
Abstract
Erectile dysfunction is a major chronic condition affecting hundreds of millions of individuals worldwide. This review provides a concise overview of research on the psychological experience of erectile dysfunction. There is evidence that psychological factors such as personality, depression, stress, and cognitive interference (e.g., performance worry, shifts in attentional focus) contribute to erectile problems. There is also evidence that the experience of erectile dysfunction can have negative psychological effects, including feelings of emasculation and humiliation, decreases in self-confidence and feelings of self-worth, feelings of isolation and loneliness, increases in depression, and decreases in subjective well-being. Effects on the affected individuals’ sexual partner include feelings of being unattractive, feelings of rejection, feeling unloved, decreases in self-esteem, and frustration. Psychological interventions (particularly multimodal interventions) show promise for treating erectile dysfunction, but more research is needed to help establish their effectiveness. We present a brief research agenda of critical areas in need of further study. This review should be of interest to the general public and also researchers looking to develop a program of research in sexual health psychology that focuses on the psychological experience of erectile dysfunction.
Erectile dysfunction is most commonly defined as a consistent or recurrent inability to attain or maintain an erection that is sufficient for sexual satisfaction (McCabe et al., 2016). The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders also considers that symptoms need to persist for more than 6 months and be causing significant distress in order to qualify as erectile dysfunction (American Psychiatric Association, 2013). This definition serves as a useful generalized description of the condition, but it is worth noting that it might be based on heteronormative assumptions, and it is unknown whether this definition is useful for individuals who identify as transgender or nonbinary (see Whitney et al., 2022). Erectile dysfunction is a major chronic condition affecting hundreds of millions of individuals worldwide. Indeed, in healthy populations, the risk of erectile dysfunction increases across the adult life span, with prevalence rates at approximately 20% before age 30 years, 25% at age 30 to 39 years, 40% at age 40 to 49 years, 60% at age 50 to 59 years, 80% at age 60 to 69 years, and 90% in individuals above 70 years of age (Allen & Walter, 2019; Geerkens et al., 2020). Erectile dysfunction is often classified as biological in origin (e.g., caused by injury, drug use, or cardiovascular damage) or psychological in origin (e.g., caused by life stress, depression, or intrusive thoughts during sexual activity) but most often reflects a combination of both biological and psychological factors (Shamloul & Ghanem, 2013; Yafi et al., 2016). Until recently, relatively little attention had been paid to the psychological aspects of erectile dysfunction. This review aims to provide a succinct overview of contemporary research that has explored psychological processes in the experience of erectile dysfunction.
Psychological Contributors
There are many factors that can increase risk of erectile dysfunction, including lifestyle habits, genetics, neurological-psychiatric disorders, drug use, and cardiovascular conditions (Allen & Walter, 2019). However, psychological factors have also been found to have a critical role in the experience of erectile dysfunction. A general model of psychological processes in the experience of erectile dysfunction is illustrated in Figure 1. In terms of more stable (long-term) risk factors, there is evidence that people who score higher on neuroticism and lower on extraversion are at greater risk of erectile dysfunction (Allen & Walter, 2018), and this is thought to reflect the different lifestyle habits of people with these personality traits. Indeed, there is considerable evidence that people who score higher on neuroticism and lower on extraversion are more likely to be active cigarette smokers and take part in less physical activity across the life span (Strickhouser et al., 2017), and both physical inactivity and cigarette smoking are major contributors to erectile dysfunction (Allen, 2019; Allen & Tostes, 2023). Personality traits also relate to sexual attitudes and schemas (Allen & Walter, 2018) that might act as additional risk factors for erectile dysfunction. Psychological states such as stress and depression can also contribute to erectile dysfunction (Atlantis & Sullivan, 2012; Liu et al., 2018), with some treatment approaches (e.g., antidepressant medication) also found to exacerbate the problem (Rothmore, 2020). Moreover, chronic stress (e.g., work stress) and mental health conditions (such as depression) contribute to elevated cortisol levels and increased sympathetic nervous system activity (relative to parasympathetic activity) that can disrupt erectile processes (Dick et al., 2020).
