
Abstract
Abstract
Although sexuality has a long history in the Indian literature, it is not discussed openly due to various reasons. Although sexual medicine has seen a reasonable growth in the last 70 years, somehow, psychological factors associated with the development of various sexual dysfunctions have not received due importance. Cultural factors which contribute to development and persistence of sexual disorders have not been evaluated properly. In terms of training, there is a wide variation across different centers in this country. There are very few indigenously designed instruments for the assessment of sexual disorders and there is limited data on well-evaluated indigenously designed interventions for the management of various sexual disorders. There is a need to homogenize the training and liaise with other specialists working in this area. Centers with well-developed services for sexual disorders need to start observerships and postdoctoral fellowship programs to train the interested clinicians. There is a need for multicentric studies to generate national-level data.
Introduction
Sexuality has a long history in the traditional Indian literature. Descriptions giving importance to male sexual potency and functioning can be traced back to the Vedas. One of the oldest Ayurvedic texts Charaka Samhita, which was written by Agnivesa (1000 bc), refers to many sexual disorders in males. These descriptions include terms like Sukrameha (spermaturia, currently understood as Dhat syndrome), Apraharsana (lack of or less libido), and Dhwajabhanga (lack of or less erection). These texts also provide information about the etiological causes of sexual dysfunction, for example, erectile dysfunction is further classified as vijopaghataja (disorders of androgens), dhwajabhanga (penile diseases or trauma), jarajanya (due to old age), and sukraksayaja (consumption of semen). These descriptions have also provided information about the remedial measures for various sexual problems. 1 These old traditions still continue to influence the manifestation of various sexual disorders among general population.
When one looks at the prevalence of sexual dysfunctions in the general population, these have been reported to be highly prevalent. However, these infrequently receive clinical attention. These are associated with significant distress and can have negative impact on the day-to-day functioning of the patient. Considering that these are highly private matters, patients are often hesitant to discuss this with the clinicians. Clinicians are also often uncomfortable in inquiring about these matters and whenever these are brought up by the patients, clinicians often themselves become uncomfortable to discuss these matters. Hence, a great deal of skills is required to assess and address these issues. 2
In modern psychiatry practice, having a good understanding about sexuality, psychosexual disorders, and marital/couple interaction is of paramount importance. With increasing stress and lack of acceptance of each other, there is increase in the relationship’s issues ending up into the clinics. With more and more research in the area of sexuality, it is now understood that in a small proportion of patients, sexual dysfunctions are purely organic, and psychological factors do contribute to the manifestation and treatment response. Hence, having an understanding about the psychological factors associated with sexual dysfunction helps in providing care to patients who not only have purely psychological sexual dysfunction but also have sexual dysfunction associated with organic causation.3, 4 Further, with increasing the use of psychotropic medications for various psychiatric ailments, clinicians often encounter sexual side effects. Hence, clinicians often face the dilemma of how to manage primary psychiatric illness in the face of sexual side effects, as these are associated with significant distress, poor functioning, and poor medication compliance. 5
A good understanding of sexual functioning and dysfunctions can enhance the clinical skills of a mental health professional. When one looks at the progress of sexual medicine from mental health professional’s perspective, since the 1960s many mental health professionals have shown keen interest in the area of psychosexual disorders. Sustained interest in this area by a group of clinicians and researchers has helped in recognizing this as a subspecialty of psychiatry. Indian Psychiatric Society (IPS) has a subspecialty section of sexual disorders. This development has led to a sustained interest of clinicians, academicians, and researchers in this area. Somehow this recognition has also helped in a great deal, in giving importance to sexual disorders in various scientific meetings, conferences, and continuing medical education (CME) programs.
What Has Been Achieved till Now?
