
Abstract
Objective
To compare the ability to detect colonic polyps using a modified Mayo Clinic (MMC) barium enema technique with that of the usual gold standard optical colonoscopy (OC).
Methods
Patients considered at an average or increased risk of colorectal cancer were initially screened using the MMC technique. Patients who refused OC, those who had isolated rectal lesions and those with incomplete OC were excluded. Patients with mass lesions in the right colon or left colon were further assessed using OC.
Results
A total of 142 consecutive patients were examined using the MMC technique. Of these, 18 patients were found to have mass lesions in the right or left colon and were further evaluated using OC. Sensitivity and specificity of the MMC technique for detecting colonic polyps/cancers of ≥0.3 cm were 87.5% and 80.0%, respectively. Most significantly, for detecting polyps of ≥1.0 cm, the false-negative rate was 0%.
Conclusions
The MMC technique may provide an alternative screening method to OC for the detection of colorectal polyps, particularly in countries where resources are scarce.
Introduction
When evaluating the effectiveness of an imaging technique, the result of the detection of colonic polyps is sometimes reported as a false-negative rate and occasionally as a detection rate. The false-negative rate is used when specificity cannot be obtained in a reasonable and ethical manner, such as when an invasive procedure is required to confirm negative results (i.e. normality) in the patients being studied. The sensitivity of a diagnostic test can be deduced by subtracting the false-negative rate from 1.0 (or 100%). The detection rate is the percentage of patients confirmed to have colonic polyp(s) out of the entire study group that was examined. The detection rate is of limited value if the incidence of colonic polyps in the population of interest is not known. However, it is very useful when comparing the efficacy of two or more imaging modalities in a single population or in multiple similar populations. The false-negative rate of optical colonoscopy (OC) for detecting colorectal polyps was 28% in a recent prospective multicentre study. 1 There is evidence to suggest, based on the records at a cancer registry, that there is an even higher false-negative rate in the right colon. 2
Unfortunately, high false-negative rates or low detection rates for detecting colorectal polyps/cancers of ≥1.0 cm also plague other colonic imaging modalities. For example, computed tomography colonography (CTC) and magnetic resonance colonography (MRC) both have a false-negative rate of 10–12% for detecting polyps of ≥1.0 cm and a higher false-negative rate for polyps of ≥0.3 cm.3,4 The false-negative rates of the usual variety of double-contrast barium enema (DCBE) and high-density DCBE vary widely. DCBE is generally believed to be the most sensitive radiological method in detecting colonic polyps. However, a study of a group of 104 patients, all of whom had negative DCBE, reported that >50 sub-centimetre polyps had been detected and removed from the patients. 5 This was indicative of a false-negative rate for DCBE of 100% for the detection of colonic polyps of ≤0.9 cm in the patients in this study. 5 In addition, both types of DCBE are very unpleasant procedures and are poorly tolerated by patients. The commonly used variety of single-contrast barium enema (SCBE) and high-voltage SCBE have very low detection rates for polyps of all sizes.6,7 Combined DCBE and SCBE is useful in only a very small proportion of patients. 8 Capsule endoscopy has a sensitivity of 88% (equivalent to a false-negative rate of 12%) for detecting colorectal polyps of ≥1.0 cm. 9 The swallowed capsule may not be excreted for as long as 10 h.9,10 An exception is a little known technique used at the Mayo Clinic in Rochester, MN, USA, 11 which consists of an SCBE with continuous fluoroscopy and vigorous manual palpation of the colon in the profile projection (with the hand of the examiner for palpation inside a lead glove). The false-negative rate of the Mayo Clinic technique in detecting colonic polyps of ≥0.3 cm in 1500 patients was 6% and the authors reported that “All 29 polyps 1 cm or larger were seen on barium enema.” 11 This finding indicated a false-negative rate of 0% for detecting colonic polyps of ≥1.0 cm.
