
Abstract
Introduction:
The safety and efficacy of colonic band ligation and auto-amputation (1) as adjunct to endoscopic mucosal resection of large laterally spreading tumors and (2) for polyps not amenable to routine polypectomy due to polyp burden or difficult location remain unknown.
Methods:
An institutional review board–approved retrospective single-institution study was undertaken of patients undergoing colonic band ligation and auto-amputation from 2014 to date. Patients with indications of ‘endoscopic mucosal resection for laterally spreading tumors’ and ‘polyp not amenable to snare polypectomy’ were included in the study. Data were collected on patient demographics, colonoscopy details (laterally spreading tumors/polyp characteristics, therapies applied, complications), pathology results, and follow-up (polyp eradication based on endoscopic appearance and biopsy results).
Results:
Patients undergoing endoscopic mucosal resection for laterally spreading tumors: Thirty-two patients (31 males, aged 68 ± 9.17 years) underwent endoscopic mucosal resection-band ligation and auto-amputation of 34 laterally spreading tumors (40 ± 10.9 mm). A median of 2 ± 1.09 bands were placed. Follow-up colonoscopy and biopsy results confirmed complete eradication in 21 laterally spreading tumors (70%). Nine (30%) laterally spreading tumors required additional endoscopic therapy to achieve complete eradication. Four (13%) patients underwent surgery for cancer, and two of them had resection specimens negative for cancer or residual adenoma. One patient suffered post-polypectomy syndrome. Patients undergoing band ligation and auto-amputation for polyps not amenable to snare polypectomy: Seven patients underwent band ligation and auto-amputation due to serrated polyposis syndrome (one patient) and innumerable polyps, or polyps in difficult locations (extension into diverticula: two patients; terminal ileum: two patients; appendiceal orifice: one patient; anal canal: one patient). The patient with serrated polyposis syndrome achieved dramatic decrease in polyp burden, but not eradication. Follow-up in five of the six remaining patients documented polyp eradication. The patient with serrated polyposis syndrome suffered from rectal pain and tenesmus following placement of 18 bands.
Conclusions:
Band ligation and auto-amputation in the colon may be a safe and effective adjunct to current endoscopic mucosal resection and polypectomy methods and warrants further study.
Plain Language Summary
Colonoscopy with rubber band placement to aid in complete removal of large polyps and polyps in technically challenging locations
Colonoscopy is a commonly performed procedure for the early detection of colon and rectal cancer, and prevention through polyp removal.During colonoscopy, sometimes situations are encountered making polyp removal difficult. These can include the presence of larger polyps or the location of a polyp in an area that makes removal technically challenging or high risk.A particularly challenging situation arises when after extensive effort there is still polyp tissue remaining that cannot be removed using routine techniques. We are interested in exploring a technique which involves the placement of a rubber band after sucking a small area of the colon lining into a cap loaded onto the tip of the colonoscope. With time the rubber band strangulates the tissue and falls off along with captured tissue and passes out of the colon naturally.To assess the effectives of this technique we studied patients that have undergone this procedure at our GI unit. We identified 32 patients with 34 large polyps between 4cm to 6cm that we placed rubber bands on polyp tissue after we were unable to completely remove the polyp. On their follow up colonoscopy, complete polyp removal was successful in 21 polyps. We were also able to achieve complete polyp removal in 9 of the remaining large polyps after additional treatment. Four patients underwent surgery because cancer was found in analysis of polyp tissue.In 5 of 6 patients with polyps in difficult locations (e.g. partly within the lumen of the appendix), placement of a rubber band led to complete removal of polyp tissue.Two patients in our study population had mild adverse events that were managed with simple measures.We believe our results show promise for our described technique and this technique should be tested in larger studies.
