
Abstract
Introduction: Sexual health issues are highly prevalent but are underdiagnosed and underrecognized in day-to-day clinical practice. The lack of awareness of the specific health care needs of the patients with sexual dysfunctions and resource limitations might be certain reasons why many hospitals are not been equipped with the sexual health care units. There is paucity of specialized psychosexual health care services across the country. Trained interdisciplinary team with prepared environment in sexual medicine is the need of the hour. We started this psychosexual medicine unit with an emphasis on sexual wellness to deliver comprehensive sexual health care which will be a primary care linkage to patients presenting with symptoms of sexual disorders, so also treatment emergent sexual dysfunction in psychiatry and other medical and surgical branches.
Aim: To portray the methods, opportunities, and challenges that we experienced in establishing a specialty psychosexual medicine facility as a different unit in a private university-based medical college and hospital in Mysuru, India.
Methods: This triweekly psychosexual medicine unit is situated in the Outpatient Division of Psychiatry and is staffed with a multidisciplinary group of health care professionals. Structured survey tools and proforma are utilized to assess all patients. Case conclusions are made according to International Classification of Diseases, Tenth Revision, symptomatic/clinical explanations and diagnostic recommendations, and furthermore Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) when required. Patient care included interventions in the form of psychotherapy and pharmacotherapy.
Results: It is possible to set up a functional psychosexual medicine facility as a different unit with a trained interdisciplinary group of professionals. Patient-centered approach is vital in our care plan and management. Postgraduate students and internees posted in psychiatry division have been undertaking rotations respectively as per their duty rota. There is also a robust academic program that includes once-weekly seminars pertaining to topics of psychosexual health and monthly journal club gatherings interchanging with seminars on sexual health and well-being appraisal devices.
Conclusion: By investing on improving infrastructure and available human resources, the specialty psychosexual medicine unit was established. The psychosexual medicine unit not only gave chances for a more comprehensive assessment of individuals with sexual disorders but also improved training and education for residents with focused interdisciplinary research in the field of sexual medicine. It portrays a versatile model that can be replicated in settings of similar type.
Keywords
Introduction
Health is a state of complete physical, mental, and social well-being, and not merely an absence of disease or infirmity. 1 Sexual health has been defined by the World Health Organization in 1975 as “the integration of the somatic, emotional, intellectual and social aspects of sexual beings in ways in which are positively enriching and enhance personality, communication and love.’’ 2
Psychosexual medicine is a psychosomatic medicine applied to sexual disorders. It is a medical specialty dedicated to the assessment, diagnosis, and therapy of patients with sexual health problems and sexual dysfunction resulting from difficulties arising at various levels of sexual response cycle, which includes desire, excitement, or orgasm. Sexual disorders and dysfunction have a profound impact on people’s perceived quality of life.
Sexual medicine is of the oldest medical specialties, though underresearched. Alfred Kinsey, also known as the father of human sexuality, was one among the first to publish scientific data on human sexual behavior, published in 1948. 3 Clinicians usually think that speaking about sexuality with their patients affects the rapport, but it is the other way around. Many patients when questioned about their sexual health would be more willing to discuss about the same. Health care professionals owing to a lack of time, knowledge, and training find it difficult to address sexual problems of their clients. Scientific bodies such as International Society of Sexual Medicine and European Society of Sexual Medicine are effectively assuming control over the reason and assisting various investigations and researches into this specific field. Taking into account the prevalence rates of female and male sexual dysfunction within the general population around 30% and 10%, 4 the need of great importance is to prepare more specialists to professionally practice sexual medicine.
The clinical practice of sexual medicine has undergone tremendous changes within the last 2 decades. Sexual medicine as a specialty is one of the most ignored areas both by profession and society, and thus, numerous informal practices win, which are misused by quacks. 5 The need for training in psychiatry and more specifically sexual medicine at undergraduate and postgraduate levels is well recognized and attempts are made to rectify the same. 6 In this article, we aim to depict our innovative and novel endeavor to establish psychosexual medicine facility as a different unit, in this tertiary care teaching hospital attached to a medical college, Mysuru, India, with the aim of providing comprehensive health care to patients with psychosexual problems. The opportunities that began and challenges we faced in this procedure of planning and establishment are expounded with the goal, so that similar initiatives can be stimulated and supported.
