
Abstract
Introduction:
A sedentary lifestyle among young and middle-aged individuals contributes to spinal pathologies, significantly affecting quality of life (QOL). Sexuality is a key determinant of well-being, and spinal conditions—characterized by motor and sensory deficits, pain, stress, and anxiety—can impair sexual function. However, studies using validated scales to assess sexual functioning in these patients are scarce.
Aim:
Evaluate sexual functioning, marital satisfaction, and QOL in patients undergoing spine surgery.
Materials and Methods:
This prospective, questionnaire-based study was conducted from December 2022 to June 2023. Fifty-three sexually active patients (aged 20–50 years) undergoing elective spine surgery were included. Validated scales such as the ENRICH Marital Satisfaction Score (MSS) for marital well-being, the changes in sexual functioning questionnaire for males (CSFQ-M) and females (CSFQ-F) for sexual dysfunction, the Oswestry Disability Index (ODI) for disability assessment, and the WHO-QOL BREF for overall QOL were used. Assessments were done preoperatively and at one, three, and six months postoperatively. Statistical analysis was performed using SPF version 25, with a significance level of P < .005.
Results:
Preoperatively, all quality-of-life domains were affected, especially the psychological domain. The ODI showed that 94% of patients were crippled before surgery, but by six months, all had minimal disability. All participants had sexual dysfunction and marital distress preoperatively; most regained normal sexual function by three months and marital satisfaction by six months.
Conclusion:
Spinal pathologies significantly impact psychosexual functioning, marital satisfaction, and QOL. This study highlights the importance of a holistic approach to postoperative recovery.
Introduction
Spine ailments are commonly seen in orthopedic practice. A sedentary lifestyle among young and middle-aged people leads to many spinal problems. Spinal cord problems include cervical/lumbar prolapsed intervertebral disc (PIVD) with or without spinal canal stenosis/with or without neural foraminal stenosis. 1 The early stages of these spine diseases are managed conservatively through physiotherapy and epidural steroid infiltration. When medical management fails, patients undergo elective spine surgeries which include decompression at single/multi-level discectomy and laminectomy with or without pedicle screw fixation. 2 The above-mentioned spine pathologies certainly hamper patients’ quality of life (QOL). Out of the many aspects that determine QOL, sexual function is an important determinant. Sexuality is the ultimate union of body and mind, the inseparable relationship between body and mind though known from ancient times, there is very little emphasis in modern medicine. 3 A certain number of these patients are likely to suffer from sexual dysfunction, which is usually overlooked by orthopedic surgeons and thus impairs the QOL even after surgical intervention. 2 Studies on sexual function in diabetes, hip arthroplasty, chronic pain and cardiac disorder have been reported.3–5 A meta-analysis done in Africa revealed very little literature available about QOL during the postoperative period. 6 Another study in neurosurgical patients revealed that there was a significant improvement in the QOL after surgery based on the visual analogue scale as well as the Oswestry Disability Index (ODI). 7
A retrospective study conducted at the University of Pennsylvania found that older adults following thoracolumbar to pelvic instrumentation for spinal deformity had either no or mild sexual dysfunction, suggesting that despite an older age and extensive spinopelvic instrumentation, it is possible to maintain or achieve satisfactory sexual function. 8 Another study done at the University of California on sex life and the impact of operative intervention on sex-life-related pain in degenerative spinal conditions showed that operative treatment leads to improved sex life-related pain. 2 There have been reports of improved sexual functioning after successful treatment of chronic pain and lumbar disc herniation. 8 Motor and sensory deficits, excruciating pain, sciatica, anxiety, and stress can impair concentration, subsequentially leading to deficits in performing daily activities. Impairment in activities may instigate financial constraints and stress, which sequentially results in impaired QOL. This also affects different areas of life, which comprise interpersonal, familial, and psychosexual. These factors usually go unrecognized either because of ignorance or lack of knowledge about the same. It is essential to address these factors, whether treated surgically or medically, to give a holistic treatment and improve the QOL of the individuals. 9 Several studies have been conducted on functional outcomes and QOL in post-spine surgery, but there are insufficient studies conducted on the Indian population.11,8–10 This study emphasizes QOL and psychosocial well-being in post-spine surgery patients with an aim to assess the QOL and psychosexual well-being in patients undergoing elective spine surgeries as well as to assess marital satisfaction and sexual functioning pre and postoperatively.