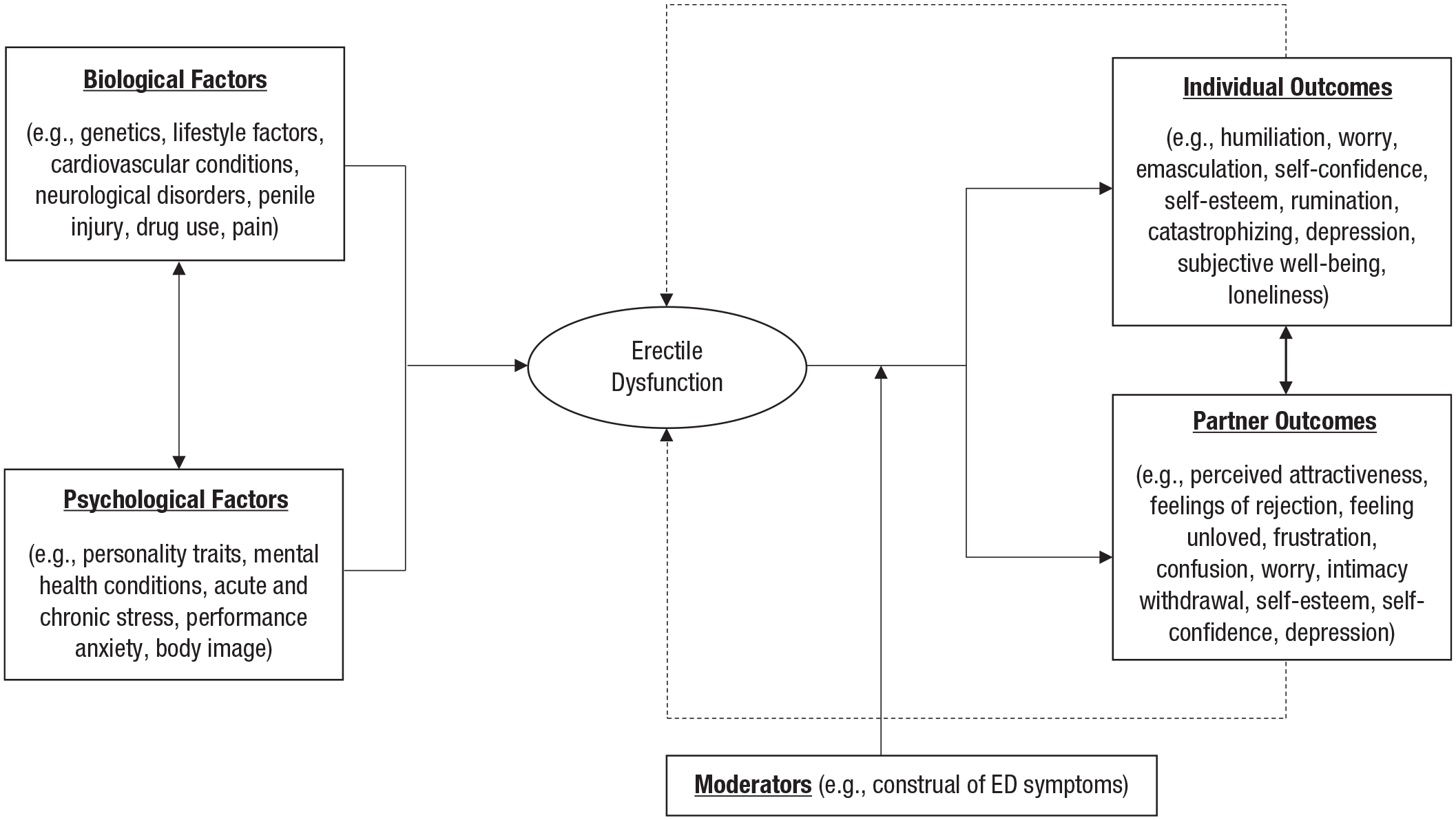
A general model illustration of key psychological contributors and outcomes of erectile dysfunction (ED).
In terms of more short-term psychological contributors, cognitive factors in the moment, such as worry (performance anxiety) and interfering thoughts, can distract from sexual stimuli that trigger signals from the brain to the penis to initiate and maintain erection. A systematic review of 67 studies found that cognitive-processing factors make a major contribution to sexual dysfunction in both women and men (Tavares et al., 2020). In particular, performance worry (before, during, and after sexual activity)—thoughts such as “I’m a complete failure because my erection was not 100%” or “I’m sure it won’t work tonight”—can contribute to disruptions in erectile function. Change in attentional focus during sexual activity appears to be a central issue, with men reporting a shift toward their own thoughts and sensations during a difficult sexual situation (a shift from an external to an internal attentional focus), a loss of automaticity in sexual behavior, and disengagement from the moment (e.g., erection concern thoughts during sexual activity) as coinciding with erection problems (Giuri et al., 2017; Tavares et al., 2020). The attributions made for erectile dysfunction are also important, with people making more internal attributions (e.g., biological causes) more likely to develop consistent erectile problems than those making external attributions (e.g., tiredness, stress) for sexual difficulties (Tavares et al., 2020).