Methods
Setting
JSS Hospital is a tertiary care teaching hospital joined to a private university-based medical college situated in Mysuru, Karnataka, India. The clinical services of the hospital are utilized by patients not only from inside the state but also from the neighboring states of Karnataka.
Initiation and Planning
For establishing a psychosexual medicine unit, planning, and close collaboration and teamwork between Departments of Psychiatry and Psychology along with hospital administrators is essential. Support from other allied medical, gynecological, and urosurgical specialties should also be included. Success in its execution requires efforts, money, and time; defined institutional objectives and goals; modifications of resources for supporting the new need; and coordination between various other departments. This stage included interactions with the Director of the hospital, Head of Clinical Services (Medical Superintendent), Head of Medical College (Principal), and heads of various other clinical departments. This phase also included developing the training curriculum; identifying and contacting potential team members and resource persons for the proposed training; developing a budget for the training; obtaining institutional approval for training; and starting a fellowship and certificate course in psychosexual medicine.
Operating Procedures
Standard operating procedures were developed by the team under the guidance of a senior consultant psychiatrist, which included frequency and structure of the Outpatient Division (OPD), content, and duration of interdisciplinary academic programs, clinical care pathways, and activities geared toward sexual health promotion and fostering team spirit among team members.
Implementation and Background of the Clinic
Psychosexual Medicine Clinic was formally inaugurated by Dr Raj Bramhabhat from Mumbai in the year 1997, as a separate unit, and OPD services were delivered to the clients who had psychosexual problems. The idea to implement and establish an academic psychosexual medicine facility as a separate unit in the Department of Psychiatry of a private university-based tertiary care teaching hospital attached to a medical college was conceived in 2016. The hospital has all clinical and diagnostic departments working inside its own premises. Without any prior appointment, any patient can just walk in and benefit from all the medical services. The psychiatry department has decent consultation and association services and gets a reasonable patient influx from different clinical specialties and communities. Before the establishment of the unit, letters/circulars were sent to every single clinical department sharpening them to its tendency and extension to guarantee brief referrals and their collaboration and cooperation.