Materials and Methods
This was a prospective questionnaire-based observational study conducted in the Department of Orthopedics at a tertiary care hospital, spanning from December 2020 to June 2022.
The sample size was calculated using the formula N = (Zα + Zβ)² × σ² / d²) with α (probability of Type I error) set at 0.05, β (probability of Type II error) at 0.80, Zα (critical value for α) at 1.96, Zβ (critical value for β) at 0.84, the clinically relevant effect size (d) to detect was 4, and the population’s standard deviation (σ) was 5.2. As a result, the calculated sample size for the study was 53.
It was approved by the Institution Ethics Committee vide approval number [JSS/MC/PG/5156/2020-21]. Informed consent was duly obtained from all study participants, ensuring that they were informed about the study’s objectives and procedures and provided their voluntary consent to participate. It included patients within the age range of 20–50 years, patients of both genders who were admitted for elective spine surgeries, with an active lifestyle and a history of sexual activity. Patients who were suffering from other medical ailments like uncontrolled diabetes, hypertension, ischemic heart disease, debilitating neurological disease etc., and those who had substance or medication-induced sexual dysfunction and traumatic spine injuries were excluded from the study.
QOL was evaluated using the WHO-QOL BREF scale,5,11 and Disability was assessed using the ODI.12,13 Sexual Functioning was assessed separately for males and females using the changes in sexual functioning questionnaire for males (CSFQ-M) and females (CSFQ-F), 14 and last, marital satisfaction was assessed using the ENRICH Marital Satisfaction Score (MSS). 15 These were administered on the day before surgery and subsequently at one, three, and six months post-surgery.
Statistical analysis was performed using SPSS Version 25, and a P value of <.005 was considered significant. Mean and standard deviation were used for socio-demographic data. ANOVA was used for the different domains of QOL. Postoperative comparison for QOL was done using the Bonferroni test to determine inter-group variation. The percentage was used for sexual dysfunction as well as marital satisfaction.
Results
Socio-demographic Details
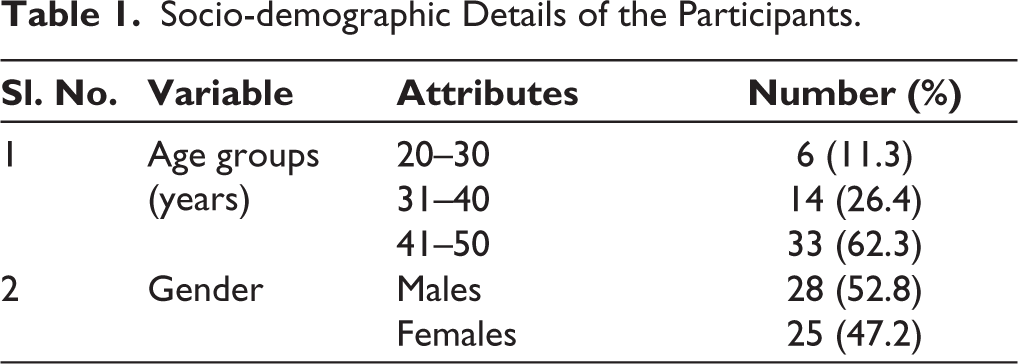
The majority of the participants, 33 (62.3%), were in the age group of 41–50 years, and most participants were males, 28 (52.8%) (Table 1).
Socio-demographic Details of the Participants.