Psychological Outcomes
A considerable amount of research has explored how the experience of erectile dysfunction can affect subsequent psychological states. One of the most common initial reactions to erectile dysfunction is a sense of emasculation (Sheng, 2021). Even a single occurrence of erectile dysfunction can trigger feelings of humiliation and shame as well as worry that one’s partner might leave them and feelings of letting their partner down (Sheng, 2021). Other common responses to erectile dysfunction include decreases in self-confidence and feelings of self-worth, feelings of isolation and loneliness, rumination and catastrophizing, and a more negative body image (Dewitte et al., 2021). These psychological responses can also act as a self-fulfilling prophecy, as worry about letting one’s partner down or worry that their partner might leave them can lead to the affected individual withdrawing intimacy at a time when their relationship is particularly vulnerable, resulting in their partner feeling unwanted and unloved (Sheng, 2021).
In terms of more long-term effects of erectile dysfunction, a 20-year systematic review of nine studies on erectile dysfunction and quality of life found that people who suffer from erectile dysfunction show a greater deterioration in psychological, social, and physical well-being compared with those without erectile dysfunction (Elterman et al., 2021). The relationship between erectile dysfunction and depression has also been found to be reciprocal in nature. A meta-analysis of 12 studies found that not only does depression contribute to an increased risk of erectile dysfunction but also the experience of erectile dysfunction is associated with a three-fold increase in the risk of a subsequent diagnosis of depression (Atlantis & Sullivan, 2012). In addition to depression, a meta-analysis of 12 studies (Velurajah et al., 2022) also found that erectile dysfunction was associated with an increased risk of anxiety disorders (posttraumatic stress disorder, obsessive-compulsive disorder, social phobia/social anxiety disorder, and panic disorder). However, much of the research on erectile dysfunction and mental health conditions has adopted case-control study designs, meaning that establishing cause and effect is not possible.
Interpersonal Psychological Outcomes
In addition to the psychological distress experienced by the affected individual, erectile dysfunction can also have substantial implications for the affected individuals’ sexual partner. Most people who have a partner who suffers from erectile dysfunction report that it is a problem for their relationship (Sheng, 2021). Common affective responses (when a partner suffers from erectile dysfunction) include feelings of being unattractive, feelings of rejection, feeling unloved, and frustration (Sheng, 2021). Erectile dysfunction can also cause trust issues in partners who interpret a man’s erection as a sign of sexual attractiveness (Dewitte et al., 2021). Erectile dysfunction can lead to intimacy withdrawal, and such changes in sexual behavior can cause confusion for the partner, worry of an affair, and a belief that the man is losing interest. These anxious thoughts can have a major impact on self-esteem and feelings of attractiveness (Li et al., 2016). Moreover, a systematic review of eight studies found that partners of those who suffer from erectile dysfunction report a lower quality of life (Elterman et al., 2021).
Erectile dysfunction can also affect sexual partners in other ways. For example, studies of heterosexual couples have observed a positive association between erectile dysfunction and female sexual dysfunction (Wang et al., 2022). In particular, after their partner had developed erectile dysfunction, women report a decrease in sexual impetus, including a decrease in sexual desire, sexual arousal, and orgasm during sexual intercourse that, in turn, led to discontent in the relationship, lower sex-life satisfaction, and general life satisfaction (Li et al., 2016). A partners’ understanding of erectile dysfunction is also important for couple outcomes. Most patients with erectile dysfunction (~87%) and their partners (~82%) rate open discussions of erectile function and sexual activity as important for maintaining a good relationship, and almost all people with erectile dysfunction (~95%) felt that their partner’s support was important (Li et al., 2016). However, a substantial number of individuals (~22%) felt that the reaction of their partner had been negative (Li et al., 2016). The attitude, behavior, and understanding of the sexual partner are important influential factors in managing erectile dysfunction, and interventions that focus on couples, rather than just the affected individual, are thought to be a better approach to improving erectile function (Li et al., 2016).