Results
The key deliverable, a Psychosexual Medicine Unit as a separate clinic in the OPD of Psychiatry at JSS Medical College & Hospital, was achieved with the following structure and functions:
Structure of the Unit
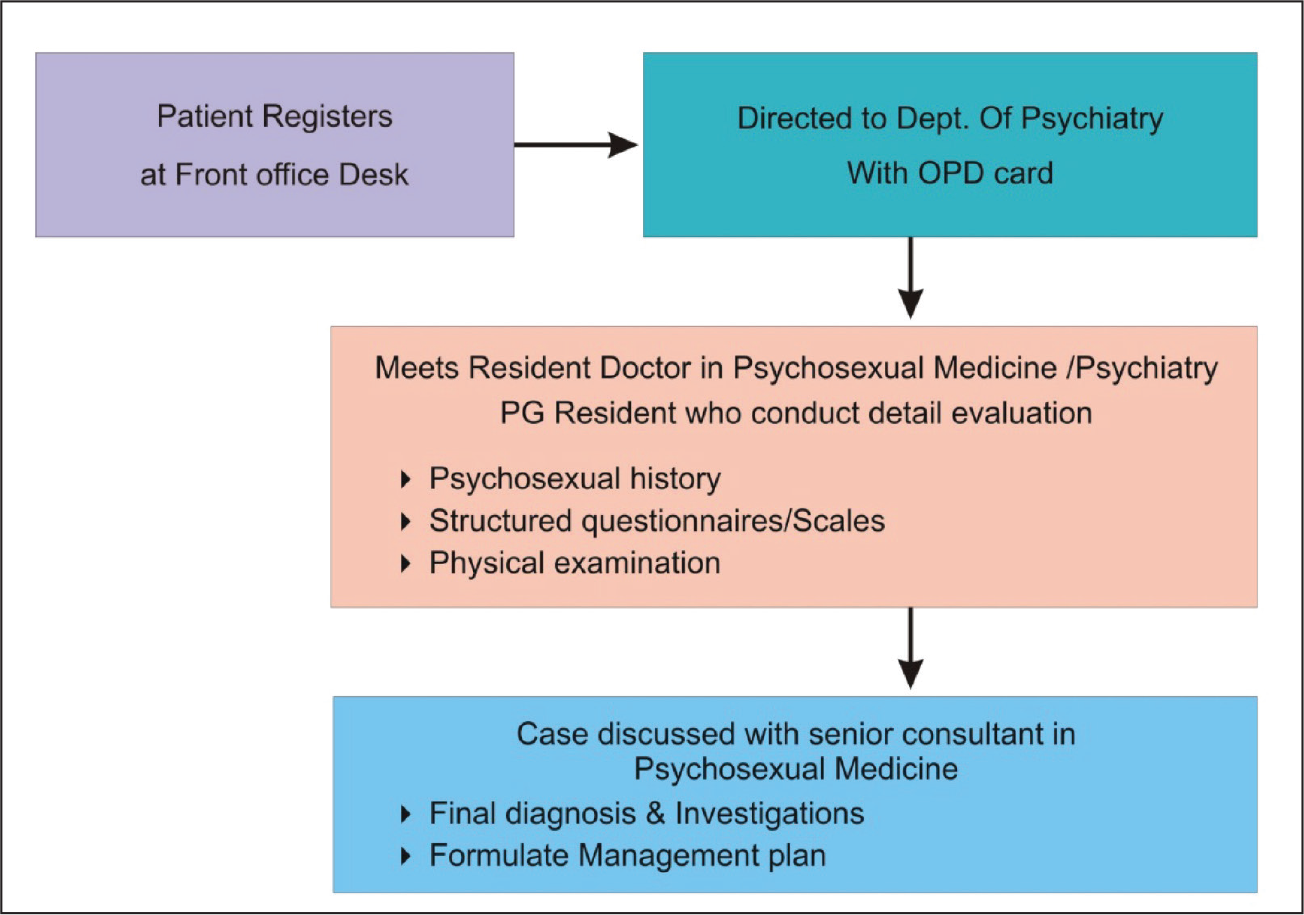
For feasibility reasons, the psychosexual medicine clinic is setup in the division of psychiatry OPD. The process flow is depicted in Figure 1. It was planned as a triweekly clinic, committed to a thorough and comprehensive evaluation of new cases, and the other day for follow-up of the old cases. The clinic is staffed with a senior consultant psychiatrist, an assistant professor, postgraduate trainees and internees on rotation basis along with a team of clinical psychologists, and medicosocial workers. The functioning of the clinic was supervised by a senior consultant psychiatrist who discusses case workups. The postgraduate residents do case workups that include detailed assessments, applying scales pertinent to sexual medicine in both outpatient and inpatient basis. The classificatory system which is usually followed is International Classification of Diseases, Tenth Revision, Clinical Descriptions and Diagnostic Guidelines and whenever necessary Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition). 7, 8 Clinical psychologists provide structured psychosexual interventions for cases and attend to psychosocial issues if any (Figure 1).
Assessment and Management
A thorough sexual history (both past and current) and assessment of general health and other sexual problems (if any) should be an integral part in sexual health assessment. Assessment included upbringing of the individual, finding out about any childhood sexual trauma, knowledge and attitude about sexuality, and cultural attitudes specific to the individual or couple. It also included medical comorbidities, such as diabetes mellitus, hypertension, cardiac diseases, vascular problems, autoimmune disorders, and psychiatric comorbidities, such as stress and anxiety disorders, mood disorders, psychosis, and history of chronic use of medications which impair sexual functioning.
