
Abstract
Background:
Premature ejaculation (PE) is one of the most prevalent male sexual dysfunctions globally, with prevalence estimates ranging from 5% to 40%. Recent frameworks classify PE into clinical subtypes based on chronicity, situational factors, and clinical characteristics, including lifelong, acquired, natural variable, and premature-like ejaculatory dysfunction (PLED). Despite its psychological and relational impacts, research on these subtypes, particularly in the Indian context, remains limited, underscoring the need for further exploration to inform tailored interventions.
Methods:
This cross-sectional study assessed heterosexual men with PE at a tertiary center in North India. Individuals with significant psychiatric/medical comorbidities were excluded from the sample. A comprehensive evaluation of patients was done, including physical examination, hormonal/metabolic screenings, and assessments using validated tools for sexual dysfunction, psychiatric symptoms, and quality of life.
Results:
A total of 102 patients were enrolled in the study. Pairwise comparisons indicated significant differences in age of onset between lifelong premature ejaculation (LPE) and PLED (P = .001), as well as between LPE and acquired premature ejaculation (APE) (P < .001). APE was significantly correlated with tobacco dependence (P = .009). Patients with LPE generally scored lower across various domains of the SF-36 Health Questionnaire, indicating more significant functional impairment.
Conclusion:
APE emerged as the predominant subtype in the sample, followed by LPE—associated with a younger age—and PLED.
Keywords
Clinical subtypes of PE might appear similar in clinical settings, though important distinctions exist among them. Acquired PE is the most prevalent subtype in the Indian clinical context, with notable variations observed regarding tobacco use, age-related patterns, and illness severity across subtypes. Accurate subtype identification is crucial for guiding targeted interventions, which can be tailored to the specific characteristics of each subtype, ultimately enhancing patient outcomes.Key Messages:
Premature ejaculation (PE) is widely recognized as a prevalent sexual dysfunction among men. Studies have identified it as the most common sexual disorder across various demographics, especially among Asian, Central and Southern American, and non-European Western populations.1,2 Reported prevalence estimates for PE range broadly from 5% to 40%, reflecting shifts in diagnostic criteria and definitions. 3 However, with the standardization of definitions and the expansion of global research, our understanding of PE’s prevalence and contributing factors has improved significantly.
The classification of PE has significantly evolved over the past two decades. Although the concept of PE subtypes is not new—Schapiro first suggested categorizing PE into “Type B” (primary) and “Type A” (secondary) in 1943—the current framework, including distinctions based on chronicity and situational factors, reflects advances in understanding. 4 The DSM-5 divides PE into lifelong (LPE) and acquired (APE) forms, while recent research by Waldinger and Schweitzer introduced two additional clinical subtypes: Natural Variable PE (NVPE) and Premature-like Ejaculatory Dysfunction (PLED).5,6
Despite these advances, the psychological and relational distress associated with PE, often leading to psychological and psychiatric comorbidities, remains a largely under-explored area. 7 Additionally, the personal nature of sexual dysfunctions often results in shame and inhibitions, which prohibits men from openly discussing their symptoms. This has historically contributed to variable reporting and delayed the development of effective therapies. 8
The clinical subtyping of PE into four syndromes illustrates a spectrum ranging from those with a predominantly neurobiological basis to those with a more significant psychological influence.6,9 While Waldinger and Schweitzer’s PE clinical subtypes have been identified, they remain under-researched, particularly within the Indian population, where data is limited. Our study specifically aims to address this gap by exploring the prevalence and differences in clinical characteristics of these subtypes in the Indian context.
Methods
This cross-sectional study was conducted over one year (September 2017 to August 2018) at a tertiary care center in North India. The Institutional Ethics Committee approved the study, and ethical principles outlined in the Declaration of Helsinki were adhered to throughout. The study findings are reported per the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. The STROBE checklist has been uploaded as supplementary online material.
Participants were males presenting with complaints of PE at the Marital and Psychosexual Outpatient Department of Psychiatry on designated clinic days. Out of 148 individuals screened, 101 were enrolled. Co-morbid psychiatric illnesses requiring priority treatment were ruled out using the Mini International Neuropsychiatric Interview (MINI) v7.0.2. 10 Socio-demographic details, including gender, age, marital status, employment, and education, were collected (Figure 1).