When one looks at the progress done in the area of sexual disorders in the last 7 decades in this country, it can be understood from the perspective of clinical services, training, and research. If one looks from the perspective of clinicians, as early as 1960, N. N. Wig gave the concept of “Dhat syndrome” to describe the cultural phenomenon of preoccupation with the loss of semen in the Indian subcontinent. 6 Soon the same phenomenon was acknowledged in other Asian and European countries. Since this beginning, a lot of research has been done in the area of Dhat syndrome in this country.2, 7 These sustained efforts of researchers led to the inclusion of Dhat syndrome as a neurotic disorder (coded as F48.8) and in the Annex 2 (culture-specific disorders) of International Classification of Diseases, Tenth Revision, Diagnostic Criteria for Research caused by “undue concern about the debilitating effects of the passage of semen.”8, 9
A large number of studies on Dhat syndrome have come up in the last decade, including the development of a questionnaire for its assessment and a multicentric study on its clinical presentation.10-12 Later, clinicians also made similar observations in among females, by equating symptoms of vaginal discharge in females with Dhat syndrome in males. 13 Over the years, clinicians and researchers have furthered this area and recently a specific instrument was developed to assess “female Dhat syndrome,” and diagnostic criteria for the same were proposed.14, 15 Occasional reports have been presented about the intervention, and a cognitive behavioral model of treatment has also been developed and tested for males affected with dhat syndrome, which comprises of assessment, psychoeducation, and cognitive behavioral interventions. 16
In terms of other sexual problems, research in the area of psychosexual disorders was slow to start with. Initial reports focused on the prevalence of sexual dysfunction in male patients attending the psychiatry outpatient services.17-22 Depending on the study site, these studies have shown that erectile dysfunction and premature ejaculation are the most common sexual dysfunctions seen in psychiatry outpatients. 23 Some of the studies have also evaluated the sexual problems among female patients.24-25 In recent times, many studies from India have also focused on the sexual side effects associated with various psychotropic medications such as antipsychotics, 26 antidepressants, 27 and mood stabilizers like lithium. 5 Studies have also evaluated the prevalence of sexual dysfunction among patients who are using various substances and are treated for the same.28-31
In terms of clinical practice, at many centers, clinicians have set up a formal marital and psychosexual clinic or psychosexual clinics. At the Post Graduate Institute of Medical Education & Research, Chandigarh, a marital and psychosexual clinic was started in 1987. 32 Vibrant psychosexual clinics have been described at many places in the country with some of the clinicians specializing only in this area. At few places, like at JSS Medical College, Mysuru, the interested clinicians have set up a laboratory for the assessment and management of patients presenting with psychosexual disorders. These clinics have led to the structured assessment of patients presenting with marital and sexual problems and have given opportunities to teaching, training, and carrying-out research. These clinics have also helped in establishing close liaison with other specialists, such as endocrinologists, urologists, gynecologists, etc. A clinical scenario has changed significantly from no pharmacological treatments for sexual disorders to whole range of pharmacological agents available to address the issues of sexual dysfunction. The emergence of drugs like sildenafil has improved the overall outcome of interventions. The use of combinations of pharmacological and nonpharmacological agents has led to better treatment outcomes.
At the organization level, besides having specialty section of sexual disorders, IPS came up with clinical practice guidelines for the management of various sexual dysfunctions in 2006, which was recently revised in 2017.3, 4 In terms of leadership, psychiatrists from India have been recognized by the World Psychiatric Association and other international organizations in this subspecialty for their contribution in the field.
All these sustained efforts have established sexuality as a subspecialty section of psychiatry, and more and more psychiatrists of the newer generation are making efforts to set up psychosexual clinics at their centers and have carried on with research in this area.
Barriers in the Progress
It is a well-known fact that India as a country is very deficient in the trained mental health professionals. Due to this, training at most of the centers focuses on the management of major and minor mental disorders. Due to this, practice and development in the field of psychosexual disorders are very much dependent on the zeal of the clinicians interested in this area. This has led to lack of sustained growth in the specialty. Exact information is not available in terms of how many training centers in this country have dedicated mental health professionals and dedicated clinics addressing the psychosexual ailments. Although, there have been many research efforts in the area of psychosexual disorders, most of this research emanates from the personal efforts of the researchers, with no or very less funding from any government agency, as these disorders do not fall in the priority area of the government. In terms of professional leadership, barring a handful of psychiatrists, minimal efforts have been shown by others in the profession. Although, the services have developed in the last few decades, clinicians have mostly relied on the developments made in other countries for practice in this area, with minimal or no efforts in developing indigenous methods of assessment and management. Some of the clinicians who have developed indigenous methods of assessment and management have not published the same. This has led to lack of dissemination of information to others.