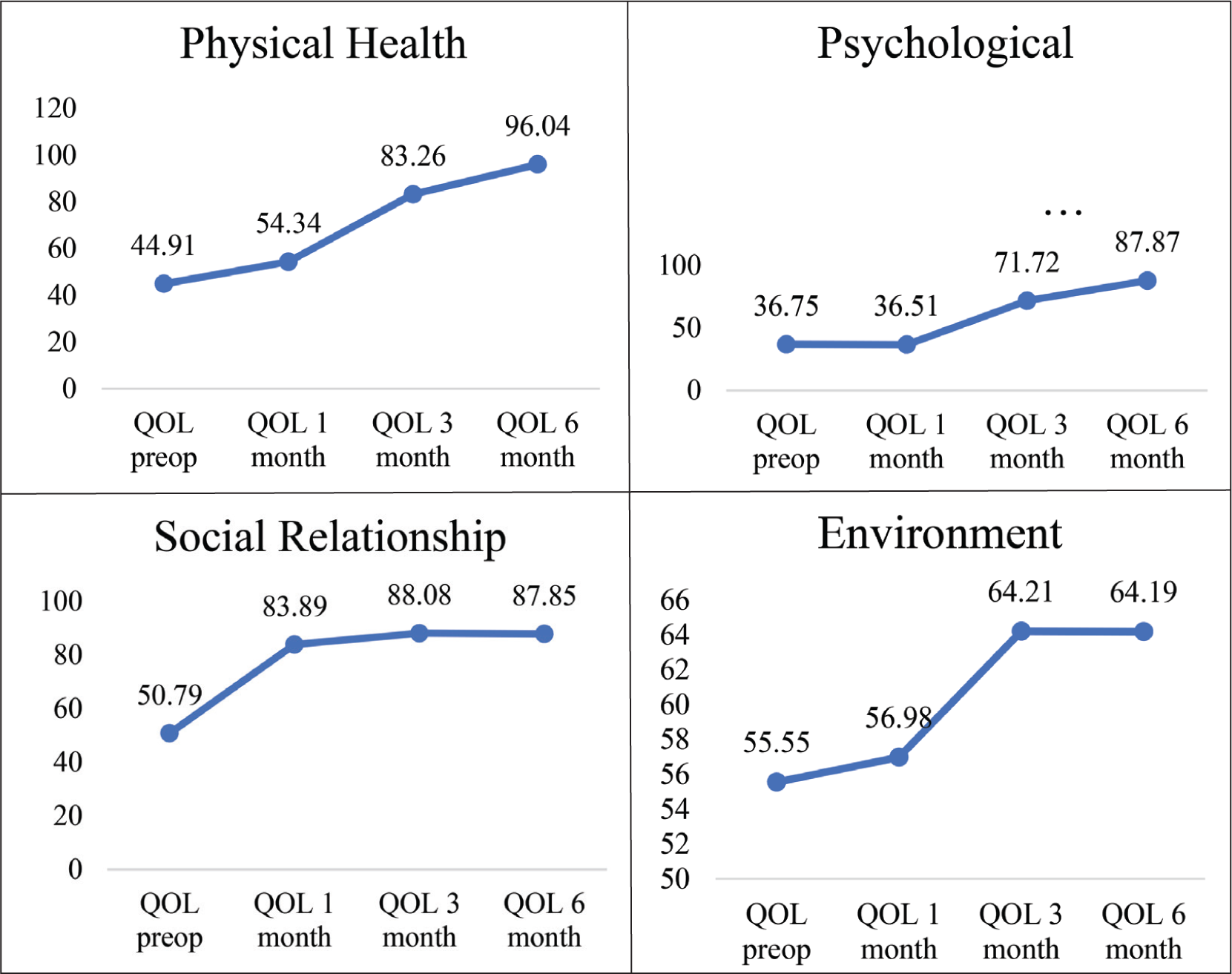
Quality of Life (Figure 1)
The graph depicts the comparison of different domains of QOL over the follow-up period. In the preoperative period, though all four domains of QOL were affected; the psychological health was the most affected. Using the Bonferroni test (post-hoc analysis), the psychological domain showed significant intergroup variation (P < .005). Psychological health was the most affected, which continued till the end of the first month post-operative. The environment domain was significantly affected and showed significant inter-group variation at the end of the third and sixth month post-operative.