In view of the recently established high false-negative rate of OC1,2 and the drawbacks of the other colonic imaging modalities, this present study was undertaken to test the hypothesis that whenever OC cannot be easily or promptly undertaken, the modified Mayo Clinic (MMC) technique can offer a reasonable alternative for the detection of colonic polyps.
Patients and methods
Patient population
The design of this prospective study followed the STARD recommendations. 12 Consecutive patients examined at Chinatown X-Ray & Ultrasound, Vancouver, BC, Canada were enrolled in the study between 9 May 2012 and 13 September 2012. If necessary, translation from English to the patient’s native language was undertaken by the examiner, a staff member or a relative who was fluent in that language. In the first stage of selection, all adults ≥18 years old at an average or increased risk of colorectal cancers were enrolled in the study (e.g. family history of colorectal cancer, positive faecal immunochemical test [FIT], change in bowel habits, rectal bleeding, abdominal pain). No patients had a known diagnosis of inflammatory bowel disease, which would be a cause for exclusion. Pregnancy and referral from hospitals/nursing homes/correctional institutions were also reasons for exclusion. Ethics permission was not applied for because the technique (barium enema) is firmly established and is still currently in use in many countries worldwide. Written informed consent was obtained from each study participant.
Imaging technique
Patient preparation consisted of ingestion of a clear liquid diet and oral polyethylene glycol 3350 (Colyte®; Alaven Pharmaceutical, Marietta, GA, USA) colonic lavage on the day prior to the examination. A barium suspension of 35% W/V (E-Z-EM Polibar Plus 105% W/V diluted with water; E-Z-EM, Lake Success, NY, USA) was used as the contrast medium. The fluoroscopic unit was a GE Advantx® RF system with a Digital Radiography System (GE Healthcare, Milwaukee, WI, USA). This system replaced the use of radiographic films. Images were stored in and retrieved from computer systems. The examination used the MMC technique, which was an adaptation of the Mayo Clinic technique to make it less strenuous for the examiner. More importantly, a limited DCBE that mainly targeted the rectum was added, rendering the supplementary proctoscopy in the original technique unnecessary. The MMC technique began with an examination of the left colon (splenic flexure through to the rectum). A digital rectal examination was performed with the patient in the left decubitus position. Barium suspension was then administered rectally by drip infusion to just beyond the splenic flexure. Under intermittent fluoroscopy, meticulous inch-by-inch deep compression with a radiology pneumatic compression paddle was applied to the left colon in the profile projection. The compression is deep enough that the anterior wall briefly ‘kisses’ the posterior wall. The sigmoid colon was also compressed in the oblique projections. A limited DCBE was later performed targeting mainly the rectum (see below). For examining the right colon (caecum through to the transverse colon), barium suspension was further administered to just beyond the hepatic flexure. Inch-by-inch deep compression was similarly applied to the right colon. In most patients, there was insufficient barium suspension in the caecum at this stage. Ancillary compression of the caecum was later performed (see below). Spot images were obtained for documentation if lesions were detected or for further viewing if suspicious changes were seen. The colon was drained briefly and air introduced until the sigmoid was optimally distended. Intentional distension of the right colon was not undertaken. Oblique spot images of the sigmoid were optionally obtained. The fluoroscopic table was tilted to just short of the upright position and an en face spot image of the splenic flexure routinely obtained. This was undertaken because compressing this segment can often be difficult. The table was then lowered to 30° above the horizontal, ancillary compression of the caecum was performed in the profile and oblique projections. The table was returned to the horizontal position and the patient turned to the left decubitus position. Brief fluoroscopy was used to see if there was excess barium suspension in the rectum. If present, the suspension was drained and air reintroduced. The patient was then turned to the prone position for overhead images. These included a caudad angled view of the recto-sigmoid, a cross-table lateral view of the rectum and both decubitus views of the abdomen with the entire rectum included in the field of view. A postevacuation image was obtained at the discretion of the examiner.