The patients presenting to psychosexual medicine unit are screened by a consultant or fellowship resident and further in detail evaluation is done by employing a questionnaire in the structured pro forma covering sociodemographic details and clinical history. Structured instruments such as International index of erectile functioning (IEF), Arizona sexual experience scale (ASEX), Female Sexual Functioning Index (FSFI), and other relevant scales were also utilized. 9 Various parameters such as illustrative models of illness, clinical care pathways, psychological morbidity, social support, coping, and quality of life were assessed. Pathways of care were documented using pro forma plotted with structured questionnaire to discover the order of clinical specialties accessed prior to the evaluation. Consultants also conduct a thorough clinical examination of the patient and any structural or organic causes diagnosed are managed by liaising with other departments.
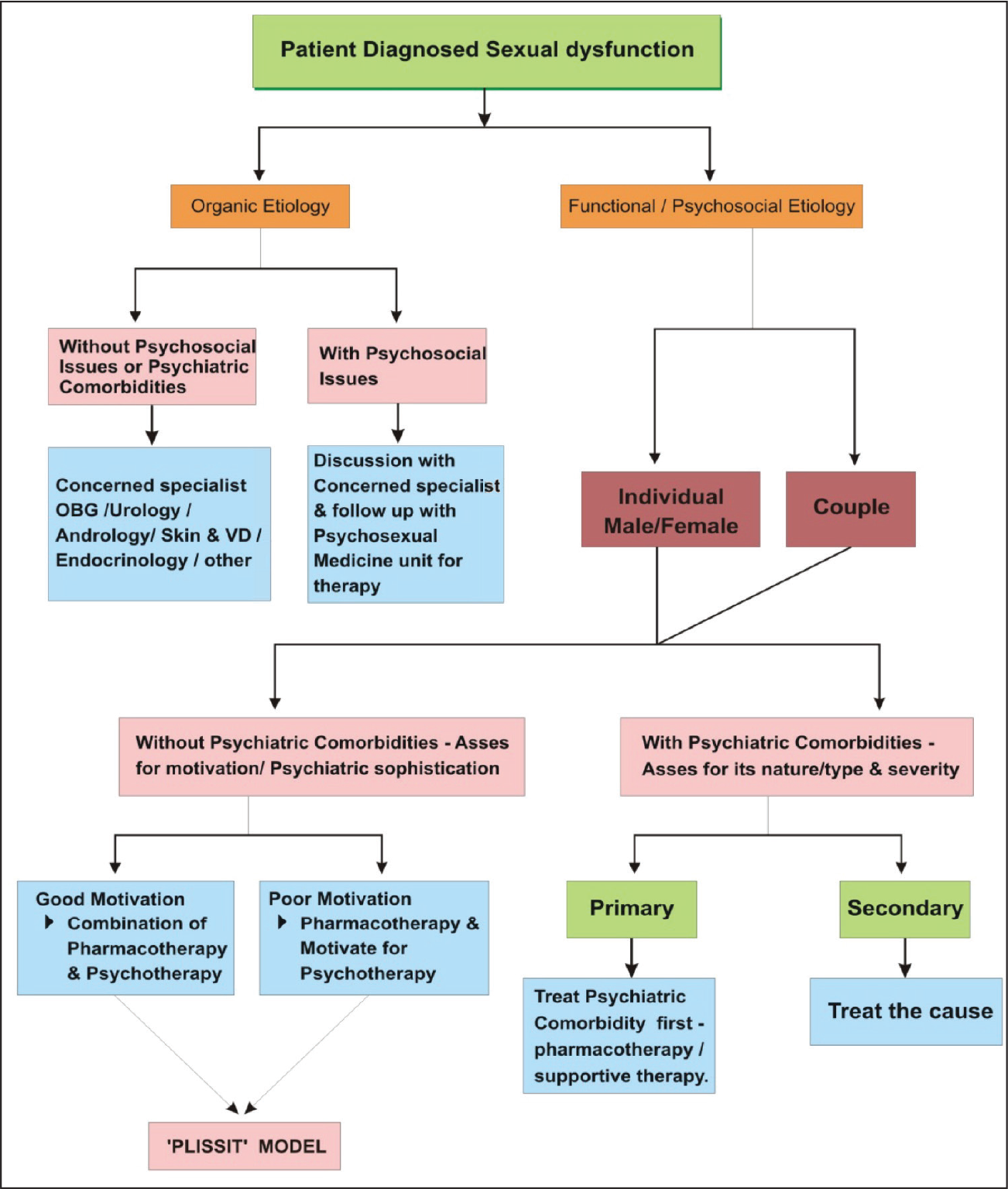
The usual evaluation time for each individual patient is 45 min approximately. After each patient’s detailed clinical appraisal, the patient’s case workups are discussed with the consultant expert, following which a provisional/final diagnosis is allocated to the case based on International Classification of Diseases, Tenth Revision, system and a treatment plan is drawn up. Patient care included interventions in the form of psychotherapy and pharmacotherapy. Residents of psychiatry medicine and clinical psychologists were responsible for delivering psychotherapy to patients. Follow-ups on regular basis were encouraged and advised for the patients as necessary, to remain within the treatment loop. During the whole clinical course of assessment and management, absolute confidentiality and privacy were maintained and assured (Figure 2).
Outpatient Services
The floor plan agreed on by the team included reserving some of the side rooms in the psychiatric unit for outpatient services. This arrangement is convenient for us to provide outpatient care on nonclinic days and also considering the limited manpower that is currently available.
Academic Platforms
The unit provides training, education, and research in psychosexual medicine. This includes study days, short introductory courses, and long-run seminar training. The fundamental objective of the training and education programs in sexual medicine is to sensitize the clinical experts to sexuality issues and make them comfortable with such issues both professionally and personally, equipping them to take an initiative among themselves in effectively managing the patients with sexual medical problems with a degree of solace.