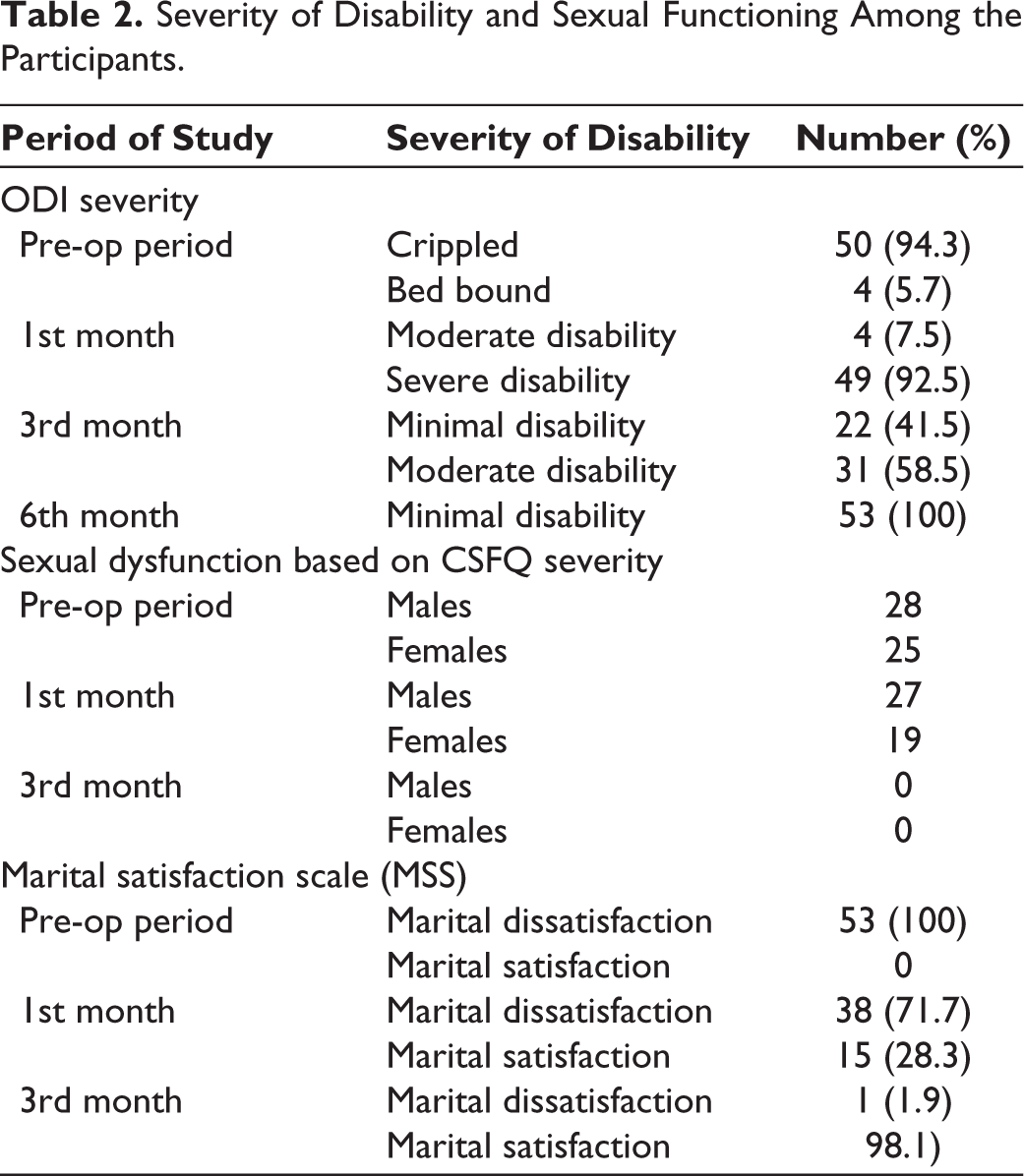
ODI, CSFQ, and MSS Scores Among the Participants (Table 2)
ODI during the pre-operative period shows that 94.3% were crippled, and 5.7% are bed bound. Post-operatively, the scores steadily declined over six months to minimal disability. In the CSFQ, pre-operatively, all participants had sexual dysfunction. The scores improved post-operatively, and by the end of three months, all the participants had normal sexual functioning. Similarly, marital satisfaction improved post-operatively, and by the end of six months, all the participants reported satisfaction.