Keywords
Introduction
Colonoscopy serves as the primary modality for colorectal cancer (CRC) prevention through the removal of pre-cancerous polyps. 1 Certain colon polyp characteristics including large size and location may render polyp removal technically challenging. For example, endoscopic mucosal resection (EMR) of large and laterally spreading tumors (LST) is associated with residual or recurrent adenoma (RRA) in 10–27% of patients2–5 and bleeding in 6–10% of patients.4–8 Risk factors for RRA include lesion size greater than 4 cm, intraprocedural bleeding, piecemeal resection, and prior EMR attempt.2,3,9 Risk factors for post-EMR bleeding include larger and right-sided LST, advanced age, and aspirin use.6–8 Although banding of polyps followed by removal with a snare (band EMR) has been described to aid complete EMR, the technique may have an unacceptably high perforation rate due to capture of the muscularis propria (MP) in the band.10,11 However, the safety and efficacy of band ligation and auto-amputation (BLA; allowing the gradual amputation of the tissue captured in the band) at the time of EMR of LST (EMR-BLA) to prevent RRA have not been evaluated. Similarly, the safety and effectiveness of BLA of polyps extending into colonic diverticula and other locations for example, the appendix and terminal ileum, also require further study. BLA of colon polyps with extension into a diverticulum because snare removal was deemed difficult or hazardous has only been reported in a few case reports.12,13 The purpose of this study is to evaluate the safety and effectiveness of (1) EMR-BLA for complete removal of LST and (2) BLA for complete removal of polyps in difficult locations.
Methods
An institutional review board–approved retrospective search of our endoscopy database from 1 January 2014 to date was undertaken for colonoscopies in which a band was placed. Patients undergoing colonic EMR-BLA for LST and for polyps located in difficult locations not amenable to routine polypectomy were included in the study. Data extracted included patient demographics, colonoscopy examination details, pathology results, and patient follow-up. Colonoscopy details extracted included the indication and site of BLA, the presence of prior endotherapy (biopsy, snare, tattoo, etc.), number of bands placed, and complications. Follow-up included assessment for complications, repeat examination findings in 3–6 months including endoscopic and pathological (biopsy) assessment of BLA site for RRA, and any further interventions performed. Data were analyzed for patients for whom complete follow-up information was available.
BLA technique
Once the decision for EMR-BLA or BLA was made, the colonoscope was removed. A band ligator (MBL-6-XL-C, or MBL-6; Cook Medical, Bloomington IN, USA) was loaded onto the scope (EG-3490K, EC-3490Li, or EC-3890Li; Pentax Medical, Tokyo, Japan) in usual fashion. The image magnifier option was used to magnify the image and limit the impact of the cap blocking the peripheral endoscopic view. The image was enhanced using the i-scan 1 option (surface enhancement) on the Pentax Processor (EPK-i7010; Pentax Medical) to offset the almost universal slight blurriness that appeared to occur while using a scope with a banding kit loaded on it in the colon. Band deployment was performed in standard fashion by suctioning the area of interest/polyp into the cap and releasing the band upon achieving maximum tissue in the cap (read out on screen). The examination was then terminated, and the bands were left attached to allow for gradual amputation.
EMR-BLA of LST
Following exhaustive attempts at complete snare removal of LST, the initial EMR-BLA band was deployed on the area of maximum residual adenoma in the EMR bed with effort to suction as much of the polyp tissue and post-polypectomy bed including muscle into the banding cap (Figure 1). This was done to maximize the tissue captured in the band (giving a mushroom appearance) and thus avoiding tissue slipping out of the band or band slipping off without amputating tissue. Additional bands were placed if there was additional residual polyp visible in the EMR bed. The examination was then terminated, and the bands left were attached to allow for gradual amputation.

EMR-BLA of an LST: (a) an almost hemicircumferential ascending colon LST; (b) flat residual polyp present in EMR bed that was not amenable to snare resection; (c) EMR bed polyp tissue aligned with the banding cap; (d) EMR bed with polyp tissue captured in bands; and (e and f) post-EMR BLA scar with no residual polyp seen 6 months later.
