
Abstract
Background:
Narrow-Band imaging International Colorectal Endoscopic (NICE) could reduce histopathology study requirements in colorectal polyp evaluation. Local and regional studies are required to validate its utility.
Objectives:
To evaluate concordance between NICE classification and histopathology.
Design:
Prospective analytic study performed in the Hospital Universitario San Ignacio, Bogotá (Colombia) between 2021 and 2022.
Methods:
Concordance between NICE I, II and III classification and histopathology [Hyperplastic Polyp (HP), adenoma and deep submucosal invasive cancer (DSIC)] was evaluated using weighted kappa. Diagnostic performance was evaluated for NICE I–II versus NICE III for DSIC versus adenoma/HP. A subgroup analysis was performed for polyps ⩾10 mm and those located in the rectum, sigmoid, and left colon.
Results:
A total of 238 polyps from 135 patients were evaluated. Median age 67 years (IQR 58.5–74.5), 54.4% males. 23 (17.1%) had ⩾3 polyps. Of polyps, 52.1% were located on rectum, sigmoid and left colon. A total of 182 (76.5%) were <10 mm. NICE and histopathology evidenced a fair-moderate concordance (quadratic weighted kappa 0.36, linear weighted kappa 0.43). NICE classification (NICE I–II versus III) compared to histopathology (DSIC versus adenoma/HP) evidenced a sensitivity of 90.9% and specificity of 99.1%. For DSIC diagnosis specificity was ⩾95% on polyps ⩾10 mm and those left sided located.
Conclusion:
NICE and histopathology concordance is suboptimal. However, NICE III for DSIC diagnosis evidence good specificity. Therefore, NICE III polyps require a prompt histopathological evaluation and follow-up. Good operative characteristics stand in polyps ⩾10 mm and left sided located. NBI formal training is recommended in gastroenterology units in Latin America.
Plain language summary
Most colorectal cancer are developed from polyps. A proper polyp evaluation is required to orientate which polyp could be a potential neoplasia. However, a definitive diagnosis is made according to histopathology evaluation. On the other hand, Narrow-Band imaging International Colorectal Endoscopic (NICE) classification based on colonoscopy could predict neoplastic polyps and drive therapeutic decisions. Our tertiary center study in Colombia evidence that NICE classification predicts adequately neoplastic polyps but is suboptimal to categorize low risk polyps. Therefore, histopathology polyp evaluation should be still recommended and NBI formal training is recommended in gastroenterology units in Latin -America.
Introduction
Colorectal cancer is the third most incident neoplasia worldwide and the second in mortality. 1 In Colombia, colorectal cancer is the third in incidence and the fifth in mortality. 1 Colonoscopy screening programs have shown to reduce the risk of colorectal cancer at 10 years 2 , in those programs with higher rates of adenoma screening and resection have shown to reduce the risk of death from colorectal cancer. 3
However, biopsy taken during colonoscopy may be associated with adverse events and higher costs.4,5 Therefore, endoscopic alternatives for polyp evaluation are under study. Narrow-Band Imaging International Colorectal Endoscopic (NICE) classification predicts neoplastic polyps based on color, vessels and surface patterns evaluated through a Narrow-Band Imaging (NBI) tool during colonoscopy. 6 Although multiple studies have evaluated NICE and malignancy concordance,7,8 there is scarce data regarding NICE histopathology prediction in South America. 9
This study aimed to determine the concordance between NBI and histopathology and NBI and neoplasia in a cohort of patients managed in a reference hospital in Colombia.
Methods
An analytical prospective cohort study was conducted. Patients who consulted the gastroenterology unit of the Hospital Universitario San Ignacio (Bogota, Colombia) for a colonoscopy between December 2021 and February 2022 were evaluated. Consecutive cases were invited to participate and enrolled once informed consent was signed. Inclusion criteria were patients older than 18 years with a polyp detected and resected during the colonoscopy with biopsy forceps or with polypectomy snare. Patients with polyps and inflammatory bowel disease diagnosis were also included in the study. 10 Exclusion criteria were patients in which a complete colonoscopy could not be completed, familiar adenomatous polyposis, coagulopathy, or pregnancy. An informed consent was filled before colonoscopy.