The maximal diameters of any right or left colonic mass lesions were obtained by comparing with a 1.0 cm metal bar at a level 10 cm above the table top of the fluoroscopic unit. All colonic mass lesions were measured on the spot images. Rectal mass lesions were measured on the overhead images. When the lesion was seen in two or more images, the measurement was made in the image with the least magnification. In the second stage of selection, patients who refused OC or those who had isolated lesions in the rectum were excluded from the study. Patients with mass lesions in the right or left colon (except the rectum) were further assessed using OC as the gold standard. If the MMC imaging was indicative of ‘carcinoma’, then the subsequent OC was performed within 2–3 weeks by the gastroenterologists at either St Paul’s Hospital, Vancouver, BC, Canada or Vancouver Hospital & Health Sciences Centre, Vancouver, BC, Canada. If the MMC imaging was indicative of a polyp (irrespective of size), the OC was usually performed within 6 months and very occasionally 9 months. However, patients on the waiting list for OC who just had a positive FIT result waited approximately 12–15 months for their OC examination. In the third stage of selection, patients who had an incomplete OC were also excluded from the analysis.
The pain level experienced by the patient during the procedure was assessed using a 0–10 verbal pain scale (0 = no pain, 10 = maximum pain). The level was ascertained and recorded by the examiner just prior to evacuation. Any complaints or positive comments made by the patient were also recorded by the examiner.
Statistical analyses
The detection rate of polyp/cancer of ≥0.3 cm and the false-negative rate of polyp/cancer of ≥1.0 cm were calculated manually. For statistical analysis regarding polyp/cancer of ≥0.3 cm, the MedCalc program, version 13.1 (MedCalc Software, Ostend, Belgium) was used. Diagnostic test evaluation was undertaken using the MedCalc program. Fisher’s exact test with Yates’ correction was used to compare frequencies. A P-value <0.05 was considered statistically significant.
Results
A total of 142 patients were examined using the MMC technique. The median age was 60 years and the mean age was 61.3 years (range 18–96 years). Forty-four (31.0%) patients commented there was little discomfort and stated they were very satisfied with the procedure. There were no complaints from the patients about the procedure. Twenty-six (18.3%) patients were found to have colorectal mass lesions of ≥0.3 cm using the MMC technique. Four patients refused OC and three patients with isolated rectal mass lesions were excluded. One patient with an incomplete OC was also excluded. Eighteen patients underwent complete OC (Figure 1). Fourteen of these patients were confirmed by OC to have polyp/cancer of ≥0.3 cm in the colon (excluding the rectum); this was the equivalent of a 9.9% detection rate (14/142). All seven polyps of ≥1.0 cm confirmed by OC (in addition to two cancers) were detected with the MMC technique.
Patient enrolment, inclusion and exclusion process. OC, optical colonoscopy.
Location and size (maximum diameter in cm) of the colonic mass lesions detected by a modified Mayo Clinic (MMC) technique compared with standard optical colonoscopy (OC) in patients (n = 18) who participated in a study to investigate whether the MMC technique offers an alternative to OC for the detection of colonic polyp/cancer.