BLA of polyps in difficult locations or polyp not amenable to routine polypectomy due to polyp burden
The polyps were sampled (partial EMR, forceps, or snare) to ensure pathological diagnosis. The BLA technique involved aligning the bottom rim of the bander cap with the lower margin of the polyp, applying suction to maximize polyp tissue in the cap (red out), and then deploying the band. Effort was made to suction the entire polyp or as much of the polyp as possible into the cap prior to band deployment. Additional bands were deployed if there was polyp visible outside the band. The examination was then terminated, and the bands left were attached to allow for gradual amputation.
Follow-up care after EMR-BLA/BLA
Post-colonic EMR-BLA/BLA care did not differ from standard post-endoscopic monitored recovery and assessment prior to discharge. Follow-up examinations to inspect the EMR-BLA site were scheduled within 6 months. Patients returning for follow-up after colon BLA underwent standard colonoscopy examination with emphasis on the area of BLA identification, description (presence of scar, residual adenoma, ulcer, etc.), sampling, and, if appropriate, further therapy.
Statistical analysis
Characteristics of the study cohorts are reported as n (%) for categorical variables and median (range) for continuous variables. A chi-square goodness-of-fit test was used to test whether the frequency of residual polyp following post-EMR BLA differed from randomness. Multivariate logistic regression analysis with forward stepwise selection was performed to assess the association between initial LST characteristics and the odds of residual polyp presence following EMR-BLA. Values of p < 0.05 were considered significant. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (Armonk, NY: IBM Corp.).
Results
EMR-BLA cohort
Thirty-two patients (aged 68 ± 9.17 years; range, 42–90 years) including 31 males underwent EMR-BLA of 34 LST during the study period. The characteristics of the study group are detailed in Supplementary Table 1 and summarized in Table 1. Median size of LST at the time of EMR-BLA was 40 mm (±10.9 mm; range, 20–60 mm), and these were found throughout the colon with no particular location predominance. Most (24; 70.6%) of the LST were previously diagnosed and referred for EMR, and the majority (25; 73.5%) had previously been sampled or undergone attempted endoscopic removal. Thirty (88.2%) of 34 LST had endoscopically visible residual polyp at the time of EMR after exhaustive attempts for complete removal with snare. EMR-BLA involved placement of 1–5 bands (median, 2 ± 1.09) per EMR bed for a total of 72 bands. Muscle capture in the band was evident in all post-EMR cases (Figure 1). Four patients underwent surgery for the indication of malignant pathology results. An EMR-BLA site scar with negative pathology on scar biopsies was achieved in 21 of the remaining 30 LST (70%) (Figure 1). Nine LST underwent additional endoscopic therapy (see Supplementary Table 1 and Table 1 for details) for residual polyp in the EMR-BLA site on follow-up examination. Ultimately, a post-endoscopic therapy scar with negative final pathology was achieved in all 30 LST without invasive cancer. Two of four lesions with cancer on index EMR-BLA (one T1b well-differentiated adenocarcinoma [WD-CA] and one invasive moderately differentiated adenocarcinoma [MD-CA]) had no evidence of cancer or residual polyp in the surgical specimen. In the case of a rectal T1b WD-CA, the post-EMR-BLA scar was identified in the rectal MP, suggesting EMR-BLA led to partial auto-amputation of the MP (Figure 2). One patient suffered post-polypectomy syndrome, likely due to transmural burn secondary to snare cautery use.
Patient and clinical characteristics including procedure outcomes for the post-EMR-BLA cohort.

APC, argon plasma coagulation; BLA, band ligation and auto-amputation; EMR, endoscopic mucosal resection; FIT, fecal immunochemical test; LST, laterally spreading tumors; MD-CA, moderately differentiated adenocarcinoma; SSA, sessile serrated adenoma; TA, tubular adenoma; TVA, tubulovillous adenoma; TVA-HGD, tubulovillous adenoma with high-grade dysplasia; WD-CA, well-differentiated adenocarcinoma.
Demographics and clinical characteristics of patients undergoing BLA of polyps not amenable to routine polypectomy.

APC, argon plasma coagulation; BLA, band ligation and auto-amputation; EMR, endoscopic mucosal resection; ICV, Ileocecal valve; SCAD, segmental colitis associated diverticulosis; SSA, sessile serrated adenoma; TA, tubular adenoma; TI, terminal ileum; TVA, tubulovillous adenoma.