Psychological and Multimodal Interventions
Many treatment approaches have been explored for erectile dysfunction, including lifestyle modification, testosterone supplements, phosphodiesterase type 5 (PDE5) inhibitors (e.g., Sildenafil [marketed as Viagra]), intracavernosal self-injection therapy, nutraceuticals, vacuum erection pumps, and extracorporeal shock wave therapy, with varying levels of success (see Beecken et al., 2021). Psychological interventions have also been met with varying levels of success. For example, a study of 31 men with erectile dysfunction found that an 8-week stress management program was effective in reducing perceived stress and cortisol levels, but there were no significant effects on erectile function (Kalaitzidou et al., 2014). In another small-sample study of 20 men with erectile dysfunction, those assigned to 10 weeks of cognitive behavioral therapy showed greater improvements in erectile function than those in the control group (Khan et al., 2019). In these studies, men in both control and intervention groups were also using PDE5 inhibitors in their treatment of erectile dysfunction.
Research syntheses have produced somewhat unclear results regarding the effectiveness of psychological interventions in erectile dysfunction treatment. A systematic review of 11 studies found that group psychotherapy, psychoeducational intervention, and rational-emotive behavior therapy appeared effective in improving erectile function (Melnik et al., 2008). However, a meta-analysis of seven studies (Frühauf et al., 2013) found that psychological interventions had no effect on erectile dysfunction (d = 0.53, 95% confidence interval [CI] = [–0.08, 1.14]). There is substantial heterogeneity in results, and this likely reflects the varied study designs in primary research. Indeed, an umbrella review of 98 meta-analyses observed that psychological interventions were considerably more inconsistent in their effectiveness compared with medication (Allen & Walter, 2019). Research exploring how psychological interventions combined with PDE5 inhibitors compare with PDE5 inhibitors alone has produced more consistent results. A meta-analysis of eight studies (Schmidt et al., 2014) found that combination treatment was superior to PDE5 inhibitors alone (d = 0.45, 95% CI = [0.03, 0.89]), and a systematic review of 13 studies (Atallah et al., 2021) found that combination therapy (PDE5 inhibitors combined with cognitive behavioral therapy, group therapy, couple therapy, or Internet-based interventions) appeared to produce greater gains in erectile function compared with PDE5 inhibitors alone. However, these studies also show substantial heterogeneity, and deciphering the most effective methods for psychological intervention requires further research.
Research Agenda
From the research reviewed, it is clear that psychological factors have an important role in the experience of erectile dysfunction. However, this topic is still in its infancy, and more research is needed to help understand how psychological factors contribute to and might be implicated in the treatment of erectile dysfunction. What follows is a brief agenda to highlight key avenues for future research.
One observation from the research exploring risk factors and consequences of erectile dysfunction is that most studies have adopted case-control designs, meaning that it is not possible to establish whether the variable being assessed (e.g., stress, depression) is a precursor or an outcome of erectile dysfunction. The field could certainly benefit from more longitudinal designs, with rigorous control of potential confounding factors (e.g., lifestyle, personality), that explore how change in erectile function over time coincides with change in psychological states. Moreover, our model illustrates feedback loops and the potential for cyclic effects as outcomes of erectile dysfunction (e.g., depression, sexual anxieties) feed into further erectile problems and, in turn, greater increases in these negative outcomes. Research using multiple time points might look to incorporate statistical path modeling that can explore these potential cyclic effects.
It is also important that research starts to move away from exploring average effects to identifying boundary conditions under which associations might operate. For example, the extent to which erectile dysfunction affects well-being and quality of life (for both the affected individual and their partner) might be contingent on personal attitudes toward sexual activity across the life span. Research should aim to identify important moderators of associations discussed in this review.
The field would also benefit from a greater integration of biological and psychological processes. As mentioned earlier, personality traits are thought to influence erectile function through lifestyle habits (Allen & Walter, 2018), but research has yet to test these mediation effects. The degree to which depression, chronic stress, or anxiety affect erectile function through lifestyle (or other biological processes) also remains unclear. Further study of biological and psychological interactions can contribute to theoretical development of the causes of erectile dysfunction.