Eligible participants were heterosexual men aged 18 or older who had engaged in intercourse within the last six months. Exclusion criteria included acute intoxication or withdrawal from psychoactive substances, organic mental disorders, psychotic disorders, intellectual disabilities, significant psychiatric, or medical comorbidities needing immediate treatment, and medications affecting sexual function and patients unable to complete investigations.
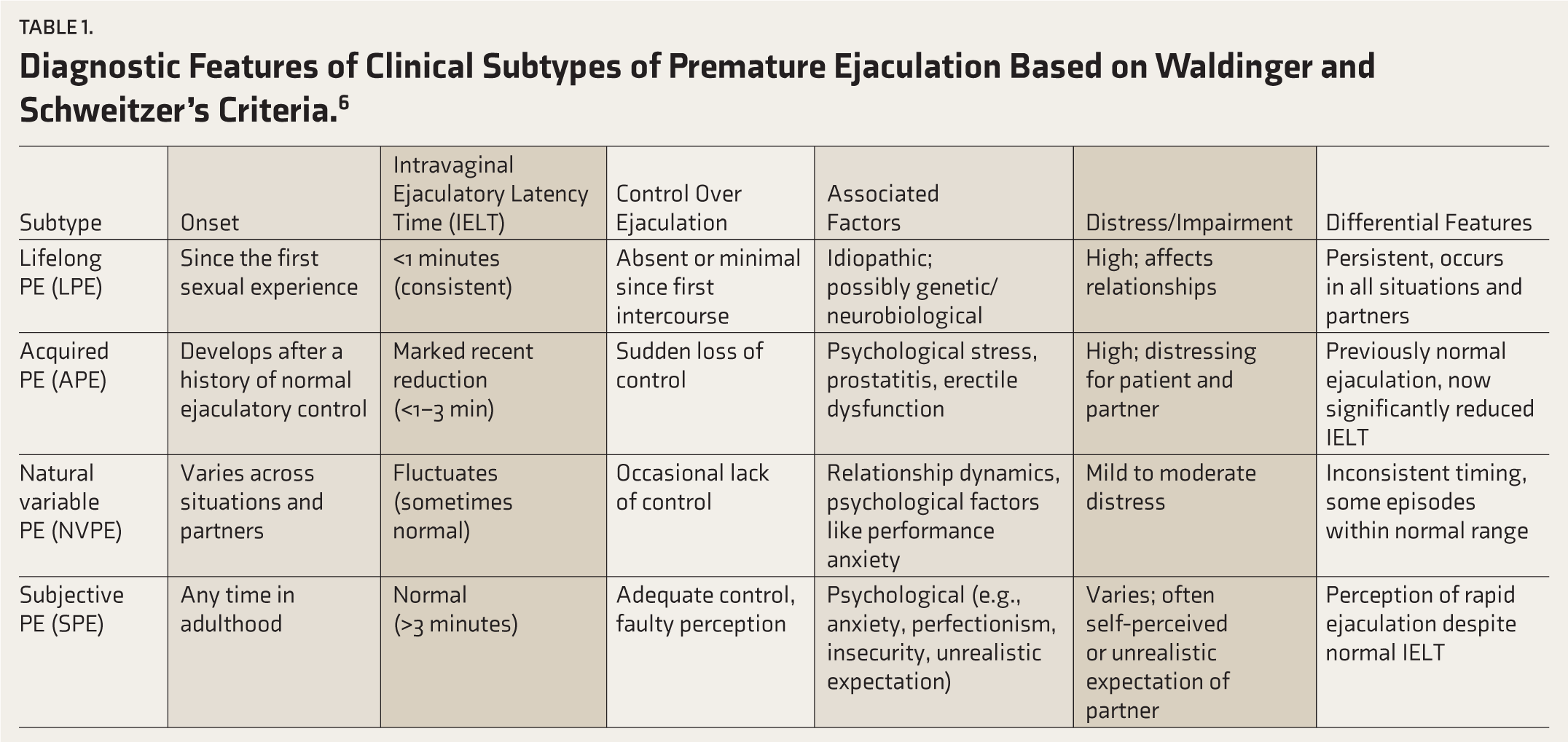
All participants provided written informed consent. A trainee psychiatric resident conducted assessments under a consultant psychiatrist’s supervision. Physical examinations, including genital and, when indicated, rectal assessments, were performed. Metabolic syndrome markers (blood pressure, lipid profile, blood sugar, BMI), serum testosterone, thyroid function tests, hemogram, and urine analyses were conducted in routine care. PE subtypes were classified based on Waldinger and Schweitzer’s framework using the PE Diagnostic Tool, while sexual dysfunction was assessed using the Arizona Sexual Experience Scale.11,12 As per Waldinger and Schweitzer, PE can be classified into four clinical subtypes based on a detailed sexual history, psychiatric evaluation, psychosocial and relational assessment, as well as medical assessment. Table 1 summarizes the most important characteristics of the clinical subtypes.