One of the major barriers in the practice of sexual medicine in this country is the fact that most of the patients with these problems first seek professional help from others, ranging from traditional healers to other medical specialists. Somehow, mental health professionals have not been able to impress others on what we can contribute to the management of these patients. Due to this, somehow, the message that mental health professionals need to be consulted for these issues has not been percolated to the general public at large. Further, although the worldwide literature has now started acknowledging that almost all cases of sexual dysfunction have psychological contributions, mental health professionals in this country have not been able to form close liaison with other specialists working in this area. This has led to providing fragmented care to patients presenting with sexual disorders.
There have been some efforts in the last few years, but yet, mental health professionals have not been able to move beyond sexual disorders/dysfunctions to talk about sexual health. This has led to continuation of myths about sexual functioning, potency, and performance. There are no universal school sex education programs across the country. There is an urgent need for the mental health professionals to take a lead in this area to prevent the development of further sexual problems.
What Have We Learnt by Now?
It would be needless to say that in Indian culture, sexuality is of paramount importance. Data from different studies also suggest that various sexual problems are quite common among people in the general population, patients attending psychiatry outpatient clinics, and patients attending other special and general outpatient clinics. The presence of organic factors does not mean that mental health professionals have no role in the management. Data also suggest that patients with primary mental disorders like depression have higher prevalence of sexual problems, compared to persons in the community. In fact, decrease libido is understood as a symptom of depression. The use of psychotropic medicines is associated with higher rates of sexual dysfunction, which has negative consequences on the management of various primary psychiatric disorders. Overall, it can be said that the presence of sexual problems is associated with marked distress, impairment in functioning, relationship issues, and legal complications.
Keeping these facts in mind, it is very clear that mental health professionals have a major role to play in the assessment and management of patients with sexual problems. Hence, the training programs in this country need to give due importance to proper assessment and management of sexual problems.
The Road Ahead
Although a good beginning has been made in the last few decades, it is far from the need of the day in the field. In terms of research, although there are many clinical-based studies on prevalence of various psychiatric disorders, there is lack of data about the same among the community-based population at large. It is said that what is seen in the clinics is just the “tip of the iceberg.” 33 Accordingly, there is a need to conduct large community-based epidemiological studies to understand the extent of the problem, both in males and females. Further, there is a need to understand the influence of age, knowledge about sexual matters, attitude toward sex, various chronic physical illnesses, mental disorders, medications, and other medical interventions on the prevalence. This kind of research can only be possible with a good leadership and a good funding. Clinicians who have till now carried the flag must continue to lead in this area and carryout such landmark studies. In terms of clinic-based data, information is still far less on the prevalence of sexual problems among patients with various mental disorders. Due to lack of these data, clinicians often underestimate their existence and never inquire about the same routinely. Our understanding about how in the context of Indian culture, sexual problems contribute to the causation and maintenance of various psychiatric disorders is far too less. Hence, there is need for multicentric studies to improve the understanding of link between the sexual problems and primary mental disorders. The association of psychotropic and sexual dysfunction has received some attention in the recent times, but isolated small sample size studies have not answered all the questions. Clinicians are far too away from taking an informed decision about when to stop, reduce, or change the psychotropic medications. Well-designed multicentric studies can answer some of these questions.
Some indigenous instruments, such as sex knowledge and attitude questionnaire (SKAQ), comprehensive questionnaire for assessment of Dhat syndrome, and scale for assessment of female Dhat syndrome, have been designed in the last few years.10, 15, 34 However, clinicians have mostly relied on instruments designed in other parts of the world to assess and monitor their patients. Many of these questionnaires are redundant due to cultural incompatibility. The need to develop culturally orientated instruments is the need of the hour to carryout clinical assessment and research in the area of sexual behaviors and disorders.
Many clinicians have come up with manuals, having algorithms for sexual problems such as erectile dysfunction, premature ejaculations, Dhat syndrome, and homosexuality.35, 36 However, these have not been evaluated thoroughly in terms of the benefit to the patients, user-friendliness, and feasibility of use. In terms of management of various sexual disorders, nonpharmacological treatments play an important role. Although some of the researchers have evaluated the effectiveness of various nonpharmacological measures in the management of erectile dysfunction, premature ejaculation, and Dhat syndrome, these have been isolated efforts in a small number of patients, which precludes generalization. Most of these studies have been in the form of open label studies with no randomized controlled trial in this area from India. Research in this area is the need of the hour. Although the area of impact of sexual dysfunction on the spouse and relationship issue has also been evaluated in occasional studies,37, 38 a lot needs to be done in this area too.