Sociodemographic data and clinical characteristics were systematically collected during patient care using standardized forms. Hospital Universitario San Ignacio Gastroenterology Unit has eight gastroenterologists who perform colonoscopy on a regular basis. Polyps were evaluated on real time during the procedure. Gastroenterologist performed the description of the characteristics of the polyps, the evaluation of the location, the resection and the classification according to the NICE classification. Histopathology evaluation was performed by a pathologist specialized in gastroenterological pathology according to the World Health Organization criteria. 10 Pathologist was not blinded for colonoscopy report. Each lesion was identified as a Hyperplastic polyp (HP), Sessile serrated polyp (SSP), adenoma, superficial submucosal carcinoma, or deep submucosal invasive cancer (DSIC, carcinoma extension ⩾ 1000 μm of submucosal invasion) (see Figure 1, flow-diagram).

Flow diagram of the patients included in the study.
NICE and histopathology concordance was evaluated according to Japan Gastroenterological Endoscopy Society Consensus. 6 NICE type I corresponded to HP or SSP, NICE type II corresponded to all adenomas with either low or high grade dysplasia, and NICE type III corresponded to DSIC.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cohort studies (Supplemental Material) 11
Sample size
H0 was defined as no concordance between NICE and histopathology classification. H1 was defined as concordance between NICE and histopathology classification. Based on an expected prevalence of 48%, 12 a minimum acceptable agreement of 80%, an expected difference of 10%, an alfa error of 5% and power of 80%, we calculated a sample size of 126 polyps according to Hong normogram for three categorical nominal outcomes 13 Finally considering that our Adenoma Detection Rate was lower than expected we recalculated sample size to 230 polyps.
Statistical analysis
For description of qualitative variables, absolute and relative frequencies were used. Central tendency and dispersion measures were calculated for quantitative variables. Mean and standard deviation were described for variables with normal distribution and median and interquartile range (IQR) for variables with non-normal distribution. Normal distribution was evaluated using the Kolmogórov-Smirnov test at a significance level of 5% (p < 0.05).
Concordance between NICE and histopathology was evaluated according to a Fleiss Kappa, a quadratic weighted kappa and a linear weighted kappa. The strength of agreement based on the kappa value was defined as follows: poor, ⩽0.20; fair, 0.21–0.40; moderate, 0.41–0.60; substantial, 0.61–0.80; or excellent, 0.81–1.0. Sensitivity and specificity of NICE I–II versus III compared with the gold standard (DSIC or adenoma/HP-SSP diagnosed by histopathology) were evaluated globally. A subgroup analysis was performed for bigger polyps (size ⩾ 10 mm) and for those located in the left side (rectum, sigmoid and left colon). Additionally, a sensitivity analysis was carried out considering the gastroenterologist experience. Statistical analysis was performed with the statistical program STATA (Stata Statistical Software: Release 16. College Station, TX, USA: StataCorp LLC).
Results
A total of 238 polyps from 135 patients were identified during the study. Median age of included patients was 67 years [Interquartile range (IQR) 58.5–74.5]. A total of 74 (54.4%) were males. A total of 12 (8.8%) had inflammatory bowel disease. Familiar colon cancer history was present in 18 (13.2%) of patients. A total of 82 (60.7%) had 1 polyp, 30 (22.2%) had 2 polyps and 23 (17.1%) had ⩾3 polyps. Of the polyps 38 (16%) were found on rectum, 39 (16.4%) on sigmoid and 19.7% on left colon. A total of 182 (76.5%) were <10 mm (Table 1 and Figure 1). Adenoma Detection Rate (ADR) was 22.4%.
Characteristic of included patients and of polyps in colonoscopy.