Another area for further study is understanding erectile dysfunction in minority groups, such as those who identify as nonbinary, transgender, or asexual. Sexual well-being in transgender or nonbinary individuals is highly variable and individualized, and this can be a challenge for defining and researching erectile dysfunction (Whitney et al., 2022).
Tied into the point above, research on erectile dysfunction would benefit from sampling more diverse populations in general. For example, most research has been conducted in Asia, Europe, and North America, but little is known about the psychological factors involved in the experience of erectile dysfunction outside of these regions. Furthermore, although a small body of research exists on erectile dysfunction in nonheterosexual men (e.g., Li et al., 2016), this area is considerably underresearched in comparison with research on heterosexual men.
Another important area of study relates to affected individuals’ construal of erectile dysfunction. The degree to which erectile dysfunction affects outcomes such as depression and well-being might be contingent on individual interpretation of erectile dysfunction symptoms. For example, an individual with the mindset that “I can sexually please my partner in other ways, which is still exciting for me” might be less likely to be adversely affected by erectile dysfunction. If erectile problems do not cause any distress, then the person would not be considered to be experiencing erectile dysfunction according to standard definitions (e.g., American Psychiatric Association, 2013); however, mindset varies on a continuum, and there is a substantial difference between mild frustration and catastrophizing. Future research should look to develop assessments that can capture erectile dysfunction interpretation and factor these beliefs into research exploring the psychological outcomes of erectile dysfunction.
It is also evident that little is known about the role of general practitioners (GPs) and health care providers. Research has found that most GPs do not inquire directly about erectile dysfunction with their patients (Sussman et al., 2016), and a number of psychological factors can prevent patients from raising issues about erectile function with their GP, the most frequent being “too embarrassed” (Rasmussen et al., 2020). Many individuals report that they are unsatisfied with their erectile dysfunction treatment, given the heavy focus on PDE5 inhibitors (Sussman et al., 2016). Mild adverse events associated with PDE5 inhibitors include headaches, nasal congestion, flushing, and dyspepsia experienced by 10% to 25% of patients (Chen et al., 2015). Further studies of GP treatment approaches could be beneficial in helping psychological treatment becoming more mainstream.
The body of research exploring psychological intervention in the treatment of erectile dysfunction would also benefit from more high-powered studies. For example, of the 13 studies included in the systematic review of multimodal interventions (Atallah et al., 2021), the mean sample size across studies was 43 (Mdn = 31). More high-powered intervention studies can help to establish more precisely how effective psychological interventions are in the treatment of erectile dysfunction.
Conclusions
Erectile dysfunction is a major chronic condition that can have substantial implications for well-being and quality of life for both the affected individual and their partner (Elterman et al., 2021). There is evidence that psychological factors such as personality, depression, stress, and cognitive interference (e.g., performance worry, shifts in attentional focus) contribute to erectile problems. There is also evidence that the experience of erectile dysfunction can have negative psychological effects, including feelings of emasculation and humiliation, decreases in self-confidence and feelings of self-worth, feelings of isolation and loneliness, increases in depression, and decreases in subjective well-being. Effects on the affected individuals’ sexual partner include feelings of being unattractive, feelings of rejection, feeling unloved, decreases in self-esteem, and frustration. Psychological interventions show promise in their ability to contribute to the treatment of erectile dysfunction, but more research is needed to help establish the efficacy of these treatments. We hope this review will benefit researchers aiming to develop a program of research in sexual health psychology that focuses on the psychological experience of erectile dysfunction.
Recommended Reading
Allen, M. S., & Walter, E. E. (2019). (See References). An umbrella review of meta-analyses on erectile dysfunction risk factors and treatment.
Atallah, S., Haydar, A., Jabbour, T., Kfoury, P., & Sader, G. (2021). (See References). A systematic review of combination therapy compared with medication in the treatment of erectile dysfunction.
Dewitte, M., Bettocchi, C., Carvalho, J., Corona, G., Flink, I., Limoncin, E., Pascoal, P., Reisman, Y., & Van Lankveld, J. (2021). (See References). A review of psychosocial processes and treatment guidelines in the experience of erectile dysfunction.
Li, H., Gao, T., & Wang, R. (2016). (See References). A review of interpersonal factors involved in the experience of erectile dysfunction.
Tavares, I. M., Moura, C. V., & Nobre, P. J. (2020). (See References). A systematic review of research on cognitive-processing factors and sexual dysfunction.