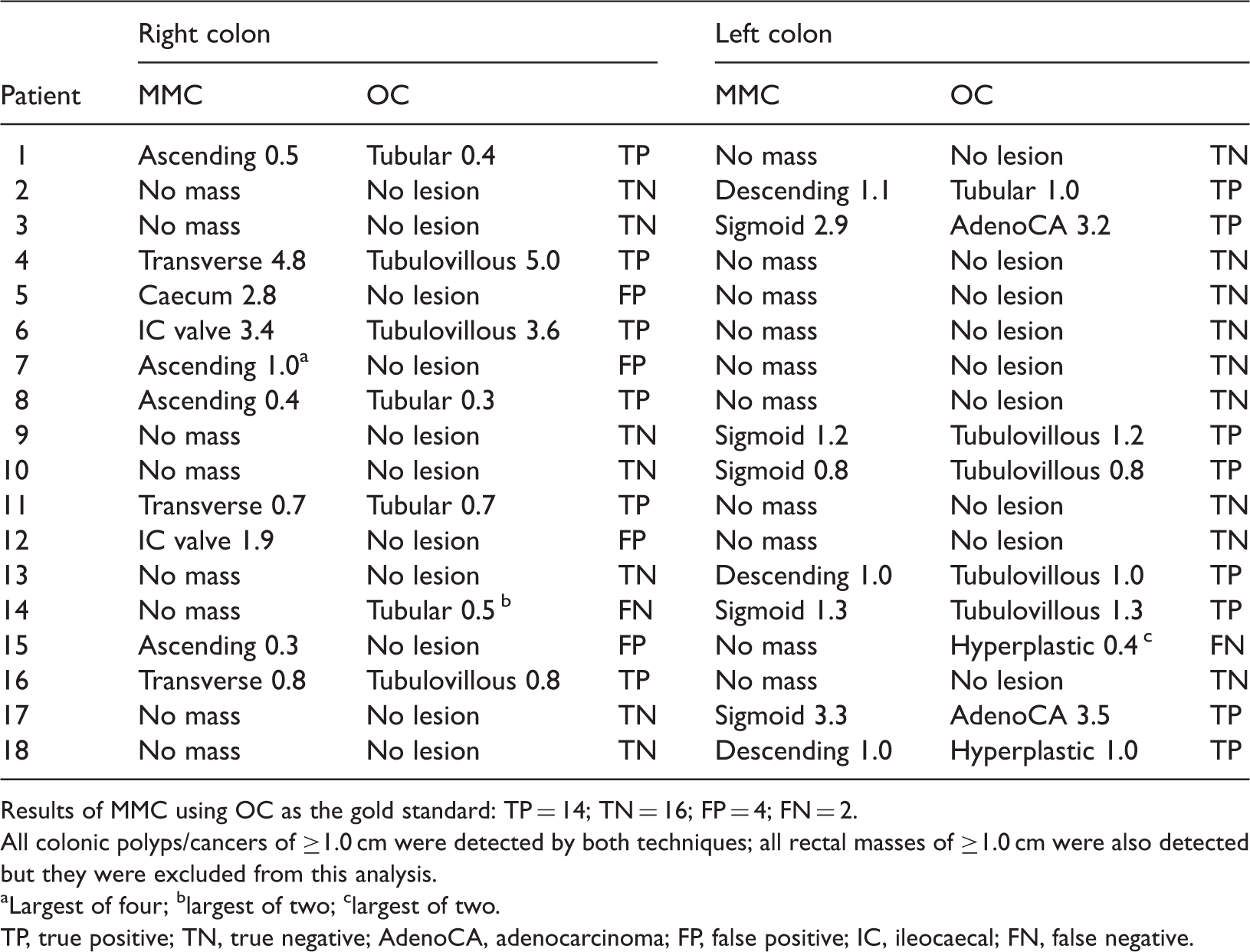
Results of MMC using OC as the gold standard: TP = 14; TN = 16; FP = 4; FN = 2.
All colonic polyps/cancers of ≥1.0 cm were detected by both techniques; all rectal masses of ≥1.0 cm were also detected but they were excluded from this analysis.
Largest of four; blargest of two; clargest of two.
TP, true positive; TN, true negative; AdenoCA, adenocarcinoma; FP, false positive; IC, ileocaecal; FN, false negative.
Discussion
Colorectal cancer is the second leading cause of death from cancer in North America.13,14 Evidence supports the progressive nature of genetic alterations during tumorigenesis in colorectal cancers. 15 It has been estimated that it takes 5 years for normal colon to develop a precancerous polyp and 5 more years for it to develop into invasive cancer. 16 The long time-interval suggests that colon cancer can be prevented by locating the colonic polyps followed by removal at a time before degeneration into invasive cancer. The size of the colonic polyp is a major factor associated with malignant potential.17,18 If the location, size and shape (sessile or pedunculated) of a colonic polyp are clearly defined with an imaging method that has a low false-negative rate, this can facilitate the selection of the most appropriate diagnostic or interventional procedure as well as the most fitting time for the patient. An optimal imaging method should have the following qualities: (i) false-negative rate of 0% for detecting polyps/cancers of ≥1.0 cm; (ii) low cost; (iii) low complication rate; (iv) short preparation time; (v) no parenteral medication/contrast agent required; (vi) no or low radiation; (vii) short recuperation time; (viii) low levels of discomfort; (ix) well tolerated by patients; and (x) it can be easily mastered by junior doctors (i.e. radiology residents).