With the advent of 5-phosphodiaesterase inhibitors, the management of sexual dysfunction, i.e., erectile dysfunction, has changed remarkably. Although this has brought significant relief to the patients in distress, it has also created problems in the practice. Now everyone is a specialist in the area, with the power to treat erectile dysfunction by prescribing sildenafil. Due to this, somehow the need to address the psychological factors has been underestimated and the new generation of psychiatrists has limited themselves to prescribing medications only. There is an urgent need to reverse this trend and the trainers should take up the responsibility of emphasizing the need for nonpharmacological treatments for management of various sexual disorders. Besides this, there is need for efficacy/effectiveness studies that can compare the nonpharmacological treatments, pharmacological treatments, and combination of both pharmacological and nonpharmacological treatments. Data from this kind of studies can not only help in formulation of evidence-based treatment guidelines and influence the clinical practice.
One of the major developments that has occurred in the last 2 decades or so in everyone’s life is reliance on technology. Computers, laptops, tablets, smartphones, etc. have become a necessary part of life, though these have led to new problems and also a few solutions. Easy accessibility and spending too much time on the internet and social media have affected the interaction patterns including sexual functioning. Easy access to pornography has changed the concept of sexuality and many a times this leads to unrealistic expectations from the partners. When the expectations are not met, interpersonal relationships see further downhill turn. At times, the use of pornography has also been reported to be an addiction. Often people turn up to the clinic with complaints of partners not interested in sex and busy on social media round the clock. However, these areas have remained untouched in terms of research, barring 1 or 2 isolated reports. There is a need to explore this area, as it is expected that the role of technology in the life of people is going to increase in the decades to come. Over the years, professional bodies have to come up with guidelines for the use of different technologies in order to reduce the deleterious effects of these on the human psyche, interpersonal relationships, and sexuality.
However, technology has also brought many solutions for the management of various sexual disorders. Technology can help in carrying out behavior therapy; can be used for carrying out cognitive behavior therapy, exposing desired sexual content, recording various parameters of interest while carrying out various pharmacological and nonpharmacological interventions, and creating virtual reality. Hence, the clinicians and researchers working in this field are expected to develop laboratories based on these technologies to answer some of the unanswered questions.
Technology can also be used to start online training programs and for the generation of videos for training and teaching purposes which the trainees can use to enhance their skills.
In terms of training, efforts should be made at all the training institutes to start the subspecialty of sexual medicine. Faculty members working in various departments need to assume the leadership role in starting these services. To start with, the clinics can be started as once-a-week services and depending on the patient burden the services can be expanded. Centers, with well-established sexual medicine clinics, must provide mentorship role in training interested faculty from other departments. In the same line, various institutes can tie-up to formulate faculty exchange programs or invite faculty from other departments for short duration for training purposes at their institutes. This will provide an opportunity to the young trainees to get trained by experts in the field. Here, organization like IPS can facilitate by providing travel fellowships to young faculty members to gain clinical experience.