Additionally, the Hamilton Rating Scales for Depression (HAM-D) and Anxiety (HAM-A) measured the severity of depression and anxiety, respectively, and the Sexual Health Inventory for Men (SHIM) evaluated erectile dysfunction.13–15 The SF-36 Health Questionnaire was also administered to assess health-related quality of life. 16
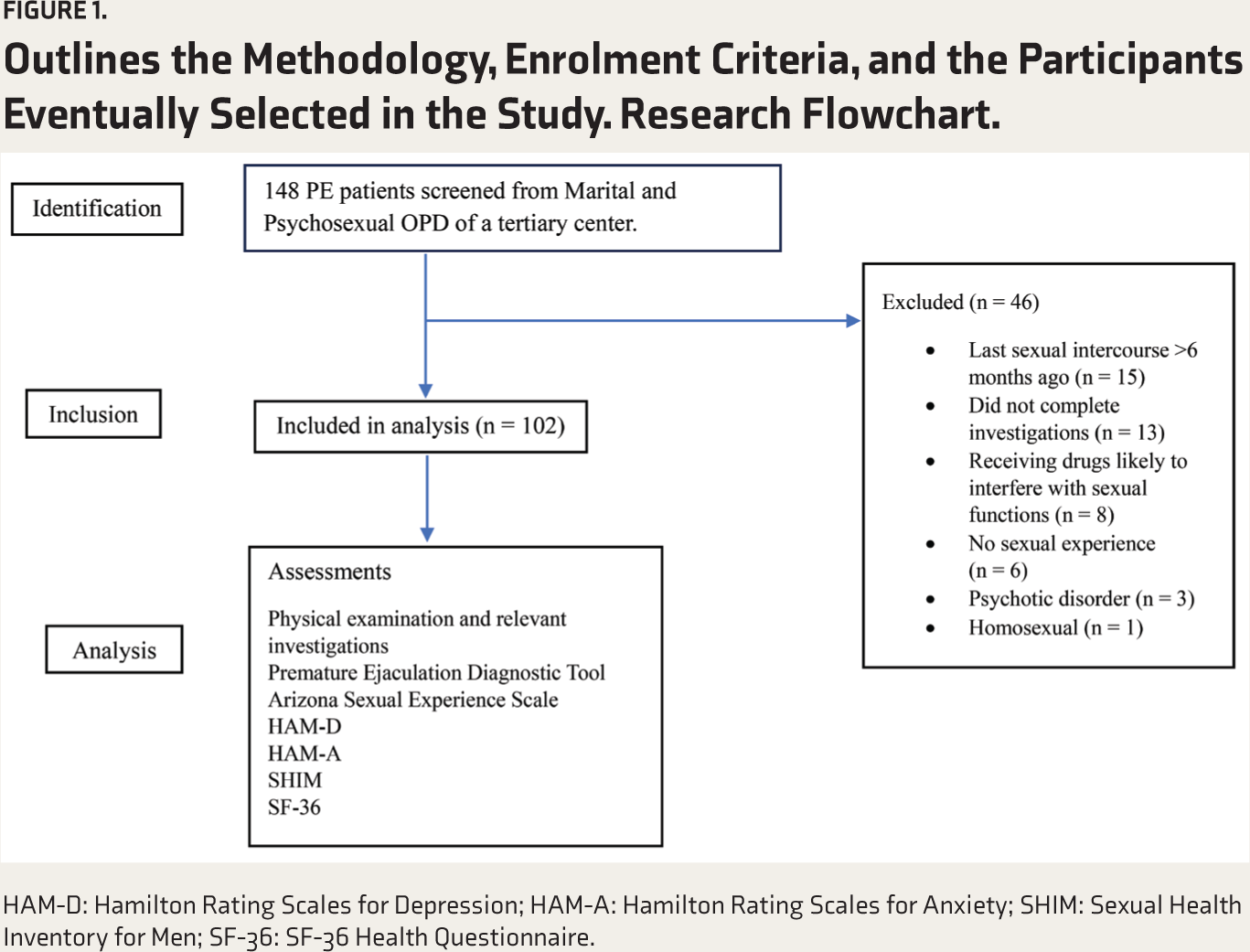
HAM-D: Hamilton Rating Scales for Depression; HAM-A: Hamilton Rating Scales for Anxiety; SHIM: Sexual Health Inventory for Men; SF-36: SF-36 Health Questionnaire.