In the present study, the false-negative rate of the MMC technique for detecting colonic polyps of ≥1.0 cm was 0% in patients in whom their right and left colons were further scrutinized by OC. Thus, the previously reported false-negative rate of 0% for detecting colonic polyps of ≥1.0 cm using the original Mayo Clinic technique has been reproduced with the MMC technique used in the present study. 11 The detection rate of the MMC technique was somewhat lower than the much acclaimed detection rate of 12.5% (3101/24 783 patients) achieved using the Malmö technique, which was identical to the incidence of polyps/cancer determined at autopsy by a study undertaken in Malmö, Sweden. 19 However, the four patients who refused OC in the present study may have had polyp/cancer of ≥0.3 cm. Taking the sensitivity of the MMC technique of 87.5% into consideration (87.5% of four patients = 3.5), the calculated detection rate is 12.3% (i.e. [14 +3.5]/142). This is comparable with that of the Malmö technique. 19
The estimated total cost of the MMC technique is about one-eighth of OC and about one-fifth of CTC in British Columbia; the actual total cost is not known as the technical component of the fees paid to the local hospitals by the healthcare system is not published and is not readily accessible. OC, CTC, MRC and capsule endoscopy may require a 2- or 3-day preparation time, whereas a 1-day preparation is adequate for the MMC technique. There is often excess fluid in the colon after oral polyethylene glycol 3350 lavage.20,21 Excess fluid in the colon adversely affects imaging examinations of the colon except dark-lumen MRC 4 and the MMC technique. On the contrary, excess fluid decreases the density of the barium suspension in the right colon and tends to lessen the effort required in examining the caecum and ascending colon. No intravenous contrast or parenteral medication is necessary for the MMC technique. The radiation dose is estimated to be comparable with or lower than low-dose 64-slide CTC. It is common knowledge that some patients find colonic examinations unpleasant. Only rarely do they voice satisfaction about the test. The low score in the verbal pain scale and the large number of patients who related positive comments about the examination provided strong evidence that the discomfort level was low and the test was well tolerated by the patients examined using the MMC technique in this present study. The MMC technique can easily be mastered by radiology residents. Many of the examinations using the original Mayo Clinic technique were performed by radiology residents. Technically, the MMC technique should be far easier to master than the commonly used DCBE or high-density DCBE. In addition, the MMC technique may well be the present-day answer to the question – What next? – posed in 2008 by Rex (Indianapolis, IN, USA). 22 The ultimate imaging test for colonic polyp/cancer in the future may be a variety of positron emission tomography/magnetic resonance imaging scan, but the radionuclide will need to have a suitable half-life and be able to enhance adenomatous polyps and carcinoids without enhancing normal colonic mucosa or inflammatory polyps; hyperplastic and hamartomatous polyps are enhanced only if high-grade dysplasia is present. However, the time required to develop a radionuclide with these properties may be ≥50 years.
In conclusion, the MMC technique may provide an alternative screening method for the detection of colorectal polyps. This may be advantageous where there are ever-increasing healthcare costs and long waiting lists for OC, as in Canada, as well as in developing countries where there is a paucity of gastroenterologists and CT scanners. Further studies are required, but if a comparable false-negative rate for detecting colonic polyps of ≥1.0 cm can be reproduced consistently, then the widespread use of this technique might plausibly bring about a significant reduction in the number of deaths from colon cancer in North America, and perhaps in developing countries as well.
Footnotes
Declaration of conflicting interest
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Acknowledgements
I wish to thank Dr Thomas S Wong for his inspiring inducement and Dr Anthony W Chow for his assistance in the statistical analysis of the data.