Fellowship and Certificate Course Training Program in Psychosexual Medicine
Fellowship training in psychosexual medicine is designed to equip the clinical training with both theoretical knowledge and practical skills. The 1-year fellowship training is open to any doctor holding MBBS or MD degrees and 6 months certificate course to the students who have completed postgraduate training in clinical psychology and behavioral sciences, or medical graduates who wish to have a deeper understanding of human sexuality and sexual problems. The university provides formal training through case-based discussions led by the consultant in the form of case conferences, seminars, and journal club meetings. The case conferences listen to reveals on and understands the work of each student by academicians in a single doctor–patient interaction. A detailed study of the consultation and analysis of the doctor–patient relationship is made during group discussion. The students are also exposed to the interdisciplinary approach by rotational postings. The training classes, ie, both basic and clinical exposure, run for a duration of 1 year, following which the student clinician should be prepared with the skills to take up the fellowship or certificate examination and for awarding the completion certificates. The seminar topics as per the academic curriculum designed cover male and female sexual anatomy, sexual response cycle, cultural aspects of sexuality, various sexual disorders/dysfunctions, sex therapy, and pharmacotherapy. 10
Discussion
The phases of this project, ie, psychosexual medicine unit as a separate clinic, described in this article demonstrate that with institutional and administrative buy-in, it is possible to develop in-hospital psychosexual health care service in medical college settings.
We hope that hospital managers and leaders in psychiatric medicine in India will invest in providing access to specialized training in center of excellence in psychosexual medicine. The university invested and encouraged this author to start out educational program, and since then an initial team of 5 health care professionals was trained during this fellowship program. Replicating this or similar projects across the country would lead to a steadily increasing number of interdisciplinary health care workforces who have additional competencies in caring for such patients.