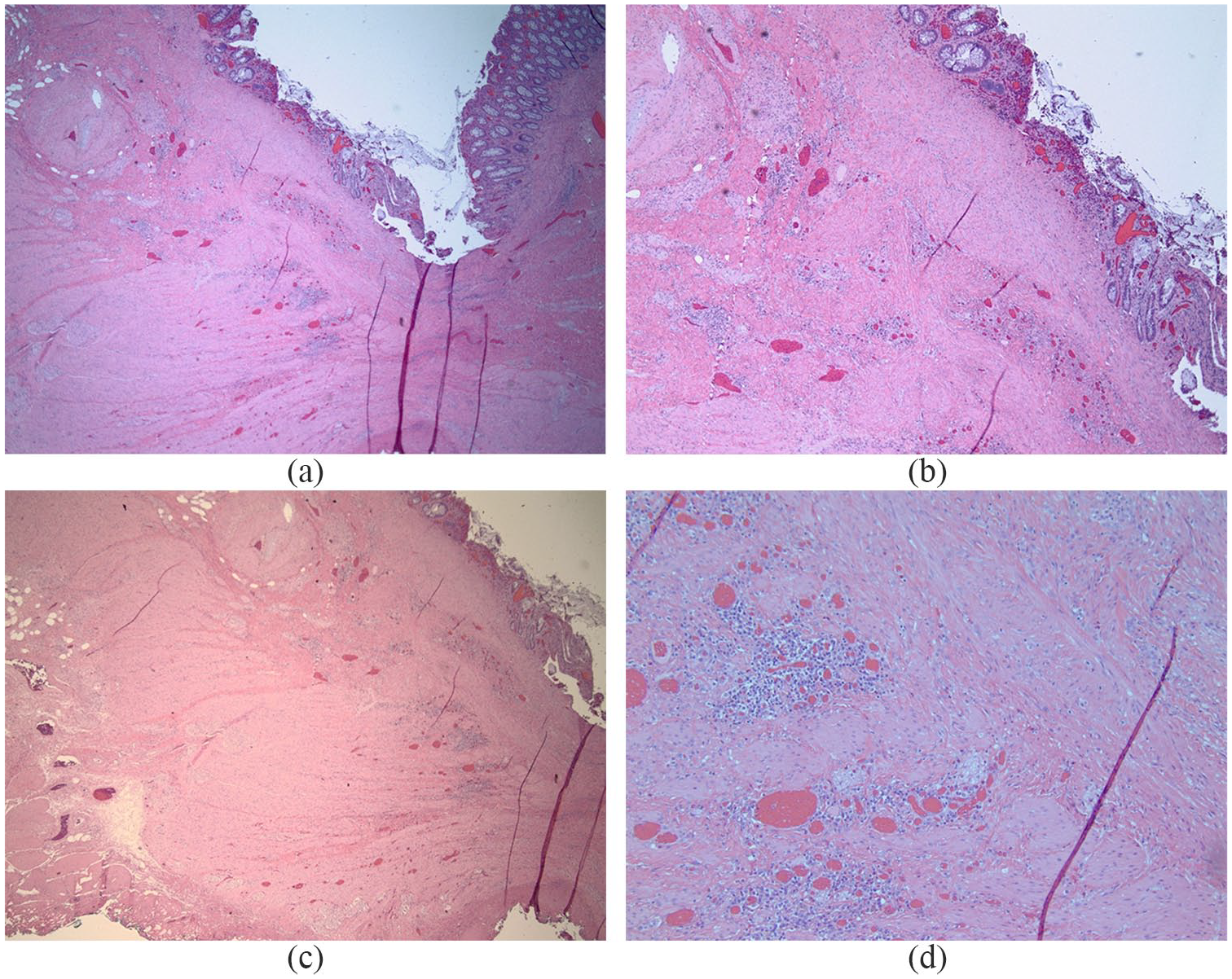
Images of histopathological changes in EMR-BLA site of T1b rectal adenocarcinoma in surgical specimen: (a, b and c) prominent scar tissue and mild chronic inflammation involving mucosa, submucosa, and superficial layers of muscularis propria; deeper layers of muscularis propria are not involved by scar tissue. No residual adenocarcinoma is seen (4×). (d) Scar tissue involving superficial layers of muscularis propria (10×).