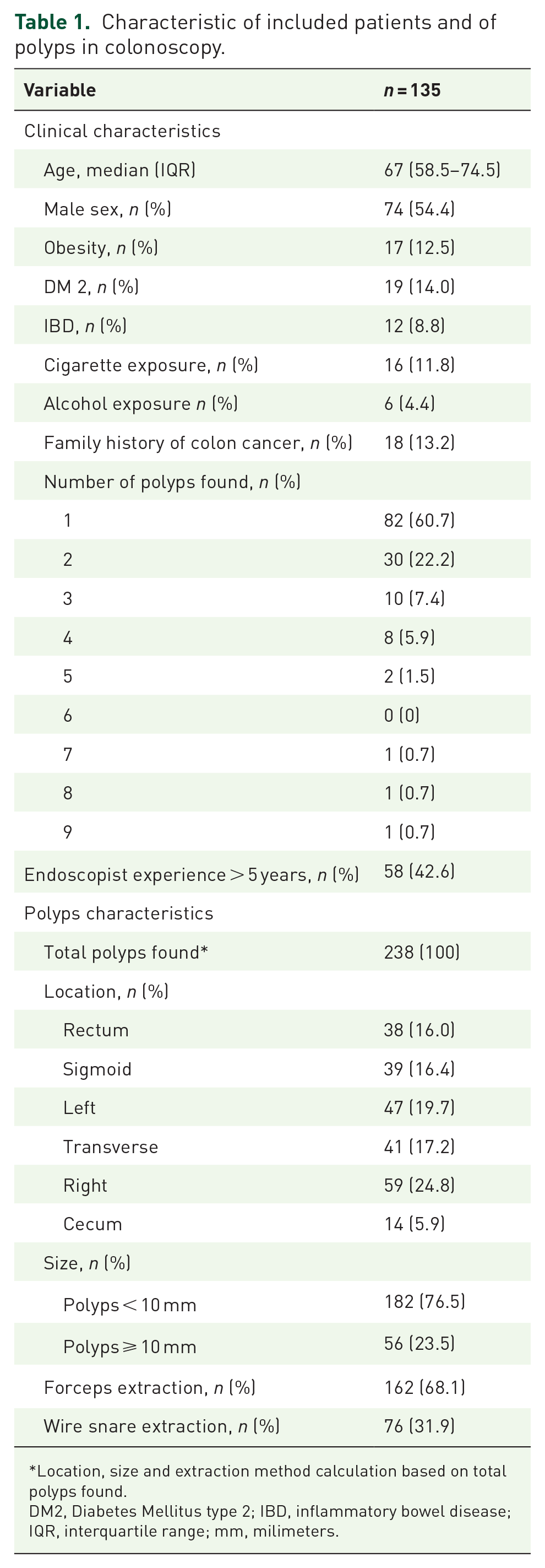
Location, size and extraction method calculation based on total polyps found.
DM2, Diabetes Mellitus type 2; IBD, inflammatory bowel disease; IQR, interquartile range; mm, milimeters.
A total of 130 polyps (54.6%) were classified as NICE I, 96 (40.3%) as NICE II, and 12 (5.0%) as NICE III. By histopathology, 11 polyps (4.6%) had DSIC, and 140 (58.8%) corresponded to adenomas (Table 2).
NICE classification and histopathology concordance on colonic polyps.
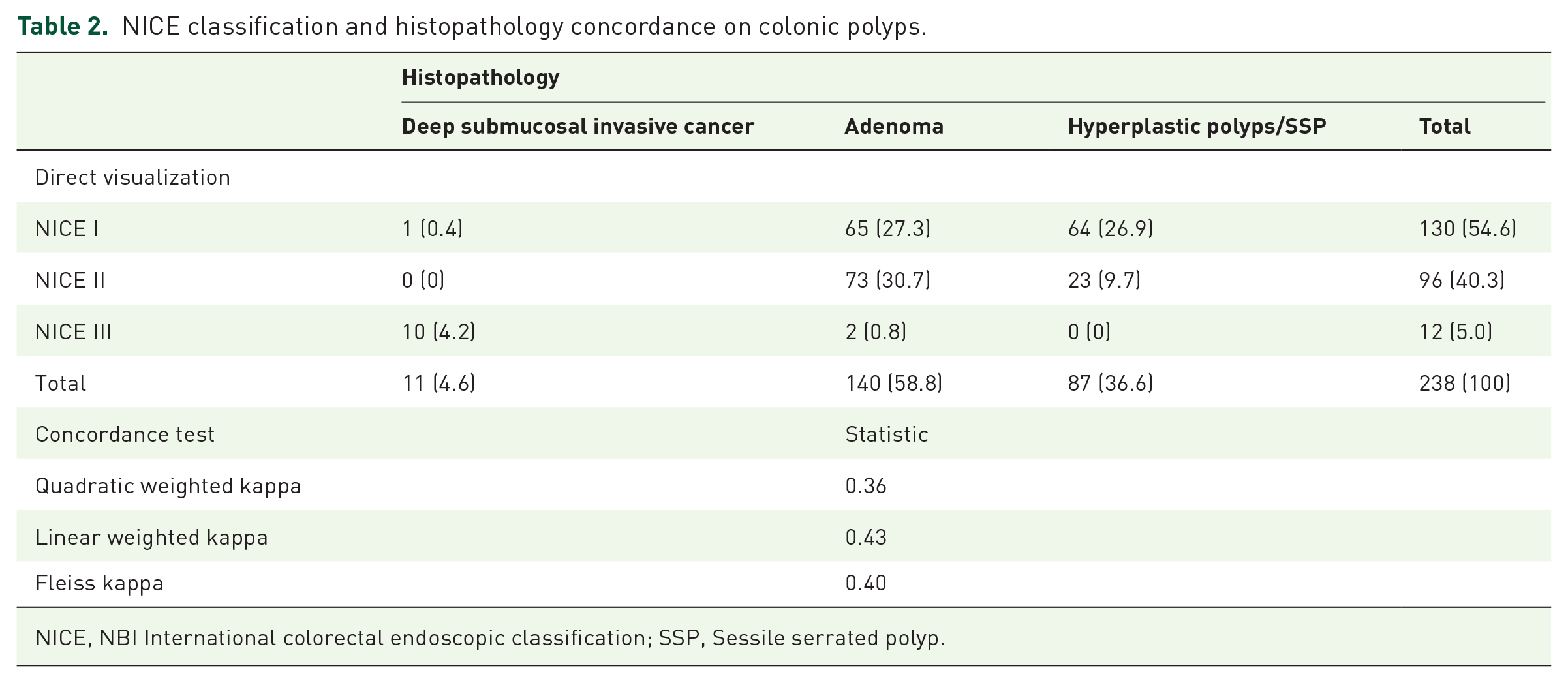
NICE, NBI International colorectal endoscopic classification; SSP, Sessile serrated polyp.
NICE and histopathology evidenced a fair-moderate concordance (quadratic weighted kappa 0.36, linear weighted kappa 0.43). Of polyps classified as NICE I 49.2% correctly corresponded to HP and 50% were adenomas. The polyps classified as NICE II corresponded to adenomas in 76% of cases. The polyps classified as NICE III corresponded to DSIC in 83.3% (Table 2). On the other hand, NICE I–II versus NICE III operative characteristics for DSIC versus adenoma/HP diagnosis had a sensitivity of 90.9% and specificity of 99.1% (Table 3).
Operative characteristics of NICE classification compared to histopathology on colonic polyps.

CI, confidence Interval; NICE, NBI International colorectal endoscopic classification; NPV; negative predictive value; PPV, positive predictive value; SSP, Sessile serrated polyp.