The project has been and is being built through multilevel, interdisciplinary support. The administration and management of the hospital and successive heads of the Department of Psychiatry and Department of Psychology are pivotal to the achievements till date.
The project took aloof from little beginnings with intra- and interdepartmental consultation services, outpatient services, and then the creation of psychosexual medicine clinic as a separate unit adjacent to the Department of Psychiatry. Interdisciplinary team training was followed with the implementation of the integrated holistic approach model of care. Academic programs also commenced and are ongoing for postgraduates of psychiatry, nursing, and for medical staff. Several conferences, continuing medical education programs (CME’s) at regional, state, national, and international levels specifically within the field of psychosexual medicine have taken place. Many short-term and future research projects are undertaken specific to sexual health. Research articles are published in indexed national and international journals.11-43
We have been mindful to document our policies, programs, and procedures. Critical reflections were an integral part of the daily activities for all participants during the interdisciplinary training and were documented. Case summaries were prepared by consultants and postgraduate residents during the training period. We regularly discuss with these notes as a reminder of our team goals and of the processes through which we collectively determine to attain those goals. We have also regularly presented interesting cases in our academic society meetings. This publication is in furtherance of our commitment to document and shares our experiences with a wider audience. Our assessment and management procedures and outcomes are being evaluated. Clinical audits are ongoing, the findings of which are able to be shared in other publications.
Feedback to team members and to the management staff of the hospital, and other relevant stakeholders has provided the premise for program adjustments, infrastructural improvements, and for securing additional resources for the unit. Feedback are ongoing, but we have presented this text with the hope that policymakers and consultant psychiatrists will find the impetus to ascertain specialized in-hospital services to cater for the needs of a population that requires care and treatment to boost psychosexual health.
Difficulties that were experienced in establishing and running the psychosexual medicine facility included, firstly, the poor referral rates and, secondly, persuading patients regarding the adequacy of psychological interventions for his or her problems. Thirdly, according to locally predominant social convictions and works on, living up to expectations of a patient’s desires. Fourthly, teaching modules being prepared for the training of the students and other health care providers, stressing on management approaches toward patients with sexual health disorders, models of communication to reduce stigma within the community for a health-seeking behavior. At present, supporting the adequacy of psychosexual measures has been found to be challenging with regards to the above-mentioned hurdles and barriers.
The unit gives chances for focused training of clinicians to deal with individuals and couples suffering from sexual problems. The residents of psychiatric medicine and clinicians practicing can get wider exposure to the various clinical presentations and treatment approaches used. Lastly, such a specialty and ardent clinic may produce better and diverse opportunities for research in the field of sexual health and medicine, and sexual disorders.
Limitations
The Psychosexual Medicine unit established here adheres only to our institution.
Other hospitals and health care organizations can adapt this layout and plan, after careful modifications as per their resource availability, size of the hospital, levels of care, patient load, etc.
Conclusion
By investing in improving infrastructure and available human resources, the specialty psychosexual medicine unit was established. By sensitizing various clinical specialties about psychosexual medicine in the hospital, hesitancy among the clinicians enquiring about sexual health has decreased significantly. Apart from this, clinicians are now more aware about drugs causing sexual dysfunction and they have started choosing appropriate drugs. The Psychosexual Medicine Unit not only gave chances for a more comprehensive assessment of individuals with sexual disorders but also improved training and education for residents with focused interdisciplinary research in the field of sexual medicine. It portrays a versatile model of care that can be utilized for establishing such specialty clinic in hospital/medical college settings of similar types.
Proposed Areas for Future Research
Psychosexual Medicine Clinic OPD Utilization rates.
To research on the prevalence of various comorbidities among patients presenting to psychosexual medicine unit.
Economic evaluation of clinical care services of psychosexual Medicine.
Integration of telemedicine technology into the clinical practice of psychosexual medicine.
To study the impact of various medications causing impairment of sexual functioning.
To prepare a master health checkup model with established Standard Operating Procedures.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.