Severity of Disability and Sexual Functioning Among the Participants.
Discussion
A study by Wagner A et al. found that the QOL improved over twelve months post-operatively. 16 Similar changes in QOL postoperatively were found by Vivian Amarlal et al. 17 and Silky Chotai et al. 18 Studies by Nikhil R Nayak et al. and Lukman Olalekan Ajiboye et al. found significant improvements in outcomes among the participants in different treatment modalities, with surgical treatment being superior.6,19 The improvement in the QOL may be explained by multiple factors, which include a decrease in the disability, improvement in the marital satisfaction and as well as improvement in sexual functioning. 18
Sexual function in spine problems and the impact of corrective surgeries on the same are not well researched. Although there were studies evaluating sexual functioning in pain, literature about sexual dysfunctions in spinal pathologies is scarce. Baumer and Walker proposed two reasons for neglect in research in this area “Firstly, physicians are not routinely trained to explore the sex life of their patients, and secondly, there has been a stifling trend in research to investigate only what can be measured by objective methods.” 20 Similar to this study, a study done in Germany showed that most patients (82%) reported satisfaction with the overall outcome of the surgery, including sexual functioning. 21 In continuation, they also found that women experienced more frequent sexual dysfunction than men. Previous data confirm that women experience more sexual problems, the most common being a lack of sexual interest, non-pleasurable sex, and lubrication difficulties. 22
Studies have found that social factors like unemployment and low income can compromise sexual desire. A German study found that 14% of people reported a deterioration of sexual life due to persistent pain and aging, 21 they also found a negative correlation between aging and sexual desire, arousal and activity. The current study did not find any correlation between age, sex, professional status, and sexual dysfunction. According to a study on predictors of the outcome of sexual functioning, the surgical procedure itself can be an independent predictor of sexual function. 19
In line with the current study, previously published data also showed microdiscectomy of lumbar disc herniation and surgical treatment of degenerative conditions had positive effects on the frequency of intercourse, erectile dysfunction and premature ejaculation.20,22 Studies which tried to compare the impact of different surgical approaches on sexual dysfunction found that neither total disc replacement nor fusion had any adverse effects on men’s erections or retrograde ejaculation. Before surgery, 34% of patients claimed that having sex added some extra lower back pain (LBP), and 30% claimed that having sex significantly limited their LBP. Both groups’ sexual lives improved post-surgery, and a direct link between LBP and improved sex lives was established. Despite a decrease in LBP, 26% of all men in the Fusion group experienced postoperative impairment in their capacity to reach orgasm, compared to 3% of men in the total disc replacement group, but in contrast to our study where all the participants had improvement in their sexual functioning six months post-surgery. 18
A study recommended that patients with degenerative lumbar spondylolisthesis have surgery, to indicate that the condition had a detrimental impact on their sexual life. 19 Similarly, a study by Schulz et al. reported that LBP patients in the operative group were having a higher percentage of pain related to sex at baseline as compared with the control group which showed a drastic improvement in sex-related pain (decreased to <20%) in an operative group on follow up, whereas in the non-operative group, there was no significant improvement in sex-related pain. 21
Sexual intimacy is a way of connecting with partners, which also enhances the sense of well-being. People of all ages and abilities are involved in sexual intimacy. A study demonstrated that sex life was relevant to most patients with spinal cord problems. 22 When patients are suffering from illness, it often precludes them from discussing sexual health. Even after recovering, patients may still face challenges related to sexual dysfunction. This may occur because healthcare professionals often lack knowledge about sexual dysfunction and its treatment, which can result in their failure to acknowledge these issues. Being aware of sexual dysfunction and its association with the diseased organ system is the first step in treating sexual dysfunction. When healthcare professionals embark on the topic, patients willingly discuss sexual problems. 23
There is an increase in interest in the interpersonal nature of chronic disease in modern-day research. 24 Studies done in the past report that there are widespread marital and sexual problems in patients suffering from chronic pain. 20 Chronic pain seriously affects the relationships of patients with relatives and intimate partners. Although it affects family, children and extended family members, the partnership is thought to be the most affected. 25 Partners experience various challenges like reduced QOL, psychological distress and negative effects on social life. 7 Emotional, sexual and communication problems among couples lead to decreased marital adjustment. 26 The satisfaction of the couples with their marriage is called marital satisfaction. 15