Characteristics contributing to LST EMR-BLA residual polyp presence
A chi-square goodness-of-fit test was used to test whether the frequency of residual polyp following EMR-BLA of LST differed from randomness. Expected frequencies in all cells were greater than 5. Visible residual polyp differed statistically from no visualized polyp, χ2(1, N = 31) = 9.323, p = 0.002. A multivariate logistic regression was performed in an effort to identify factors associated with the odds of residual polyp following EMR-BLA of LST. Overall, logistic modeling was not significant (p = 0.08) and did not identify a discrete factor contributing to residual polyp following EMR-BLA.
BLA patient cohort with polyps not amenable to routine polypectomy
Seven patients (Table 2) underwent BLA of polyps due to either serrated polyposis syndrome (SPS) with innumerable and confluent polyps (one patient) or polyps in difficult locations with extension into diverticula (two patients), terminal ileum (two patients), appendiceal orifice (one patient [Figure 3]), and anal canal (one patient). The patient with SPS and innumerable polyps was not deemed a surgical candidate due to multiple severe comorbidities and had multiple BLA procedures (a total of 67 bands placed) with a dramatic decrease in polyp burden but incomplete eradication. He suffered from rectal pain and tenesmus following the index BLA procedure with placement of 18 bands in the rectum and sigmoid colon. Thereafter, he was able to tolerate up to 12 bands per session, but ultimately passed away due to unrelated causes. Post-BLA scarring did make subsequent band placements difficult in this patient. Two patients with multiple large sessile serrated adenoma (SSA) in the setting of dense sigmoid diverticulosis also had multiple bands placed (5 and 12 bands, respectively), leading to post-BLA scars and negative pathology. Three patients with polyp extension into the terminal ileum and appendix (Figure 3) also achieved polyp eradication, and one patient with a hyperplastic polyp extending into the anal canal was not scheduled for follow-up examination following BLA. A total of 92 bands were placed in this cohort during 11 BLA procedures.

BLA of an appendiceal orifice polyp: (a) appendiceal orifice polyp with extension into the appendix; (b) submucosal lift performed pre-EMR; (c) after partial EMR, the ‘intra-appendiceal’ portion of the polyp is suctioned into the cap and a band deployed; and (d) a scar is seen at the BLA site with obliteration of the appendiceal lumen on 6-month follow-up examination.
Discussion
Piecemeal EMR of LST is associated with risk of RRA in 10–27% of patients and bleeding in 6–10% of patients.2–8 The use of argon plasma coagulation (APC) as an adjunct to piecemeal EMR has been shown to decrease the RRA rate but is far from perfect and associated with complications including bleeding and injury to the muscle layer.14–18 More recently, hot avulsion of RRA has been suggested to be superior to piecemeal EMR alone or a combination of APC and piecemeal EMR in RRA eradication, 19 but still relies on the application of heat therapy. A widely available technique that does not require additional expertise or training by endoscopists and can be used to safely and effectively eradicate residual polyp at the time of EMR of LST is desirable. Our data suggest that BLA may fulfill such a need. Due to routine exposure to band ligation of esophageal varices, gastroenterologists are familiar with the technique of BLA. However, the existing data regarding BLA in the colon are limited to case reports of BLA of polyps in diverticula.12,13 An ex vivo study has described capture of the MP in bands especially if deployed proximal to the left colon; thus, band-assisted EMR in the colon may have an unacceptably high perforation rate.10,11 In this retrospective study of over 160 bands placed in the colon of 39 patients for various indications, we show that BLA is safe, despite MP capture in the band at the time of EMR-BLA of LST, raising the possibility that BLA may safely lead to MP auto-amputation. EMR BLA also led to complete eradication of adenomatous tissue in 70% of LST following one EMR-BLA session in a cohort of patients with visible polyp in the EMR bed following exhaustive attempts at snare removal and contributed to complete polyp eradication on follow-up examination in all non-cancerous LST. These data suggest that BLA could play a role as an adjunct to EMR of LST. Randomized studies comparing BLA with APC and avulsion are required to compare the effectiveness and safety profile of each technique in decreasing RRA following EMR of LST. We also expand on the existing data of BLA of polyps in difficult locations and show that these polyps can be band-ligated and left to safely auto-amputate in areas traditionally felt to be higher risk of perforation with snare techniques (e.g. diverticula).