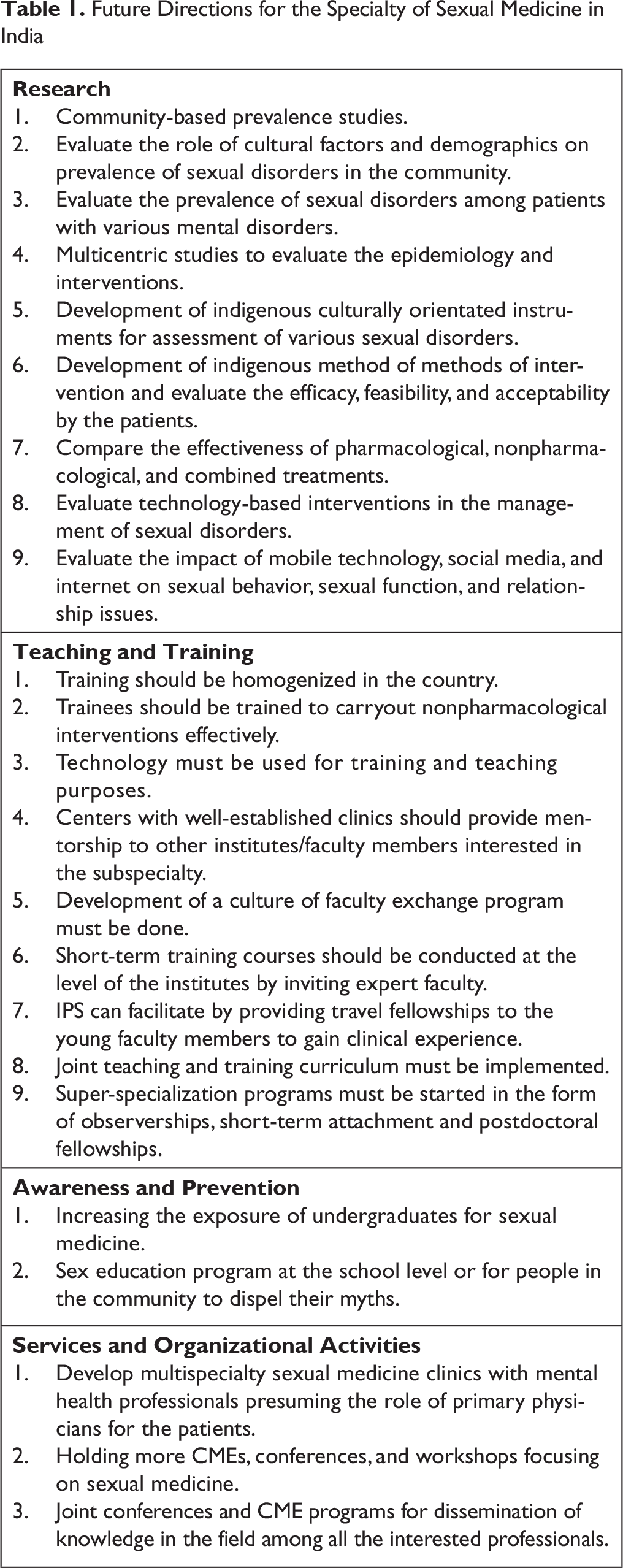
Centers, with well-established sexual medicines, can formulate a joint curriculum for training residents across the country to homogenize training programs which must emphasize case assessment, case formulation, how to elicit history about possible organic and psychological factors associated with sexual dysfunction, how to carryout investigations, formulating a treatment plan, and executing a treatment with emphasis on nonpharmacological treatments. Proper supervision needs to be provided to the trainees to harness their skills. Centers with well-established training programs and facilities should also come with super-specialization programs in the form of observerships, short-term attachment, and postdoctoral fellowships to provide opportunities to interested candidates (Table 1).
At present there is no exposure to the field of sexual medicine at the undergraduate level. On the similar line, there is lack of proper sex education program at the school level or for people in the community to dispel their myths. It is often noted that many sexual problems are fueled by the existing myths. Hence, there is a need to take up this issue with the appropriate administrative authorities to formulate such programs (Table 1).
Although there is some liaison between the mental health professionals and specialist from other disciplines such as endocrinology, urology, and gynecology, it is far too less. The mental health professionals should aspire to develop multispeciality sexual medicine clinics with mental health professionals presuming the role of primary physicians for the patients presenting with sexual problems, as they are well equipped in providing both pharmacological and nonpharmacological treatments and at the same time are capable of handling psychological distress and interpersonal issues arising due to the sexual dysfunction and ensuring hormonal and surgical interventions.
In terms of the organizational responsibility, IPS and other professional bodies should conduct more CMEs, conferences, and workshops focusing on sexual medicine. The present efforts of having sexual medicine as a subspecialty of IPS and updating of clinical practice guidelines must be continued (Table 1).
Future Directions for the Specialty of Sexual Medicine in India
Conclusions
Over the years, a significant progress has been made across the country by starting of psychosexual clinics in many teaching departments and at private centers. Research endeavors have provided some insights into the epidemiology of sexual disorders. Some training is available at various institutes in the field of sexual medicine. IPS has made major contributions by establishing sexual medicine subspecialty section and also formulating treatment guidelines for the management of sexual dysfunction. However, there is a long journey to follow. Sexual health of every individual has 2 facets, ie, mental and physical. Although the physical aspect is addressed by specialist from other specialties, they are largely ignorant about the psychological aspects and these are often neglected. This precludes providing holistic care and the patient is compartmentalized into various departments for the same problem. Mental health professionals need to stand up to the expectations of the patients and enable themselves to take the role of primary physicians in managing sexual problems.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.