The marital crisis model shows that women and men can experience marital dissolution differently. Neither does all marital loss result in compromised well-being, nor does marriage enhance well-being, highlighting complex dynamics worthy of further investigation in this population. 26 The MSS during the preoperative period among the study participants shows that 100% of the participants had marital distress/dissatisfaction. The MSS after one month of the surgery revealed that most participants had marital dissatisfaction (71.7%), while marital satisfaction was seen in 28.3% of the participants. 98.1% of the participants had marital satisfaction in the third month post-surgery, and very few (1.9%) had marital dissatisfaction. 27 This displays that in our study, there is a drastic improvement in marital satisfaction post-operatively as compared to preoperative time. Our study links with Mahsa Yousefi et al., who stated that the marital adjustment in patients who underwent laminectomy surgery significantly improved compared to pre-operative in all dimensions like mutual agreement and expressing affection, and solidarity. 28 Earlier studies suggest that disability, anxiety and depression lead to decreased MSS during the preoperative period.29–31
A large study which included 4,864 men and 1,277 women which was a fifteen-year long-term follow-up study in patients with traumatic spinal cord injury showed hypothesis testing—supporting the marital crisis model. 32 Marital loss through being or becoming separated, separated, or divorced, being or becoming widowed had a consistent and negative impact on all the well-being outcome measures. While being or becoming married had only the advantage of decreasing depressive symptomatology over time. The impact of marital dissolution on well-being outcomes was not uniform. It was moderated by gender, such that widows had poorer self-perceived health and more depressive symptomatology than men. While divorced women had higher life satisfaction and self-perceived health than men. 31 Our study is only a six-month follow-up study, so we could not find any marital transitions during that period.
In the current study, there is improvement in QOL, disability and psychosexual well-being in patients undergoing elective spine surgeries. It is very important to address these factors, whether treated surgically or medically, to give a holistic treatment and improve the QOL of the individuals. Studies using validated questionnaires would help to give more insights to the medical fraternity to improve the quality of sexual life of their patients
Conclusions
There is a considerable psychological and emotional burden on patients undergoing treatment for spinal cord disease and intractable pain. Despite displaying severe psychological suffering before surgery, patients may significantly benefit from treatment. Their QOL improves with progress after the time of surgery. As the QOL improves, their psychosexual conditions and marital status are better when compared to preoperative time.
Limitations
One of the limitations of the study is that sensitive topics like sexual functioning: People are hesitant to give information on sensitive topics like sexual functioning, which may have had an impact on the outcome of the study. During the early part of the assessment, the study participants were in the hospital, which could be a limiting factor for sexual functioning.
Footnotes
Acknowledgements
We appreciate the continuous support provided.
Author Contributions
Mohammad Jasim Hussain: Contributed to concepts, design, definition of intellectual content, literature search, data acquisition, manuscript preparation, and manuscript review.
Purushotham Sastri: Participated in design, definition of intellectual content, literature search, data acquisition, manuscript editing, and manuscript review.
Raj Kiran Donthu: Involved in the definition of intellectual content, literature search, manuscript editing, and manuscript review.
Shivananda Manohar J: Contributed to the definition of intellectual content, manuscript editing, and manuscript review.
TSS Rao: Responsible for data analysis, statistical analysis, guarantor, and manuscript review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Generative AI in Scientific Writing
We have not used any Artificial Intelligence (AI) tools in writing the manuscript (except Zotero as a referencing tool and Grammarly for grammar corrections).
Ethical Approval
The study was approved by the Institution ethics committee (IEC) approval number: JSS/MC/PG/5156/2020-21.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was duly obtained from all study participants.
Reporting Guidelines
The observational study has been prepared according to STROBE guidelines.
Submission Declaration and Verification
The manuscript has not been published previously, nor it is under consideration for publication elsewhere, and its publication has been approved by all authors.