There are multiple subjective and objective advantages and limitations of BLA using current banding devices. First, after a prolonged examination with exhaustive attempts at piecemeal EMR of LST and visible residual polyp, the ‘bail-out’ option of placing a band on the recalcitrant area is attractive because it avoids the application of thermal injury to the EMR bed and does not require any additional skill by the endoscopist. However, all current banding devices are of the over-the-scope variety, which leads to the cumbersome process of having to remove the scope from the patient to load the banding device and then re-insert the scope to the EMR bed for BLA. This can be time-consuming, and although no complications were identified in this study, consideration must be given to potential risks of scope re-insertion and insufflation after creating an EMR defect in the colon and additional sedation/anesthesia duration. The availability of a through-the-scope banding device would remove these concerns. An additional limitation of BLA is the non-availability of the auto-amputated tissue for pathological evaluation, which is similar to other ablative techniques (e.g. APC). As such, it is important to adequately sample any lesion considered for BLA to confirm the degree of dysplasia present. Recent techniques such as endoscopic submucosal dissection20–22 and endoscopic full-thickness resection23,24 have the advantage of providing complete histological evaluation of an LST. Unfortunately, these techniques are not yet widely available and also have a significant perforation rate.20–24 We believe that BLA may be appropriate as an adjunct to benign LST EMR to reduce the rate of incomplete removal in the same way APC or avulsion is being used. If post-EMR-BLA pathological analysis of an EMR specimen reveals cancer, further intervention including surgical resection should be considered.
Our study has several limitations which include its single-center, retrospective cohort design. Due to the study design, we do not have a comparison group (e.g. EMR of LST without BLA and with APC) and were also unable to calculate the additional time required to perform EMR-BLA over EMR alone. The strengths of this study include (1) the first description of EMR-BLA in a series of patients with LST with follow-up data and (2) the safety profile of colonic BLA for a variety of indications in the largest report of its kind to date.
Supplemental Material
sj-pdf-1-cmg-10.1177_26317745211001750 – Supplemental material for Safety and efficacy of band ligation and auto-amputation as adjunct to EMR of colonic large laterally spreading tumors, and polyps not amenable to routine polypectomy
Supplemental material, sj-pdf-1-cmg-10.1177_26317745211001750 for Safety and efficacy of band ligation and auto-amputation as adjunct to EMR of colonic large laterally spreading tumors, and polyps not amenable to routine polypectomy by Stephanie Romutis, Bassem Matta, Jonathan Ibinson, John Hileman, Smiljana Istvanic and Asif Khalid in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
Author contributions
S.R. was involved in data analysis, drafting, and final approval of the manuscript and was accountable for all aspects of the work presented herein. B.M. was involved in the data acquisition and analysis, drafting, and final approval of manuscript and was accountable for all aspects of the work presented herein. J.I. was involved in data analysis and final approval of the manuscript, and was accountable for all aspects of the work presented herein. J.H. was involved in study design, data acquisition, and final approval of the manuscript and was accountable for all aspects of the work presented herein. S.I. was involved in data acquisition and analysis and final approval of the manuscript, and was accountable for all aspects of the work presented herein. A.K. was involved in study conception, design, data acquisition and analysis, drafting, and final approval of the manuscript and was accountable for all aspects of the work presented herein.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.