Diagnostic Features of Clinical Subtypes of Premature Ejaculation Based on Waldinger and Schweitzer’s Criteria. 6
Data were entered into a Microsoft Excel spreadsheet (Microsoft Corporation, Redmond, WA, USA). Descriptive statistics were used to calculate means, standard deviations, and frequencies. The Shapiro–Wilk test assessed the normality of data distribution, and the data was non-normally distributed. The Kruskal–Wallis H test was used for continuous variables, while categorical variables were compared using Fisher’s exact test and the Chi-square test where applicable. Statistical analysis was conducted using SPSS version 25. 17 These analyses facilitated comparisons among socio-demographic and clinical groups across PE subtypes.
Results
A total of 148 patients were screened, with 102 ultimately enrolled in the study. The most common reason for exclusion was the patient’s last sexual intercourse occurring more than six months prior to the study (n = 15), followed by incomplete investigations (n = 13). Additional exclusion reasons included current use of medications likely to interfere with sexual function (n = 8), lack of sexual experience (n = 6), presence of a psychotic disorder (n = 3), and homosexuality (n = 1). Only one patient met the criteria for NVPE; due to the small sample size, data from this patient were excluded from comparative analyses. Table 2 presents the socio-demographic profile of enrolled patients. Pairwise comparisons indicated significant differences in age of onset between lifelong premature ejaculation (LPE) and PLED (P = .001), as well as between LPE and acquired premature ejaculation (APE) (P < .001). Regarding substance use, tobacco dependence was significantly more common among patients with APE than those with LPE (P = .009), with 22 patients in the APE group reporting tobacco use. Other clinical variables—such as duration of illness, body mass index, exercise habits, intercourse frequency, and severity of PE—did not show significant differences between groups.
Comparison of Sociodemographic Profile of Different Clinical Subtypes of PME.
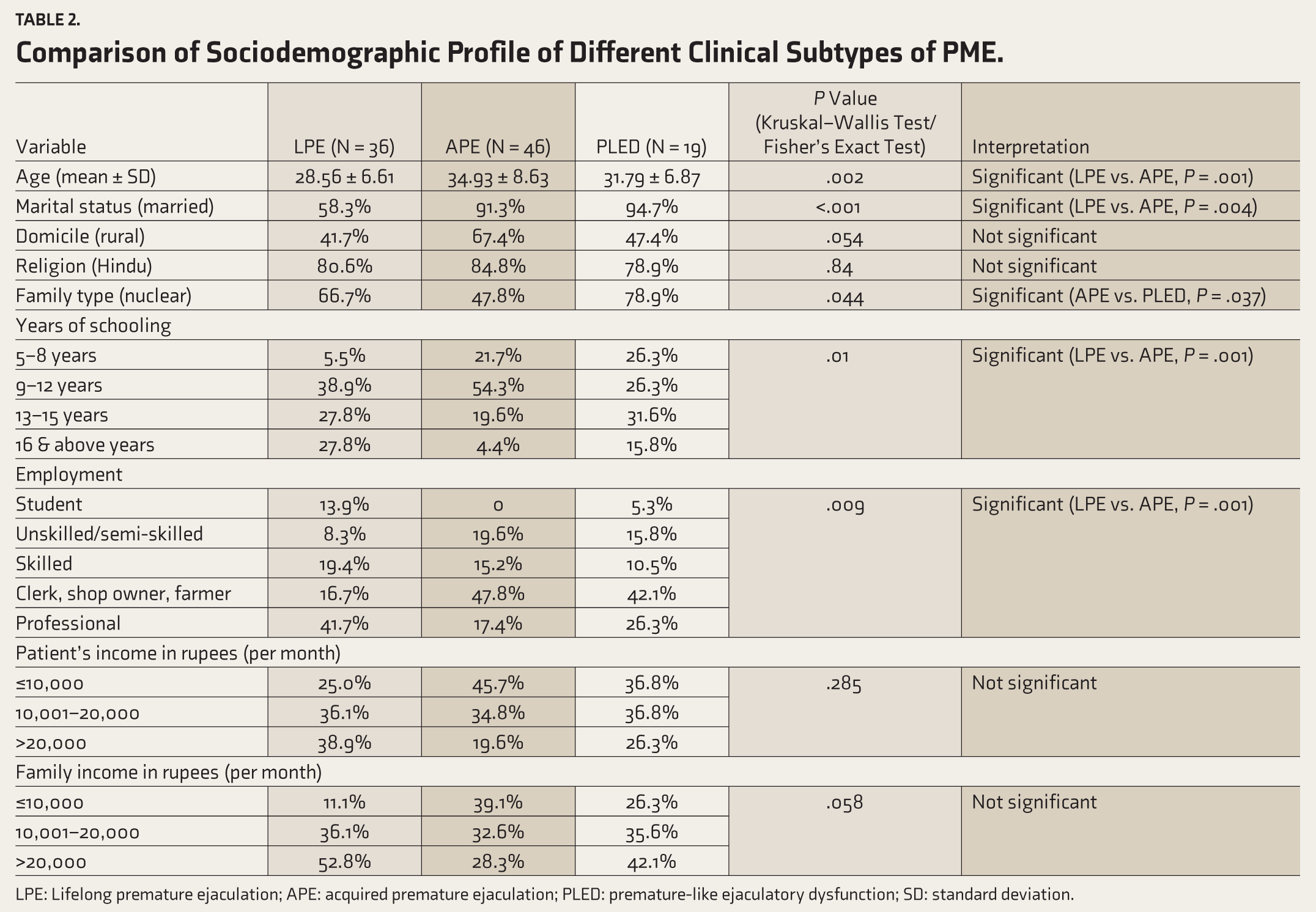
LPE: Lifelong premature ejaculation; APE: acquired premature ejaculation; PLED: premature-like ejaculatory dysfunction; SD: standard deviation.
The comparison of co-morbid sexual disorders, as well as erectile dysfunction and depressive symptoms among clinical subtypes, revealed no significance. The comparison of domains of the Arizona sexual experience scale showed that clinical subtypes had comparable scores with no significant findings. The distribution of co-morbid physical disorders among clinical subtypes was not significant. Table 3 compares scores of domains of health-related quality of life among clinical subtypes.
Comparison of Scores of Domains of Health-related Quality of Life Among Clinical Subtypes of PME.