Subgroup analysis evidenced that for polyps ⩾10 mm, the sensitivity and specificity to detect DSIC (NICE I–II versus NICE III) were 100% and 95.7% respectively (Table 4). For left sided located polyps the sensitivity and specificity were 83.3 and 95.2%, respectively (Table 5). Similar operative characteristics values were evidenced according to gastroenterologist experience (sensitivity 100 versus 85.5, specificity 98.4% versus 100% when comparing gastroenterologists with more or less than 5 years of experience) (Supplemental Table 1).
Operative characteristics of NICE classification compared to histopathology on colonic polyps ⩾10 mm.

CI, confidence interval; NICE, NBI International colorectal endoscopic classification; NPV; negative predictive value; PPV, positive predictive value; SSP, Sessile serrated polyp.
Operative characteristics of NICE classification compared to histopathology on left-sided (rectum, sigmoid and left colon) located polyps.

CI; confidence Interval; NICE, NBI international colorectal endoscopic classification; NPV; negative predictive value; PPV, positive predictive value; SSP, sessile serrated polyp.
Discussion
Our study evidence that NICE and histopathology concordance are suboptimal. However, NICE III for DSIC diagnosis evidence good operative characteristics. Therefore, NICE III polyps require a prompt histopathological evaluation and follow-up. Those good operative characteristics stand in polyps ⩾10 mm and in those located in the left side of colon.
