sexual dysfunction in the patient group was lesser (43.63%) in one study 16 and the general population was more (55.5%) in another study. 25 One of the reasons for this disparity might be the various sociocultural backgrounds, as evidenced by another south Indian study by Rao and Nagaraj, where consideration of speaking about sexual functioning and issues as “taboo” was observed. 26
In the present study, most females with remitted depression were housewives, residing in nuclear families, from urban areas, belonging to lower to middle socioeconomic status, which concord with previous literature in this area.9, 16 In our study, the proportion of female sexual dysfunction in the patient group was found to be more. SSRIs causing sexual dysfunction, a well-known fact, may be cited as one of the reasons for the increase in prevalence.
In the current study, there was dysfunction in almost all the subdomains, with dysfunction in lubrication and orgasm being the most common. These results were in contrast to other Indian data available, where most patients receiving SSRI had decreased libido, followed by reduced arousal. The other subdomains were less frequently affected in those studies.9, 16,27 This might be because of the sociocultural differences in the study population as both the other studies are from North India or had minor variations in the inclusion criteria.
In our study, the mean scores of arousal, lubrication, overall sexual functioning, and marital satisfaction were significantly lower in the patient group. A similar pattern was observed in another Indian study where the scores of all the subdomains of sexual functioning (except for pain) were significantly lower in the patient group. 9
In this study, age of onset of depression and marital duration had a significant negative correlation with desire, lubrication, and orgasm, whereas the level of education had a significant positive correlation with all the subdomains except pain and arousal. These findings were partially like the available Indian data, where the correlation was seen only to desire subdomain.9, 16 In par with literature, the previous number of episodes had no correlation with sexual dysfunction.9, 16,27 However, we found a significant negative correlation between current treatment duration and lubrication and overall sexual functioning. This is in contrast to other research where there was no correlation between treatment duration and sexual dysfunction. 9
The present study showed a strong positive correlation between sexual dysfunction and marital dissatisfaction in the patient group. There was also a significant positive correlation between marital satisfaction and all the subdomains of sexual functioning. This could be supported by the findings of a previous study that marital dissatisfaction has a negative impact on the onset, course of illness, and response and adherence to treatment, which increases the chances of relapse. 28 Marital dissatisfaction is four times more in depressed patients when compared to those without depression. 29
There was a positive correlation between components of QOL and all subdomains of sexual functioning in our study, which is similar to a study done by Whisman. 30 The fact that sexual dysfunction is correlated with marital dissatisfaction and poor QOL even in the normal controls 15 makes it furthermore worthwhile for us to focus on addressing the same in females with depression with or without treatment, which per se can lead to poor QOL.26, 29–31
However, our study had a few limitations. This hospital-based observational study is limited by a small sample size. Hence, the generalizability of the results is limited. Blinding was not done for the researcher or participants. There is a possibility of selection bias as convenient sampling was done. One of the major limitations was not including individual SSRI drugs, dosage, and other common side effects, which can be considered the scope of further studies. Medical and gynecological comorbidities and other conditions excluded were based on history and examination findings and not by laboratory confirmation. Further research can include large sample sizes and interventional/follow-up studies to avoid bias and improve the generalizability of the results. Sexual dysfunction and other parameters can be studied with respect to individual SSRI drugs.
Conclusion
Female sexual dysfunction is more in remitted depression patients and is associated with marital dissatisfaction and poor QOL. In Indian culture, considering the stigma related to women expressing problems in sexual functioning, as per our study, it is better for mental health professionals to look for sexual side effects as a routine during follow-up so that we can identify and address the issue as well before it leads to medication nonadherence and relapse of depression.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning this article’s research, authorship, and publication.
Funding
The authors received no financial support for the research, authorship, and publication of this article.