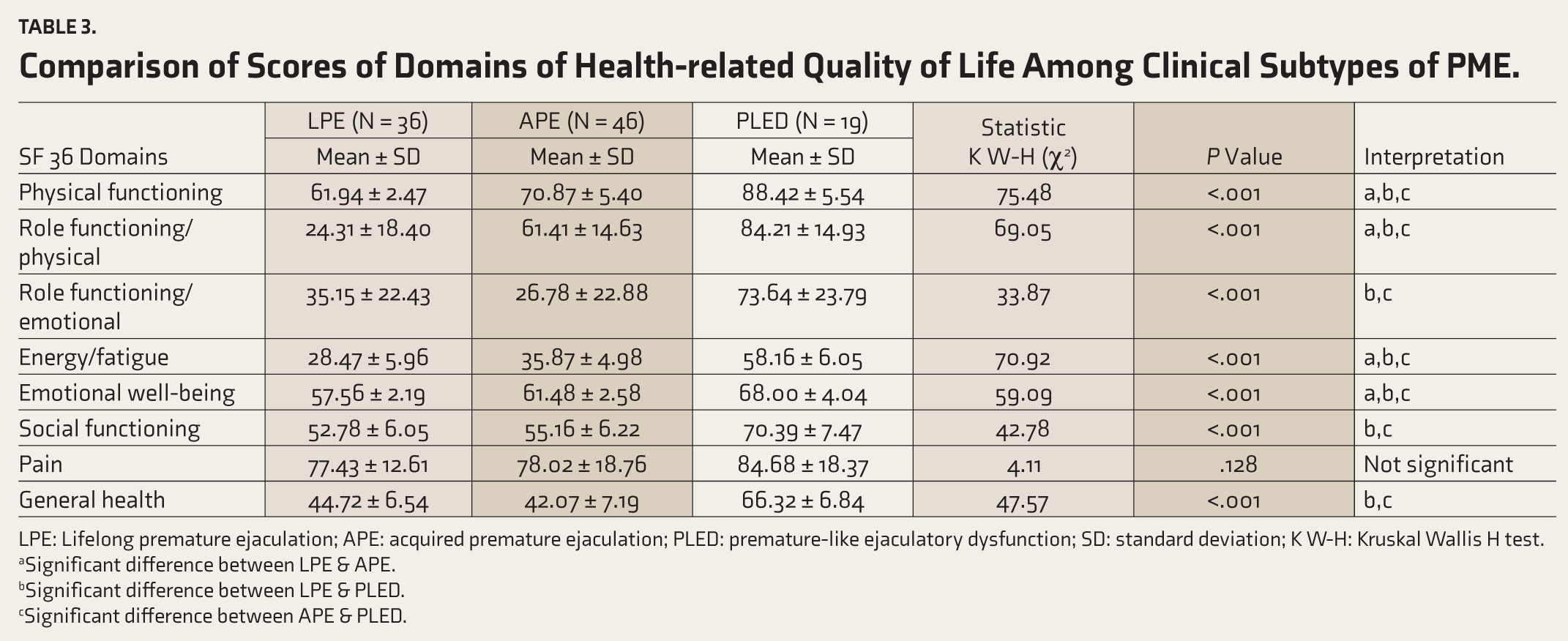
LPE: Lifelong premature ejaculation; APE: acquired premature ejaculation; PLED: premature-like ejaculatory dysfunction; SD: standard deviation; K W-H: Kruskal Wallis H test.
aSignificant difference between LPE & APE.
bSignificant difference between LPE & PLED.
cSignificant difference between APE & PLED.
Discussion
This study provides a cross-sectional analysis of patients presenting with PE at a specialty psychosexual outpatient department in a tertiary care center in Northern India. Our sample comprised individuals diagnosed with PE using the PEDT, who were further categorized into clinical subtypes according to Waldinger and Schweitzer’s criteria. Due to the limited representation of NVPE in our sample, the comparative analysis focused on the remaining three subtypes: LPE, APE, and PLED.
Our findings indicate that APE was the most common subtype (n = 46), followed by LPE (n = 36) and PLED (n = 19). This contrasts with previous community-based surveys, which identified NVPE and PLED as the most prevalent forms of PE.18,19 The discrepancy is likely due to the clinical nature of our sample; patients with more persistent or acquired forms of PE, such as LPE and APE, are more likely to seek treatment. Our results align with findings from a similar hospital-based retrospective study in India, which also reported LPE and APE as the more prevalent types in clinical settings. 20
Pairwise comparisons in age revealed significant differences between LPE and APE (P = .001). LPE patients were predominantly in the 18–30 age group, while APE patients were distributed nearly equally between the 18–30 and 31–40 age groups. This pattern may reflect the chronic nature of LPE, prompting individuals to seek treatment earlier than those with APE, whose symptoms tend to develop progressively.
Marital status comparisons also showed significant differences, with APE patients more likely to be married (P = .004), whereas LPE patients were distributed almost equally between married and single statuses. The later onset of APE may explain the higher likelihood of marriage in this group, as symptoms arise after individuals have established relationships.
In terms of age of onset, significant differences were observed between LPE and both PLED (P = .001) and APE (P < .001), with LPE having an earlier onset, often coinciding with the first sexual encounter. This earlier presentation may contribute to the increased distress associated with LPE, as affected individuals lack a reference for normal ejaculatory function. Additionally, tobacco dependence was notably higher in the APE group, potentially attributable to the older age distribution in APE and the development of substance use over time.