Our results evidenced an inadequate NICE and histopathology concordance. Almost 50% of adenomas were classified as NICE I, 26% of HP were classified as NICE II and 9.1% of DSIC were classified as NICE I (Table 1). Other studies have also evidenced suboptimal results for NICE classification.14,15 However, a Japanese study evidenced good operative characteristics for NICE I (specificity 99.6%) and NICE III (specificity 99.6%) classification categories. Therefore, they recommended NICE classification as an adjuvant tool to identify polyps that do not need to be removed or who require prompt histopathological evaluation. 9 We evaluated if the differences between their and our results could be explained by the experience of gastroenterologist but we did not find any association, maybe because NBI formal training was not evaluated in our study and the gastroenterologist experience may not adequately represent the experience with NBI.16–18 Therefore, our findings suggest that in clinical centers without formal NBI training all polyps should be removed endoscopically for histopathology evaluation. Additionally, formal NBI training should be encouraged to improve diagnostic performance with NBI.
On the other hand, NICE III detects DSIC with a sensitivity of 90% and a specificity ⩾99%. A finding similar to that found in other studies. The Japanese study mentioned before evidenced a specificity of 99.6% for NICE III and DSIC. 9 However, other studies have evidenced a lower specificity (81.5%) that varied even between experts (52.2%–96.4%). 7 Therefore, our findings suggest that NICE III polyps are no pathognomonic for DISC. However, prompt histopathological evaluation and follow-up is emphasized in NICE III polyps.
Additionally, NICE III adequately predicts DISC in polyps ⩾10 mm and left sided colon polyps. Specificity in those subgroups was superior to 95%. Puig et al. 19 prospectively evaluated NICE accuracy for polyps ⩾10 mm, finding similar results (sensitivity 58.4%, specificity 96.4%). Hamada et al., 9 in a retrospective study again found similar results (sensitivity 77.8%, specificity 99.4%). On the other hand, although other studies have evidenced that left-sided polyp location is associated with 30% NICE misclassification, a lesser NICE III specificity was found. 15 Therefore, it seems prudent to secure prompt histopathological evaluation in polyps ⩾10 mm and left sided colon polyps.
The prospective methodology of the study, the adequate polyp characterization, and the histopathology evaluation according to gastrointestinal pathology specialists strengthen our study results. However, several limitations should be mentioned: Our study was performed on a single center, and our limited number of T1b cancers limits the precision of our estimations. Therefore, additional studies in Latin America with a higher sample size are recommended to evaluate NICE diagnostic performance. Pathology was evaluated by a single pathologist who was not blinded by colonoscopy report. However, his specialized training in gastrointestinal pathology should limit bias. Additionally, Japan NBI Expert Team (JNET) classification, an excellent method for differential and depth diagnoses of colorectal lesions, was not evaluated in our study. Unfortunately, in our center (and in many Latin American centers), Magnifigyng NBI technology is not available, so our study provides useful information based on locally available technology. Finally, no bowel preparation score was calculated in this study, and ADR was suboptimal. 20 Although both are quality indicators in colonoscopy, it is unclear if there is an association between bowel preparation, ADR and NICE performance.
Conclusion
Our results evidence that NICE and histopathology concordance is suboptimal. However, NICE III for DSIC diagnosis evidence good operative characteristics. Therefore, NICE III polyps require a prompt histopathological evaluation and follow-up. Those good operative characteristics stand in polyps ⩾10 mm and left-sided colon polyps. NBI formal training is recommended in gastroenterology units, both in Latin America and globally.
Supplemental Material
sj-docx-1-cmg-10.1177_26317745241231102 – Supplemental material for Concordance between nice classification and histopathology in colonic polyps: a tertiary center experience
Supplemental material, sj-docx-1-cmg-10.1177_26317745241231102 for Concordance between nice classification and histopathology in colonic polyps: a tertiary center experience by Andrea C. Buitrago-Tamayo, Carlos E. Lombo-Moreno, Valentina Ursida, Ana M. Leguizamo-Naranjo, Oscar M. Muñoz-Velandia and Rómulo D. Vargas-Rubio in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.