Analysis of ejaculatory function showed that LPE patients reported higher levels of ejaculatory dysfunction, which may be due to their limited experience with normal ejaculatory control, leading to greater perceived severity. In contrast, APE patients have typically experienced normal ejaculatory latency in the past, making the recent loss more psychologically impactful.
Comorbidities, both sexual and physical, were similarly distributed across subtypes, with no significant differences detected. This diverges from previous community-based studies that found comorbidities more prevalent in APE.18,19 The difference may stem from the clinical nature of our sample, which likely includes patients with more severe symptoms and those seeking help after extensive delays. These factors could influence the presentation of co-morbid conditions in tertiary care populations compared to general or community samples.
Regarding health-related quality of life, patients with LPE generally scored lower across various domains, indicating greater functional impairment, which is expected given their condition’s chronicity and early onset. The emotional well-being domain, however, was notably lower for APE patients, possibly due to the stress of marital and social expectations. Since APE often emerges in established relationships, these patients may experience greater psychological impact from PE’s effects on intimacy and relationship stability. Similarly, APE patients scored somewhat lower in the general health domain than LPE patients, though this difference was not statistically significant.
Earlier studies have shown PME to be frequently co-morbid with erectile dysfunction and depression.21,22 However, our study did not find significant differences in the severity of co-morbid sexual disorders, erectile dysfunction, depressive symptoms, or scores on the Arizona Sexual Experience Scale across subtypes. This may be attributed to the high severity of symptoms in our tertiary care sample and possible delays in seeking treatment, which may compound these clinical features. Patients with PE often delay seeking treatment due to stigma and may try alternative remedies first, which can exacerbate symptom severity and impact the likelihood of co-morbid conditions.
PE can have various underlying causes, which affect its pathophysiology, etiology, and treatment. According to Waldinger’s earlier descriptions, LPE was believed to have a strong neurobiological and genetic basis, typically needing only medication for treatment. APE, on the other hand, was attributed to medical issues (like prostatitis or thyroid problems) or psychological factors (such as relationship issues), warranting a combination of medication and psychotherapy. Normal variable PE was seen as a natural variation in ejaculation performance. At the same time, PLED was thought to stem mainly from psychological causes, best managed through reassurance and psychotherapy. 6 It is essential to highlight that although the clinical characteristics of various PE subtypes may look similar, accurately identifying each subtype has important clinical implications. Proper diagnosis of the specific subtype can guide more effective, targeted treatment strategies, as management approaches differ significantly depending on the underlying causes.
Limitations
The study was observational and had a small sample size, which reduced the strength of its findings and limited the ability to generalize the results. In this study, quality of life and sexual experiences, assessed through self-report measures, were evaluated using tools translated into Hindi, with assistance provided by the interviewer in understanding during administration. Future research should aim to incorporate standardized tools in local languages to assess health-related quality of life and sexual experiences.
Conclusion
This study highlights the predominance of APE, followed by LPE and PLED, in a clinical sample. Notably, significant age differences were found between LPE and APE, with LPE patients generally younger at presentation. Tobacco dependence was primarily associated with APE. No significant differences were observed in co-morbid sexual or physical disorders, depressive symptoms, or Arizona Sexual Experience Scale scores among subtypes. These findings offer insights into the demographic and clinical distinctions among PE clinical subtypes in patients seeking specialized care, which may inform targeted intervention strategies. It is also important to emphasize that while several clinical characteristics of PE subtypes appear similar in presentation, accurately distinguishing them holds significant clinical implications. The management strategies and anticipated outcomes vary substantially across subtypes, underscoring the need for precise diagnosis to guide tailored treatment approaches and improve therapeutic effectiveness.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Consent to Participate
A written informed consent was obtained from all subjects involved in the study.
Consent for Publication
Not applicable.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Considerations
This study was approved by the Institutional Ethical Committee of King George’s Medical University, Lucknow with letter no. 790/Ethics/R.Cell-18, Ref. code 89th ECM II-B Thesis/P54 on July 07, 2018.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Prior Presentations
This manuscript has not been previously published or presented elsewhere. It has not been distributed or shared on any preprint server, conference, or other scholarly collaboration networks.
Simultaneous Submission to Another Journal or Resource
The content is original and has not been submitted for publication in any other journal.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.